
Abstract
Objective:
To identify the challenges and facilitators for implementing a 24-h telephone cancer service.
Data sources:
English language articles were retrieved from Medline, Cumulative Index of Nursing and Allied Health Literature, and Ovid Nursing electronic databases published from 2000 to 2015.
Study Design:
The authors performed an integrative literature review. The qualitative and quantitative articles were evaluated using the Critical Appraisal Skills Program. All mixed-methods articles were evaluated using the Mixed Methods Appraisal Tool. Thematic analyses were used to synthesize the findings from the included articles.
Findings:
The literature of this review highlights the complexity of the decisions that accompany the consideration of implementing a teleoncology in Qatar. The literature review detailed challenges and facilitators for implementing 24-h call service for cancer patients. These were grouped as human, technology, documentary tools, and organizational domains. The core concept that integrates each of these domains is communication.
Conclusions:
If the telephone triage is to be implemented in National Center for Cancer Care and Research (NCCCR), more research is needed about the characteristics of cancer patients in Qatar. A more robust understanding of this population will inform decisions about the utility of developing a teleoncology service at NCCCR.
Introduction
Cancer patients may undergo various combinations of treatment modalities with associated side effects and complications. Telephone cancer services are designed to respond to cancer patients in their homes and to provide them with medical and nursing advice based on their signs and symptoms. 1,2
Telephone triage is “an interactive process between the nurse and client that occurs over the telephone and involves identifying the nature and urgency of the client's healthcare needs and determines the appropriate disposition.” 3 Telephone triage is a subspecialty and the success of telephone triage requires high standards of protocols and guidelines, advanced technological equipment, and qualified staff who have good experience and training. 4 Outcomes regarding the success of telephone triage are currently measured using data such as reduced unnecessary emergency visits, reduced healthcare cost, and number of calls and metrics about facilitated access to care. 3 Broadly, providing health assessment and advice over the telephone has been “recognized as a means of improving access to and quality of healthcare services, particularly for rural or underserved populations.” 5 The term teleoncology has been developed by Maserat to reference remotely provided cancer care. 6 The main goal of this integrative review was to explore the challenges and facilitators for implementing 24-h telephone cancer service. In particular, the review was conducted to support healthcare administrators to consider the feasibility of implementing telephone services for cancer patients in Qatar.
Cancer causes 10% of all deaths in Qatar and the probability of developing cancer increases with age and life expectancy is rising. 7 In 2011, The Qatar National Cancer Strategy was developed with aims and objectives for 2015 to improve the cancer patients' journey care in Qatar.
Methodology
This study is an integrative literature review of primary resources about the challenges and facilitators of implementing 24-h call service for cancer patients. According to Torraco, an integrative literature review is “a form of research that reviews, critiques, and synthesizes representative literature on a topic in an integrated way such that new frameworks and perspectives on the topic are generated.” 8 This literature review follows the framework that was proposed by Whittemore and Knafl who described an integrative review as “a specific review method that summarizes past empirical or theoretical literature to provide a more comprehensive understanding of a particular phenomenon or healthcare problem.” 9 They proposed 5 phases of an integrative review: (1) problem identification, (2) literature search strategy, (3) data evaluation, (4) data analyses, and (5) presentation. 9
Literature Search Strategy
This integrative review included articles that reflect original qualitative, quantitative, and mixed-methods research with primary data that were published in English between 2000 and 2015. The keywords used in the literature search were “telephone triage,” “phone support service*,” telemedicine*, helpline*, hotline*, tele nurse*, 24#hour, Service*, support, “cancer OR oncology OR neoplasm,” impediment*, advantage*, barrier*, obstacle*, challenge*, and facilitator*. Articles were retrieved from Medline, Cumulative Index of Nursing and Allied Health Literature, and Ovid Nursing electronic databases. All reports, secondary resources such as literature reviews, and unpublished articles, such as abstracts and dissertations, were excluded. The preliminary search identified 503 articles. In addition, 21 articles were identified by a manual search from the reference lists. Figure 1 shows the number of retrieved articles from each database. After applying the inclusion and exclusion criteria, 13 of those 37 articles were deemed fit for inclusion in this literature review (Fig. 2).
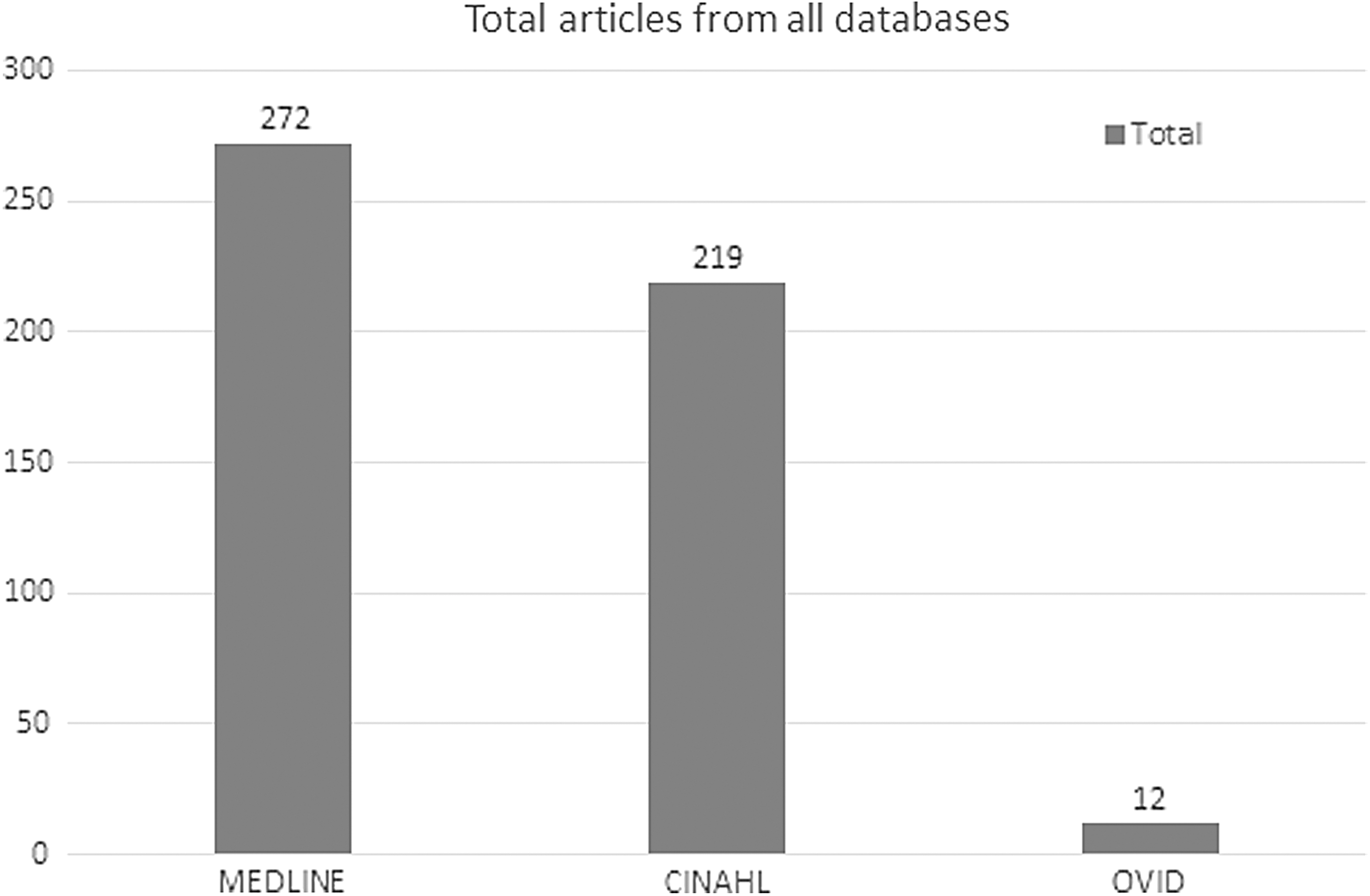
Total articles from all databases.

Flowchart showing the results of the study selection process.
Findings
The five domains—(1) human, (2) technology, (3) organization, (4) documentary tools, and (5) communication—are interrelated. In particular, the communication domain emerged as a core feature across all the challenges and facilitators to teleoncology practices. This integrative review found that all the factors under each domain can be either a challenge or a facilitator depending on how they are dealt with in the planning and start-up phase of a teleoncology service. Finally, in stage 4 of the review process, the domains were developed into a conceptual framework for addressing barriers and facilitators during the implementation of teleoncology.
Human Domain
The most commonly cited issues relevant to implementing telephone triage for cancer care are in the human domain. 2,10 –18 These issues revolve around the people who are implicated in the services, and most often refer to nurses, other team members, patients, and their families. As well, the human domain includes broad community attributes. Each of the groups of people who constitute the human variable can be considered a stakeholder group related to teleoncology.
Nurse Attributes
Nurse attributes are conceptualized in the literature as challenges and facilitators. The attributes can be classified into four elements: knowledge, skills, experience, and level of confidence. When nurses lack knowledge, skills, experience, and/or confidence, it generates a barrier to the success of a telephone health service. 16,17,19
According to Singh and Warnock, 2 it is crucial to educate and train all nurses who will use the telephone system and companion resources. This is the case no matter how much prior nursing experience they have. The specialty education for teleoncology nurses includes telephone training. This training is necessary to develop the nursing skills related to conducting assessments over the phone and using guidelines to give advice. The absence of nonverbal communication cues is a challenging element of a telephone nursing practice, and nurses must be trained in how to elicit assessment data on the phone using verbal probes. 14 As well, nurses must be comfortable with the telephone technologies such as telephone call waiting systems and mobile phone applications, for monitoring patients at a distance. These nurse training factors must be taken into consideration during the planning phase of teleoncology implementation because well-trained nurses increase the success of the telephone triage program.
In the literature, nurses' knowledge has been discussed in light of guidelines, technologies, protocols, and policies, and patient information. Stacey et al. 17 used a mixed-methods design to survey nurses from three different ambulatory oncology services in Canada to determine nurses' perceptions of factors that influenced the nurses' use of symptom protocols when providing remote management for oncology patients. In this study, nurses reported that using the protocol resulted in standardized approaches for providing remote support for the patients. Eighty-three percent of the participating nurses believed that the use of protocols enhanced remote symptom management outcomes. However, 20% of the nurses perceived the protocol to be complex, and 55% of nurses reported that the lack of flexibility embedded in the guidelines created challenges in the care of some patients. In this regard, some nurses reported that their knowledge and experience were not appreciated when they were closely tied to a written script. Very importantly, there were nurses who reported that they worried about asking too many questions. They were concerned that the list of required questions may irritate the patients who were calling for support. They thought that the standard requirement to ask specific questions was sometimes irrelevant to the call, and this impacted nurses' compliance with the telephone scripts.
Despite the expectation that nurses adhere closely to algorithms, their expert knowledge about the types of calls is an important human factor for good telephone triage. Macartney et al. 12 conducted a survey to investigate nurses' recalls and impressions regarding the most common symptoms patients called about. In addition, the survey was designed to identify the facilitating factors and barriers that impact the telephone triage healthcare services.
Team Attributes
In most of the studies included in this literature review, nurses were the core telephone responders; however, the nurses seldom worked in isolation from the multidisciplinary team (MDT) where nurses could consult about and refer callers to doctors and allied health professionals. The literature on barriers and facilitators to telephone triage includes factors related to team attributes that fall under the human domain of the teleoncology model developed from this integrative review. The success of telephone triage depends on good relationships and cooperation among other services, such as diagnostics, pharmacy, homecare, family physician, and emergency room. 12 They reported that physician availability, support, and responsiveness are considered facilitators for telephone triage implementation. In addition, nurses need to be supported by administrators. Training and education of the entire MDT is an important facilitating factor for the providers who have no or little experience on how to use the telephone triage equipment to be comfortable and confident while using this kind of technology. 10 Doorenbos et al. reported that lack of experience for all the MDT members about the telephone triage technology might affect the success of the project. 10
Patient, Family, and Community
Since the telephone triage project is patient centered, it is crucial to consider, during the planning phase, strategies that aim to proactively overcome the challenges highlighted in the literature. Stacey et al. 17 designed a research project to assess the factors that impact nurses who use the symptom protocols while providing remote services for cancer patients. These researchers reported that patient-related barriers may include communication-related challenges, individual preferences, and limitations of comprehending over-the-telephone advice. Accordingly, Stacey et al. suggested that using some prompts may help the nurse ensure the patient's comprehension of the advice, such as “Do you understand?” This may contribute to improving patient outcomes. 17
Doorenbos et al. 10 also identified a very important determinant for the success of telephone triage system, which is a trusting relationship between patient and nurse. According to this study, it can be difficult to establish a trusting relationship between the patient and the telephone responder. Therefore, to augment trust, significant consideration needs to be given to understand and respect the historical, legal, political, and cultural background of the patients and the community that the teleoncology organization serves. Similarly, Stacey et al., 19 in their report about how to enhance patients' understanding about the use of protocols, stressed the need to raise public awareness about the service, how it works, and its contribution to improving the health condition of the target population.
Technological Domain
Technology is a core component of teleoncology and can be classified under two categories of challenges and facilitators. These two categories relate to (a) the actual equipment and technical infrastructure and (b) issues such as access, privacy, security, legal, ethical, cultural, and economic issues that are nontechnical but arise from the technology.
Technical factors related to the broad telecommunication infrastructure, such as radio masts and towers and communication satellites, must be considered. As well, factors such as decisions about networking hardware, data storage capacity, type of telephone equipment, and IT support are critical considerations during planning and implementation. It was asserted that the main attribute for project success is related to ensuring technical readiness. 10 Well-planned and managed telecommunication infrastructures are key to successful service.
Access, security, legal, ethical, cultural, and economic factors are also important features of the technological domain. Hall and Murchie argued that some patients, especially elderly people, are reluctant to engage in using modern technology. 20 Levine et al. 11 conducted a qualitative study to identify perceived barriers and facilitators to using smartphones and telemedicine technology to monitor older adults with chronic noncancer pain. The study found that this population of patients was unable to use the technology and that this was a barrier to the success of the program.
Organizational Domain
There are many barriers and facilitators related to the perceived organizational support. Time constraints related to the timed targets for each call, telephone responders' workload, and the provision of adequate education and training for staff are the most commonly cited organizational barriers in the literature. Organizational support is closely linked to the human factors as it relates to available resources to support practitioners. Macartney et al. 12 conducted research into oncology nurses who were providing remote care to identify the most prevalent and challenging symptom management. This study also explored the factors that affect the remote support system. They found that time constraints and workload are the most common barriers in any initiative for changes in practice. In the context of telephone triage, the time constraint can be defined as the length of time expected to provide the service and the length of time patients spend in “call waiting.” Also, they reported that 29% of the nurse participants identified that the time available for providing the remote support service is too short. Similarly, Stacey et al. 17 found that 78% of nurse participants determined that the time allocated to provide a remote support by using the protocol was inadequate. Their participants claimed that their organizations forced them to minimize the call length, which placed the nurses under a great deal of pressure to achieve the organizations' targets.
Closely linked with available time, workload is another organizational factor that influences the success of the telephone triage service. Twelve percent of the participants reported that workload and inadequate staffing levels are barriers to implementing a telephone triage service for cancer patients. 12 Stacey added that the lack of electronic charts and/or lack of directions on how to use them were reported as a barrier by more than 50% of the nurses who participated in their study. 17
Organizations are implicated in lack of training and education and the lack of clear mandates on how to use guidelines and protocols. These are important organizational factors that influence the success of telephone triage. They must be proactively addressed during the project's planning phase. 12,17,19 According to Stacey, 17 nurses reported that they not only needed special training to assist them to assess patients remotely without physical contact but that specialized training is also required to effectively using remote symptoms management protocols and the technology that underpins these systems.
Accordingly, organizational facilitators include, but are not limited to, providing staff training and education, integrating the electronic health records, key stakeholder involvement from the beginning of the implementation process, dedicated space for the telephone services, and enough call time to provide the service. Moreover, providing easy-to-access guidelines may facilitate the success of the project. These guidelines should comprehensively address symptoms and must be consistent with the educational resources that patients are given during their cancer treatments. 12,17,19
Documentary Tools Domain
According to Stacey et al., 17 documentary tools are a crucial component of safe and effective implementation of telephone triage service. Guidelines, protocols, and policies are important to standardize the telephone care services and are expected to help telephone triage nurses to assess, prioritize, and guide patients with the proper interventions. The quality of the documentary tools developed for telephone triage implementation are key barriers and/or facilitators and revolves around the availability, characteristics of the tools, and training and education related to their use. Easy access to the documentary tools that support telephone triage improves the telephone triage services. 12
The major characteristics for documentary tools that were highlighted by this integrative review relate to the complexity of documents, their adequacy for the management of multiple symptoms, and the currency of the evidence embedded in the algorithms and guidelines. Underlying the focus on documents is the ease of use and the quality of nurses' documentation and record keeping. 2,12,16,17
According to Singh and Warnock, 2 there are many factors that relate to documentation, and there is a debate about the usefulness of documentation that provides opportunities for nurses' narrative notes compared to the simplicity and ease of flowcharts and tick boxes. Similarly, Macartney's 12 nurse informants reported that training and education about how to use the symptom management guidelines are developed as a core skill that is directly linked to the documentary design. According to them, this negatively impacted the quality of documentation and increased the risk of liability for the organization. Stacey et al. also made reference to the legal risks of incomplete documentation. Their integrative review points to the critical importance of the documentary tools developed to support telephone triage and the necessity of evaluating the documentation forms and assessing how well they work for the triage nurses who use them. 17
As with each of the domains that contribute to the conceptual framework developed from this integrative review, in the documentary tools domain, training and education for nurses are core factors. Nurses must be well oriented to the documents and their use. Lack of a clear process that enables nurses to quickly and accurately assess and prioritize callers is considered a barrier to successful implementation. Developing useful documentary tools and systems is critical and must be considered during the early stages of project implementation. 2,19
Communication Domain
Communication is an essential component in healthcare relationships. Mooney et al., 13 who studied telephone-linked care for cancer symptom monitoring, described the various technologies used but indicated that cancer care provided remotely most commonly uses simple telephone or audio contact between the healthcare professional and the patient.
Researchers highlighted language barriers, unclear speech, and hearing difficulties as serious communication challenges that can be barriers to effective remote support. When these barriers are present, the patient's and family's capacity to describe the symptoms, the care provider's capacity to understand caller's descriptions, and the caller's ability to understand the advice given seriously jeopardizes quality outcomes in teleoncology. 12
Mooney et al., an interpersonal communications expert, cited the National Cancer Institute in 2001 to argue that there is a significant opportunity to use technology for improving the provider/patient communication during cancer treatment. 13
A more focused view of telephone communication is evident in the qualitative study by Neergaard et al. that concentrated on specialized palliative care. These authors investigated the health professionals' point of view on modern telecommunication as a mode of healthcare service. Their respondents talked about the different communication skills that created distinctive differences among calls with patients, calls with relatives, and calls with other professionals. 21
Discussion
Broadly, the literature on telehealth reveals that nurse-led telephone triage is an effective way to provide support for patients in their homes. 3 As well, it supports triage for patients who require medical care to direct appropriate responses to serious illness and/or to enhance early intervention to prevent complications and serious illness. Most telephone triage services are linked into emergency health services, and the linked dispatch services can initiate emergency medical services to the patient's home. 2 In cancer care, telephone triage holds promises for oncology nurses to provide high-quality health advice to cancer patients. According to Stacey et al., the service has been found to decrease the number of unnecessary emergency room visits and contribute to the early recognition of oncologic emergencies that need immediate intervention. Flannery and Stein found that it is a resource for emotional support for the patients and their families, and that it supports continuity of care. 22
Conceptual Framework
The conceptual framework that was developed from and organized the findings of this integrative review is presented in Figure 3. The tools and skills listed in each of the domains must align to produce accurate information, clear communication, and a strong human element that is the essential feature of a successful teleoncology service. Also, the conceptual framework highlights language in the communication domain in Qatar. The inclusion of language as part of the core communication component of the conceptual framework is particularly important in the distinctive Qatar healthcare environment, through which the majority of the population in Qatar does not share the same first language. While healthcare is conducted in English, for the majority of healthcare providers, English is not their first language. However, there are many foreign residents in Qatar who speak minimal English and no Arabic. These language demographics complicate communication among healthcare workers and communication between healthcare workers and patients.
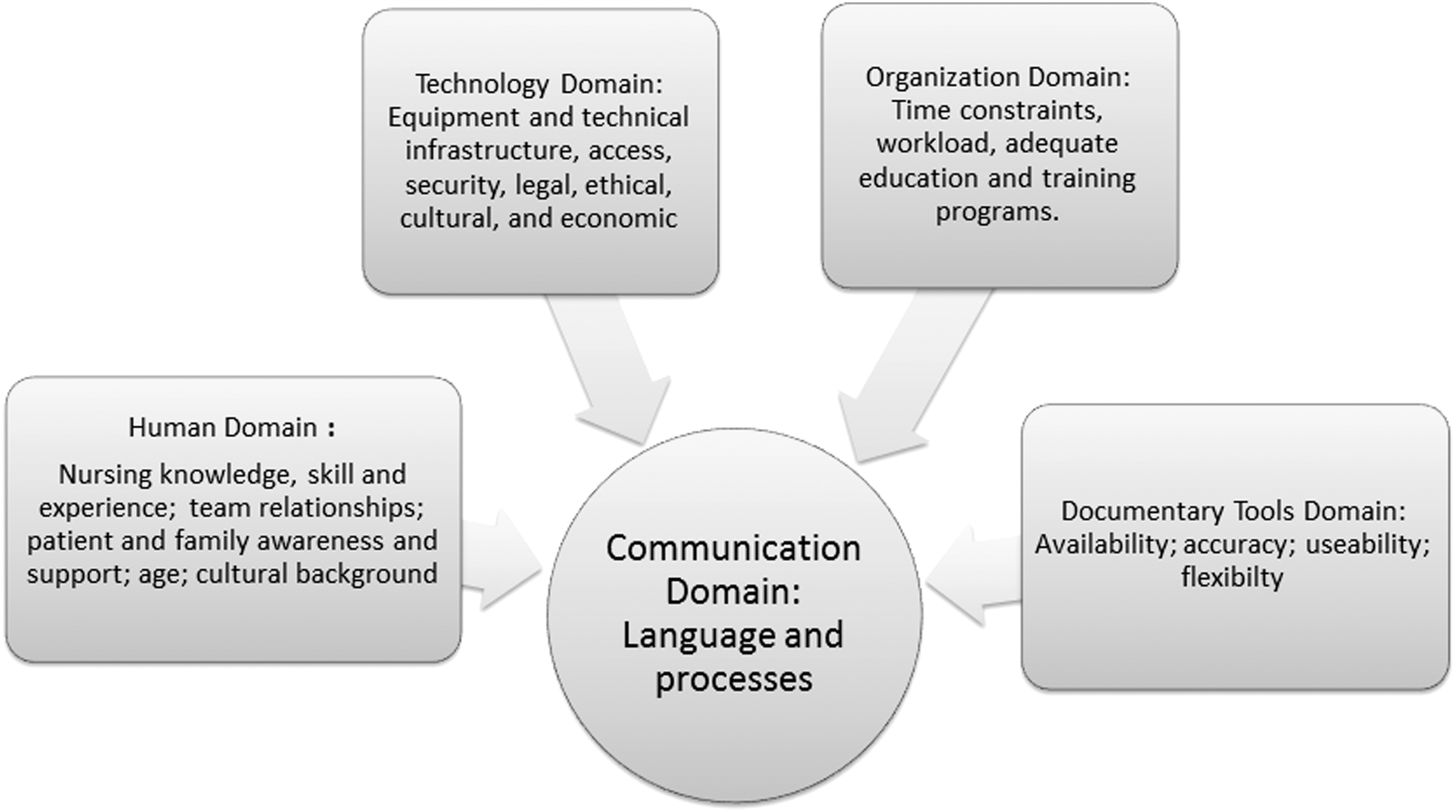
Telephone triage conceptual framework.
The findings of the integrative review support the conclusion that communication is the key to effective teleoncology services. Communication by telephone is different from face-to-face assessment. The absences of visual cues that are considered essential in the conventional face to face triage are not available for teleoncology nurses. The literature is conclusive that these important telephone skills require training. In addition, even with access to good documentary tools, the literature about teleoncology nursing suggests that it is vital for nurses to have extensive clinical experience with cancer patients to effectively respond to patients' questions. 12,17,19
Limitations
This literature review, as with any study, has limitations. Some of these are related to the search and the articles that were retrieved and included. The large number of articles that were retrieved through the manual bibliographic search demands that the search terms be addressed as a possible limitation. The integrative review exposed language terms such as “remote service,” “tele-oncology,” and “tele-practice.” These seem to be new terms that have not yet been widely adopted. Nonetheless, they represent a useful terminology that must be considered search terms for future investigations.
The core term adopted in the findings of this integrative review is the term tele-oncology. Teleoncology first appeared in an article by Maserat 6 who described teleoncology as the delivery of “…clinical oncology services at a distance … encompass the use of electronic devices to aid clinical diagnosis, treatment and follow-up based on the transfer of video, images of clinicians and patients and data including pathology and radiology images, graphics and text” (p. 811). The term “tele-practice” was credited to the College of Nurses of Ontario. Nursing telepractice is described as “the delivery, management and coordination of care and services provided via information and telecommunication technologies.” 16
The final limitation for the search could be the close adherence to the Whittemore and Knafl 9 methodology, which suggests that an integrative review should focus on primary source studies and exclude secondary sources. For the purpose of this review, excluding secondary sources meant that no other literature reviews could be included, and this exclusion may have unnecessarily limited the findings. Nonetheless, we are confident that the focus on barriers and facilitators that we identified as the problem, the systematic literature search strategy, the use of the matrix for data evaluation, data analyses, presentation of findings, and discussion are a reliable resource, not only for planners and decision makers in Qatar but also for healthcare executives and providers in other regions who are considering implementing teleoncology services.
Recommendations and Dissemination
One of the strongest recommendations from the examination of this topic through an integrative review is that more research is needed about the characteristics of cancer patients in Qatar. A more robust understanding of this population will inform decisions about the utility of developing a teleoncology service at National Center for Cancer Care and Research. It may also be the case that a nursing teleservice in Qatar needs to include broad health concerns and not be focused only on cancer. Additional research is needed to support these sorts of decisions.
Conclusion
The literature of this review highlights the complexity of the decisions that accompany the consideration of implementing the teleoncology in Qatar. The literature review detailed challenges and facilitators for implementing 24-h call service for cancer patients. These were grouped as human, technology, organizational, documentary tools, and communication domains. The core concept that integrates each of these domains is communication. The objective of this review was to summarize and synthesize past literature to “present the state of the science.” 9 Closely following the strategies suggested by Whittemore and Knafl sustained the rigor of this literature review. 9 The data comparison process supported the development of a useful diagram that denotes the conclusions and represents the depth and breadth of what is currently known about the topic. The work contributes a new understanding that is useful to practice and policy. The findings of this project will have direct applicability to cancer care in Qatar.
Footnotes
Disclosure Statement
No competing financial interests exist.