
Abstract
Introduction
With rapid advancement in information and communication technologies, several applications such as the internet of things and smart wearable devices have been proposed for the management of telehealthcare services, particularly for aging populations. The burgeoning elderly demographic in Taiwan represents a key challenge with regard to planning for the efficient delivery of health care for the elderly population given the increased demands for long-term health care and medical services entailed. To address the challenge, it is necessary to develop long-term telehealthcare plans.
The integration of telehealthcare technologies into geriatric care offers many advantages for doctors and caregivers. One such advantage is remote monitoring. The technology can facilitate the management of health care in patients who do not require daily medical assistance by communicating medical data to health care providers from wearable smart devices such as wristbands or watches. 1,2 Telehealthcare systems can also play a vital role in family and social care, reducing social and medical costs in a social context in which the numbers of middle-aged people caring for elderly patients is increasing. 3,4 It is reasonable to assert that the health care service industry should integrate emerging smart technology products and services into their practice.
Many studies on telehealthcare have focused on patient satisfaction and feasibility or development of long-distance care services. 3,4 However, there is a lack of evidence concerning users' practical experience based on the journey mapping approach. The purpose of this article was to document telehealthcare technology users' experience with smart devices. The article assessed users' acceptance of telehealthcare in a longitudinal manner to clarify the underlying factors for consideration for widespread implementation and adoption of telehealthcare among Taiwan's elderly population. The research took an integrated mixed-methods approach, exploring the users' journey by mapping experience and evaluating acceptance to address a number of pertinent research questions. First, what are elders' experiences and technology acceptance of telehealthcare devices used at home? 5 –7 Second, what are users' suggestions for telehealthcare device design or improvement? Third, does usability affect users' acceptance of the technology? Finally, what suggestions could this study provide for future device and service design?
Using smart mobile devices or telehealthcare platforms to address the health problems of an aging population may seem straightforward. 8 However, the implementation of the technology is complicated by user experience. Users need to wear the sensor every day to measure their physiological information, and thus acceptance of the long-term wearing, the appearance, the interface, the operation, the duration, the substantive value, the product stability and the value-added services associated with the devices is critical and must be understood through user opinion and authentic experience.
The health care industry must extend care services to holistic health care, take advantage of information technology, and apply it innovatively to health care services to cope with the social impacts of chronic diseases that beset the aging population. To clarify whether contemporary telehealthcare technologies meet the needs of this demographic, this study revealed users' journey maps and used a questionnaire to investigate users' use behavior, their acceptance of the technology, and its usability.
The Aging Society and Telehealthcare
In 2016, the Taiwan National Development Council reported that by 2018 the ≥65 years demographic will have increased 14%. By 2025, the elderly population is expected to exceed 20% of the total, making Taiwan a predominantly elderly society. 9 The same phenomenon is occurring simultaneously in Japan, China, and Germany with major implications for each society in terms of health care. 10,11 Demands on caregivers for medical services and long-term care will increase. In addition, there will be an increased demand for assistance to caregivers to help them care for the elderly people. In response, the consumer health care market is expected to shift its focus from traditional elderly health care and related services to telehealthcare services.
Telehealthcare offers many key advantages. 12 –14 For instance, elderly people who do not need daily medical assistance can communicate with health care providers by wearing wireless devices such as wristbands or watches. 1 Relevant studies posit that as the proportion of middle-aged people who must care for the elderly increases, a well-established health care system helps to integrate technology and information, offsets the pressure on caregivers, and reduces both social and medical costs. 15
Chen and Shieh proposed the development of a long-distance care service strategy selection model in which (1) each specialized institution as a unit provides telehealthcare services, (2) medical institutes coordinate and establish telehealthcare centers independently, (3) medical institutes establish a strategic alliance with noncompetitive parties, and (4) medical institutes establish a strategic alliance with diverse industries. 3
Telehealthcare has been defined as, “The use of communications technology to provide health and social care directly to the user (patient). This excludes the exchange of information solely between professionals, generally for diagnosis or referral.” 16 A number of low-cost sensors have been developed that use telemetry to provide electronic measures of certain activities, such as inputs to assessment measurements. These sensors can measure a wide range of functional performances, providing a means of continuously and objectively assessing a patient's condition after hospitalization. 17,18 Telecare technologies allow hospitals to continuously monitor biomedical indicators while also providing patients with online services such as clinical appointment scheduling, medical consulting, remote alerts, and so on. Telecare has the potential to transform the health care industry by reducing costs, increasing quality, and enhancing patient satisfaction. 19 It has also been promoted as an effective tool to enable clinicians to work smarter, although some health stakeholders believe the technology will compel users to work harder by creating extra work. 20
User Experience and Journey Mapping
Alben defined “experience” as all the aspects of how people use a product: the way it feels in their hands, how well they understand how it works, how they feel about it while they are using it, how well it serves their purposes, and how well it fits into the entire context in which they are using it. 21 The term user “experience” has even more elements, taking into account the wider relationship between the product and the user to investigate the individual's personal experience. 22 –24 It can incorporate the complete set of effects elicited by the interaction between a user and a product, including the degree that all senses are gratified (aesthetic experience), the meanings that are attached to the product (experience of meaning), and the feelings and emotions that are elicited (emotional experience). 25 Draft International Standard defines user experience as all aspects of experience when interacting with a product, service, environment, or facility. In their terms, user experience is dynamic, context dependent, and subjective. 26
Some authors have proposed defining user experience as something individual, rather than social, that emerges from interaction with a product, system, service, or object. 27 A study in selected hospitals in Ghana illustrates this conception. Semistructured interviews incorporating the critical incident technique were conducted with 8 doctors and 24 outpatients, exploring patients' experiences of health care. An abductive and thematic analytical approach was used to identify 76 useable critical incidents that had significant influence on both the outcome of the service and patients' experiences. 28 From this perspective, customer experience can be regarded as a holistic interactive process, facilitated through cognitive and emotional clues, moderated by customer and contextual characteristics, resulting in unique and pleasurable (or not) memories. 29
In summary, user experience has many facets. It is the cumulative result of the aesthetic, experiential, and emotional senses in the interaction between the user and the device. Specifically, it includes tactile feel, operational knowledge, user-friendliness, and effectiveness. Moreover, user experience is impacted by visual feeling, customer service, and brand impression.
Journey maps have been applied in many fields to assess user experience, design, usability, and marketing. Journey maps describe “significant changes in a user's needs, degrees of satisfaction with the product, or other use metrics across phases of the user's experience.” They provide graphic visualizations and valuable data such as point of view, touchpoint, challenges, or frustration of a user's experience with a product or service. 30
Previous studies have used user journeys to develop diverse service dimensions. Risdon asserts that journey models should illuminate the most important dimensions, perhaps a transition or a switch between channels. 31 They should not simply illustrate a journey step-by-step, but should reveal something about it based on how the data are modeled—for example, how many people use one channel over the other, or what part of the experience is blatantly broken, or what part of the experience has not been considered. The user's journey map must describe the point of contact between each user and the product and/or service provider.
Bate and Robert brought the user experience to health care improvement. 32 In 2015, Chinese designers worked on health care service design to determine the advantages and disadvantages of the methods they used. They found glaring unbalanced consideration between safety and experience in their design process. Learning from this, balanced combinations of experience and safety maps can help designers cope with health care service design issues. 29
In conclusion, a user journey map allows designers and researchers to re-create a variety of methods for diverse projects. Telehealthcare services are complex service networks consisting of elderly patients as end users sharing information through smart devices with medical professionals and caregivers. To test the efficacy of such a service, journey mapping is used to record user experience throughout the process of using a telehealthcare device.
Unified Theory of Acceptance and Use of Technology
The Theory of Rational Action postulates that a person's intentions about performing a behavior are influenced by social pressures or “subjective norms” that arise from his/her perceptions of what others will think while performing the behavior in question. In this theoretical model, both personal attitudes and social or “normative” factors exert a direct influence on behavioral intentions, which are the strongest predictor of actual behavior. 33 As in the original theory, a dominant factor in the Theory of Planned Behavior is the individual's intention to perform a given behavior. Intentions are assumed to capture the motivational factors that influence a behavior. They are also indicative of how hard people are willing to try, and the level of effort he/she plans to exert, to perform the behavior. In general, the stronger the intention to engage in a behavior, the more likely it will be performed. It should be clear, however, that a behavioral intention can find expression in behavior only if the behavior in question is under volitional control. 34
In 1986, Davis suggested the Technology Acceptance Model (TAM) to bridge the gap between previous behavior research and behavior in a technology acceptance framework. 35 He examined the mediating role of perceived ease of use and perceived usefulness in their relation between a system's characteristics (external variables) and the probability of system use (an indicator of system success). More recently, Davis 35 proposed a newer version of his model: TAM2. It included subjective norms and was conducted with a longitudinal research design. Overall, the two models explain ∼40% of a system's use. Analysis of empirical research using TAM shows that results are neither consistent or clear, suggesting that significant factors are missing from the models. 35,36
In this study, we refer to the unified theory of acceptance and use of technology (UTAUT) to analyze the acceptance of technical services and to collect the experience of using novel telehealthcare devices from users. UTAUT theorizes that four constructs play a significant role as direct determinants of user acceptance and use behavior: performance expectancy, effort expectancy, social influence, and facilitating conditions. In addition, there are four key moderators: gender, age, voluntariness of use, and experience (Fig. 1). 37
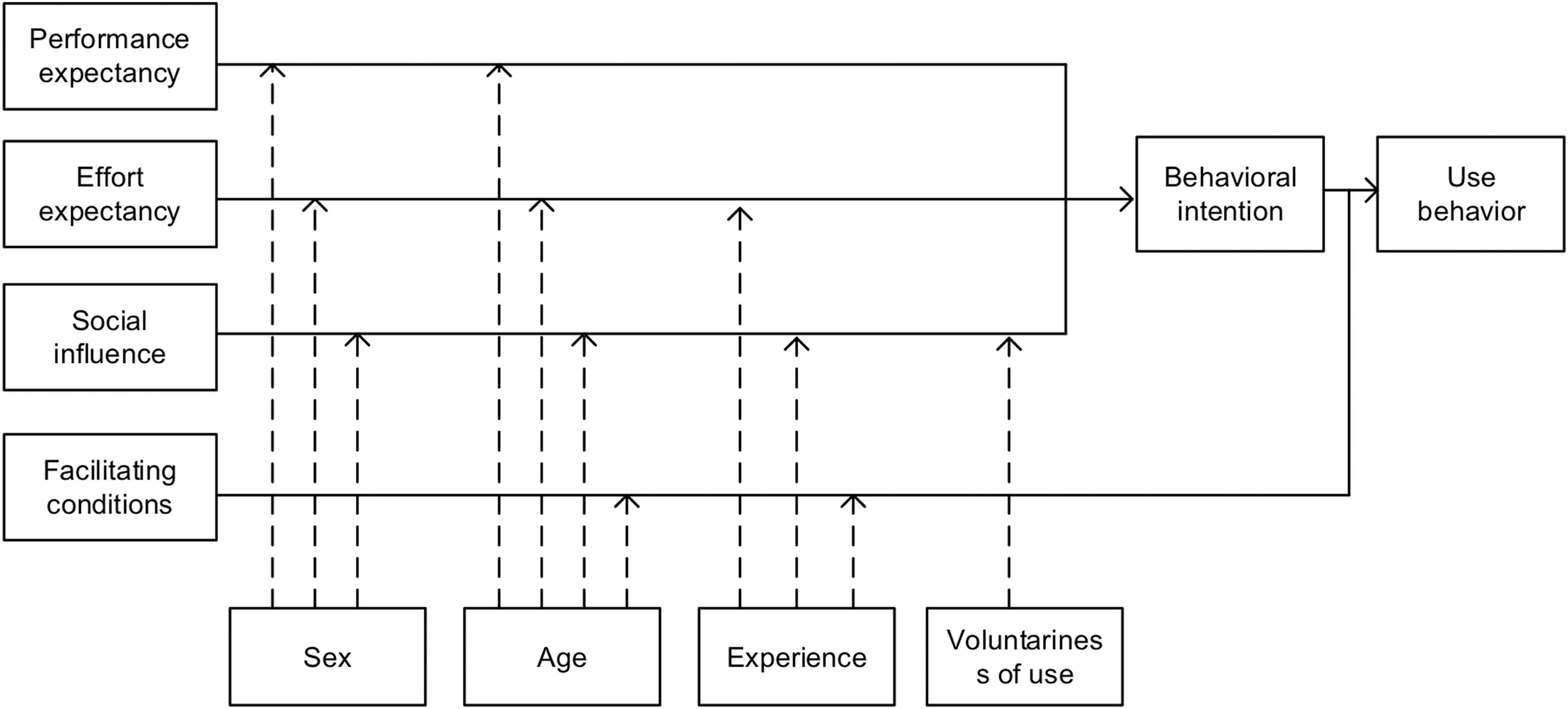
Unified theory of acceptance and use of technology.
Performance expectancy is the degree that an individual believes that using the system will help him/her attain gains in job performance. It includes perceived usefulness, extrinsic motivation, job fit, relative advantage, and outcome expectation.
Effort expectancy is the degree of ease associated with the use of the system. Three constructs from the existing models capture the concept of effort expectancy: perceived ease of use, complexity, and ease of use.
Social influence is the degree than an individual perceives how importantly others believe he/she should use the new system. Social influence as a direct determinant of behavioral intention is represented as a subjective norm in the previous model.
Facilitating conditions is the degree that an individual believes that an organizational and technical infrastructure exists to support use of the system. This definition captures concepts embodied by three different constructs: perceived behavioral control, facilitating conditions, and compatibility. 37
Usability Evaluation Model
Usability is defined as “the extent to which a product can be used by specified users to achieve specified goals with effectiveness, efficiency and satisfaction in a specified context of use.” 38 It is defined by five quality components: (1) Learnability: how easy is it for a user to complete a basic task at first use? (2) Efficiency: how quickly can a user become familiar with the system perform tasks? (3) Memorability: how easy is it for a returned user to reestablish proficiency? (4) Errors: how many errors does a user make using the system, how severe are the mistakes, and how difficult or easy is it to recover from the mistakes? and (5) Satisfaction: how satisfied are the users with using the product? 38
Nielsen's 38 components defined usability in a broad sense, covering not only the ease of use and the effectiveness of the product, but also the subjective users' preference satisfaction. In addition, Brooke 39 developed a questionnaire, the System Usability Scale, which takes quick measurements of how people perceive the usability of computer systems. This proved to be an extremely simple and reliable tool for usability evaluations. 39
Research Design and Methods
This study integrated a convergent parallel mixed-methods study design. Qualitative and quantitative data were collected in parallel, analyzed separately, then merged based on Creswell and Plano Clark's suggestion. 40 In addition, a questionnaire was used to test the theory of TAM and examine users' acceptance and adoption behavior. Furthermore, observations and interviews were conducted to assess users' firsthand experiences. The rationale for collecting both quantitative and qualitative data was to yield multiple perspectives so as to derive a more complete understanding of the users, which could provide valuable insight to not only the telehealthcare service industry but also to smart device developers and marketers. 41 The mixed-methods approach facilitates the comparison of perspectives from participants and incorporates the main findings.
Users' Background
There were 51 participants: 33 women (64.71%) and 18 men (35.29%) with a mean age of 52.1 years. Twenty-nine participants held high school or technical college degrees (56.86%) and 22 participants held at least undergraduate university degrees (43.14%). Of caregivers, 22 were spouses (43.14%), 13 were offspring (25.49%), 10 were relatives (19.60%), and 6 were helpers (11.77%). In terms of medical history, five participants had hypertension (9.80%) and two participants had hypertension and diabetes (3.92%).
Data Sampling
Purposive sampling was used. Participants were observed and documented before and during use of the telehealthcare device. In addition, participants were interviewed and completed questionnaires after the use of telehealthcare devices. Each in-depth face-to-face interview lasted 30–45 min and was recorded after obtaining participant consent. This process provided deeper understandings of participants' firsthand experiences that could inform future design and implementation of smart devices. To analyze the vast amount of data, both qualitative and quantitative, content analysis and variance analysis of all variables were adopted to gain credibility, reliability, and validity. We took an explorative approach to transcripts, using only a few predefined codes, to allow the emergence of relevant themes from the qualitative data and to avoid blinkering the analysis with a theoretical bias.
Research Equipment
The remote monitoring for the telehealthcare scenario of smart device application and service design is illustrated in Figure 2. Observing the emotions and experiences after users' interaction with devices can help designers enhance logical design and thinking and design skills. In addition, it can help avoid the repetition of problems. The journey mapping documented every difficulty the participants encountered in operation. The experimental equipment used was the Guider Technology gCare-700H health care watch. This 2G/3G device is equipped with remote positioning, step calculation, and a phone. It supports both iOS and Android mobile devices and uses Bluetooth for blood pressure machine data transmission.
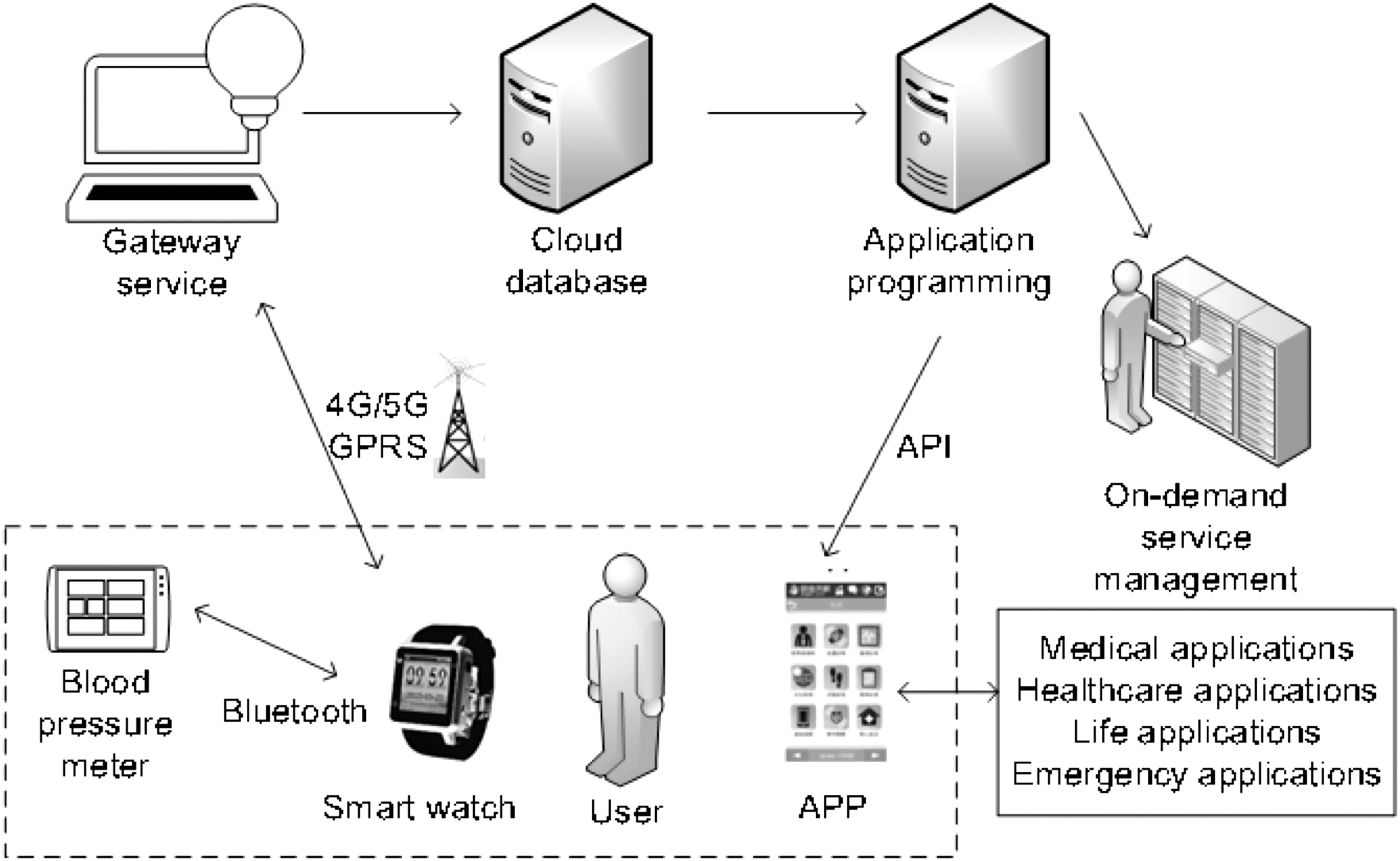
Remote monitoring for telehealthcare scenario of smart device application and service design.
Questionnaire Research Model and Hypotheses
Relatives commonly bear the responsibility of taking care of aged family members. However, the decreasing birth rate means that older adults need to care for themselves. This study utilized the UTAUT model, which posits that performance expectancy, effort expectancy, social influence, and facilitating conditions significantly influence intention to use. 37 In addition, Nielsen proposed that error, learnability, efficiency, memorability, and the usability evaluation would significantly affect users' satisfaction. 38 The proposed model and the research hypotheses are given in Figure 3. The proposed model includes nine determinates of use behavior and several key moderators (i.e., users' age, sex, education, income, medical history, income, and relatives' income).
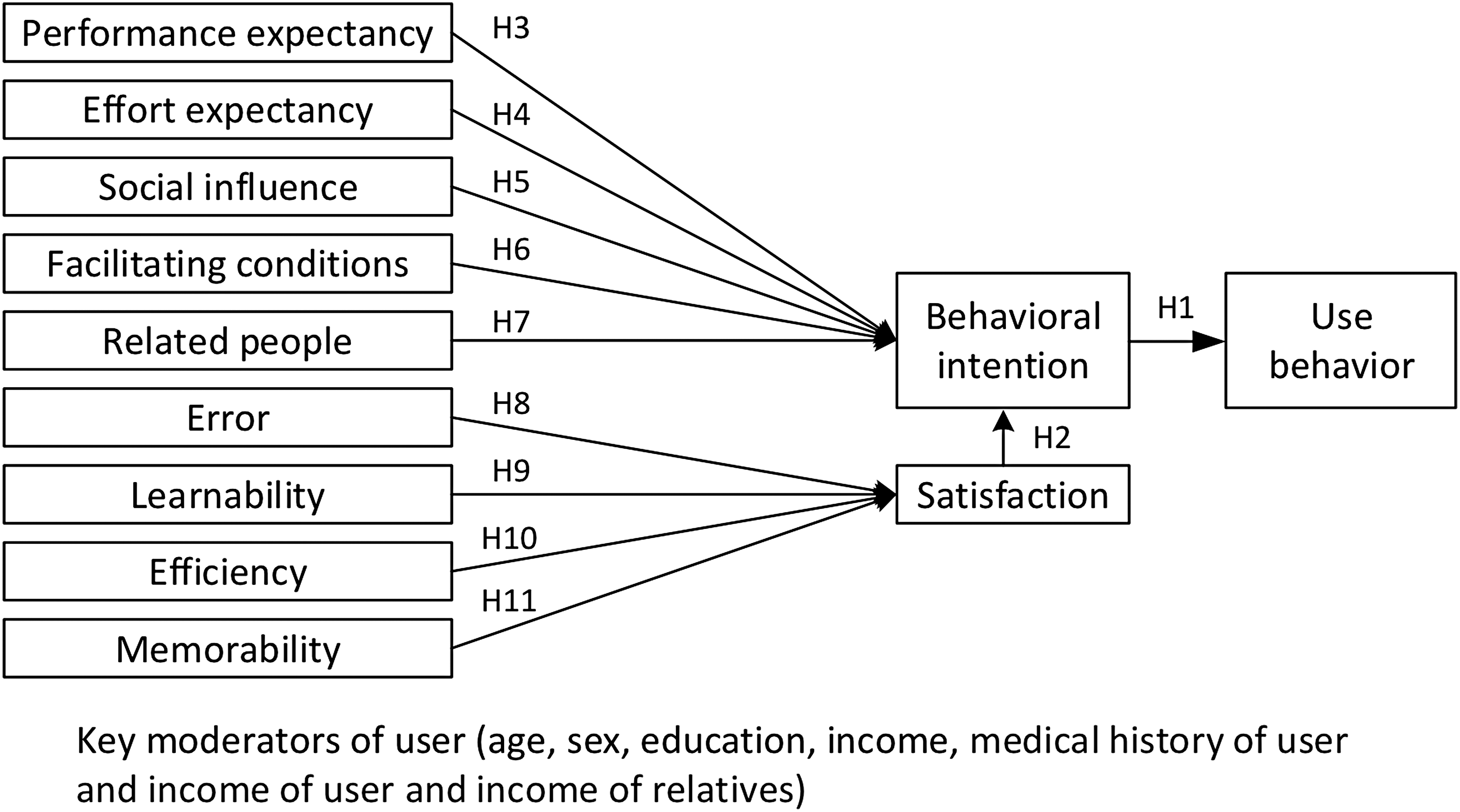
Research model.
H1: Behavioral intention will have a positive influence on use behavior
H2: Satisfaction will have a positive influence on user's behavioral intention
H3: Performance expectancy will have a positive influence on user's behavioral intention
H4: Effort expectancy will have a positive influence on user's behavioral intention
H5: Social influence will have a positive influence on user's behavioral intention
H6: Facilitating conditions will have a positive influence on user's behavioral intention
H7: Relatives will have a positive influence on user's behavioral intention
H8: Error will have a positive influence on satisfaction
H9: Learnability will have a positive influence on satisfaction
H10: Efficiency will have a positive influence on satisfaction
H11: Memorability will have a positive influence on satisfaction
Hypotheses were verified by a questionnaire survey and measured using a five-point Likert design and analyzed with IBM SPSS statistical software.
Results
User Journey Mapping
The telehealthcare journey mapping is illustrated in Figure 4. It documents participants' experience before, during, and after using the smart device.
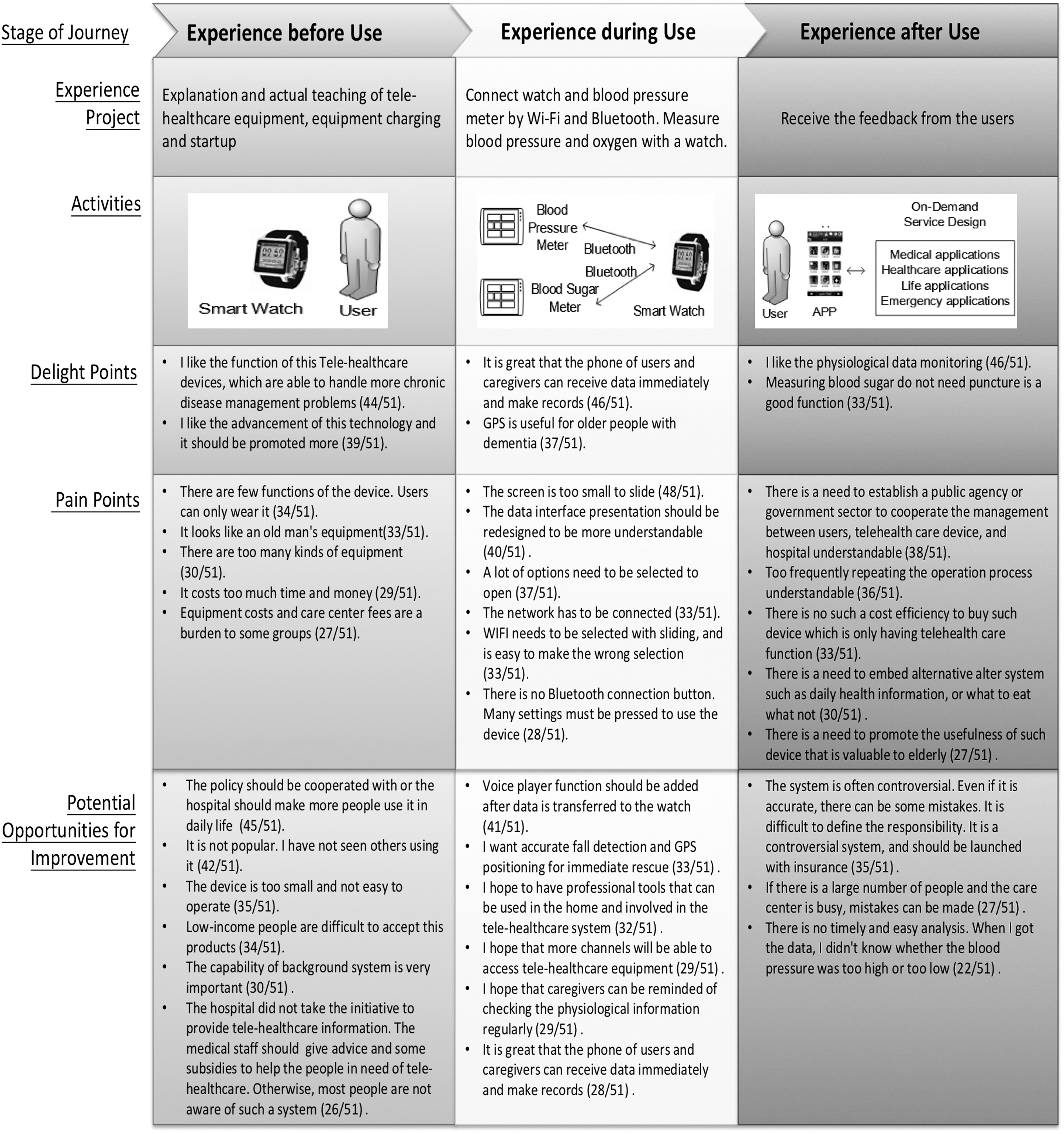
Telehealthcare journey mapping.
Experience before use
Researchers described the attributes and operation of the telehealthcare equipment and helped users set up the devices (Fig. 4). Most (88%) participants complained the device was too small to operate and suggested including touch and sound controls. They also recommended that the device should be replaced by an application on a smart phone that integrates wireless network connections, sound control, and USB function. Considering the above suggestions, the telehealthcare industry should take advantage of the popularity of smartphones and enhance their telehealthcare capabilities in the future.
Specifically, participants noted the following positive aspects: “I like the function of this telehealthcare device—that it can handle chronic disease management problems” (86%, 44/51), and “I like the advancement of this technology. It should be promoted more” (76%, 39/51). In contrast, participants noted the following negative aspects: “The device has too few functions. Users can only wear it” (66%, 34/51); “It looks like old man's equipment” (64%, 33/51); “There are too many kinds of equipment” (58%, 30/51); “It costs too much time and money (56%, 29/51)”; and, “The equipment costs and care center fees are a burden to some groups” (52%, 27/51).
Participants also noted other possibilities for improvement: “The policy should be followed. Perhaps the hospitals should make more people use it in daily life” (88%, 45/51); “It is not popular. I have not seen others using it” (82%, 42/51); “The device is too small and not easy to operate” (68%, 35/51); “People with a low income find it difficult to accept this product” (66%, 34/51); “The capability of the background system is essential” (58%, 30/51); and, “The hospital did not take the initiative to provide telehealthcare information. The medical staff should give advice and subsidies to help people in need of telehealthcare. Otherwise, most people are not aware of such a system” (50%, 26/51).
Experience during use
Users connected the smart watch and blood pressure meter through Wi-Fi and Bluetooth. Measurements of both pressure and oxygen were sent to the smart watch. The participants reported that they opened Wi-Fi frequently and suggested that the simplification of the design of the graphical display, the sound control, and the always-on function would improve the device. The operation of the Bluetooth connection for periodic blood pressure measurements and transmission was too complicated and troublesome. Participants suggested that the function of a one-click Bluetooth connection should be added to the blood pressure machine. To minimize the processing time, telehealthcare systems must be user-oriented in terms of device design, implementation of management software, and user interfaces.
Telehealthcare measurement accuracy is a critical issue. Inaccurate measurements or faulty systems risk safety problems for patients, which may result in litigation, jeopardizing health care centers. Specifically, participants noted the following positive aspects: “It is great that the phone of users and caregivers can receive data immediately and also make records” (90%, 46/51); “GPS is useful for older people with dementia” (72%, 37/51). In contrast, participants noted the following negative aspects: “The screen is too small to slide” (94%, 48/51); “The data interface presentation should be redesigned to be more understandable” (78%, 40/51); “A lot of options need to be selected to open” (72%, 37/51); “The network must be connected” (64%, 33/51); “Wi-Fi needs to be selected with sliding. It is easy to make the wrong selection” (64%, 33/51); and “There is no Bluetooth connection button. Many settings must be pressed to use the device” (54%, 28/51).
Participants also noted room for improvement: “Voice player functions should be added after data is transferred to the watch” (80%, 41/51); “I want accurate fall detection and GPS positioning for immediate rescue” (64%, 33/51); “I hope to have professional tools involved in the tele healthcare system that can be used in the home” (62%, 32/51); “I would like more channels to be able to access telehealthcare equipment” (56%, 29/51); “I wish that caregivers could be reminded to check the physiological information regularly” (56%, 29/51); and although participants reported that “it is great that the phone of users and caregivers can receive data immediately and also make records” (90%, 46/51), they expressed hope that these features “continue to improve” (54%, 28/51).
Experience after use
Participants thought that the telehealthcare equipment could not be used by all chronic patients and the cared-for because of system limitations. For example, bone density determination and kidney function tests could not be performed with the current equipment. In the future, more tests should be supported by the telehealthcare system. The establishment of a medical records database is also a key consideration. In addition, it is essential that telehealthcare systems perform successfully during natural disasters and other emergencies. Developmental goals should then include the ability to cope in emergencies and other critical contingencies. Equipping all devices with GPS and alternate transmission paths may be essential during natural disasters.
Specifically, participants noted the following positive aspects: “I like the physiological data monitoring” (90%, 46/51), and “The ability to measure blood sugar without puncturing the skin is a good function” (64%, 33/51). In contrast, participants noted the following negative aspects: “There is a need to establish a public agency or government sector to co-ordinate management between users, the telehealthcare device and the hospitals” (74%, 38/51); “The operation process has to be repeated too frequently” (70%, 36/51); “There is no cost efficiency in buying devices that only have telehealthcare functions” (64%, 33/51); “There is a need to embed alternative systems such as daily health information or what and what not to eat” (58%, 30/51); and “There is a need to promote the usefulness of these devices as valuable to the elderly” (53%, 27/51).
Furthermore, participants provided feedback, making suggestions for future improvement. For example, 68% of participants thought the adoption and implementation of telehealthcare systems was potentially controversial: “Even if it is accurate, there can be mistakes. It is difficult to assign responsibility. As the system is controversial, it should be launched with appropriate insurance.” In addition, 60% of participants stated the following: “If there are many people and the care center is busy, mistakes can be made.” Finally, 43% of participants reported that there was no timely and easy analysis: “When I got the data, I did not know whether the blood pressure was too high or too low.”
Users' technology acceptance
According to the questionnaire results, users thought that a reasonable cost for telehealthcare was ∼1000 Taiwan New Dollars (TWD) per month. Men were more likely than women to accept the telehealthcare equipment. Men were also more satisfied with the effectiveness of telehealthcare equipment, had more confidence in it, and were thus more willing to endorse the use of telehealthcare for quick assessments of their physical condition in place of going to the hospital. In terms of income, participants with a monthly income <25,000 TWD showed little interest in telehealthcare equipment, whereas higher income groups tended to have more positive attitudes. For example, participants with an income between 25,000 and 35,000 TWD felt no pressure with regard to telehealthcare equipment costs and believed the systems may be effective. Also taking into account that (1) effort expectancy and relatives significantly influenced users' behavior intentions; (2) error and memorability significantly affected satisfaction; and (3) intention and satisfaction affected users' behavior, the government should grant reasonable subsidies and incentives to low-income households as social welfare and assistance for the use of telehealthcare equipment.
Questionnaire Data Analysis
Credibility can measure the reliability of data. If the overall credibility of the scale of variables is >0.70, it means the questionnaire has adequate stability and internal consistency. The analysis result of the credibility of this study reached 0.921.
Variance Analyses
Sex and users' technology acceptance
There were no significant gender differences in most dimensions. Men did have a significantly higher evaluation of performance expectations (p = 0.017) and satisfaction (p = 0.04) than did women, including item 3 of performance expectations—“using telehealthcare equipment can more quickly understand your health than going to the hospital” (perceived usefulness, p = 0.003)” and item 5 “the effectiveness of using telehealthcare equipment is satisfactory” (outcome expectation, p = 0.004). More men than women agree that telehealthcare equipment can allow users to more quickly understand their physical condition in place of going to the hospital. In addition, men reported more satisfaction with telehealthcare equipment than women.
There were no significant sex differences in terms of users' satisfaction. However, “I am very confident in this system” (p = 0.056) and “I would recommend others to use telehealthcare equipment” (p = 0.053) approached significance, indicating that men have more confidence in the use of the equipment and higher tendency to endorse the equipment than do women.
Relatives' medical history and users' technology acceptance
Results revealed that relatives' medical history had no considerable influence on study variables.
Relatives and users' technology acceptance
Relatives were significantly associated with performance expectancy (p = 0.046). Subsequent analysis of the differences in performance expectancy shows that when the caregivers are offspring, the performance expectancy is significantly greater than that associated with other relatives or spouses, meaning that when offspring or young people take care of potential telehealthcare users, users are more able to recognize the functions and expectations of the telehealthcare equipment. Furthermore, when technology products are recommended by offspring, and their use assisted by offspring or young people, users are more willing to accept them.
Interviewers' income and users' technology acceptance
The income of interviewees was significantly associated with social influence (p = 0.041). Subsequent analysis of the differences in social influence shows that people with high incomes think that the public responds well to telehealthcare devices. However, interviewers whose income was <25,000 TWD only gained an average of 2.58 points in social influence, meaning this group of people do not think the public responds well to telehealthcare devices. The government should therefore grant reasonable subsidies and incentives to low-income households as part of social welfare and social relief.
Potential caregivers' income and users' technology acceptance
The income of potential caregivers was significantly associated with performance expectancy (p = 0.044). Participants with incomes ranged between 25,000 and 35,000 TWD gained significantly higher average points than participants with incomes <25,000 TWD or >45,000 TWD, meaning that participants with a moderate income were more satisfied with the effect and benefits of telehealthcare equipment. In explanation, it seems that for participants with incomes between 25,000 and 35,000 TWD the cost of telehealthcare equipment is not a burden and that they believe the equipment is effective. For participants with incomes <25,000 TWD, the heavy cost is associated with no expectation for the equipment, whereas those with incomes >45,000 TWD might use more original equipment or other medical care options bearing higher costs, such as telemedicine and family doctors.
Correlation Analysis of Variables
A table detailing the correlation analysis is included as Appendix Table A1.
Regression Analysis of Variables
We tested the following variables in regression analyses: performance expectancy, effort expectancy, social influence, facilitating conditions, behavior intention, behavior, error, learnability, memorability, efficiency, satisfaction, and relatives' influence.
To ensure the effectiveness of the regression model, we further tested the variance inflation factor (VIF) of dimensions to determine whether there were collinearity problems. Wu said: “VIF is the reciprocal of tolerance. The greater the VIF value, the smaller the tolerance of independent variables and the more collinearity problems there are. When variation expansion factor value is over 10, there may be problems of collinearity among variables.” 42
Table 1 provides the results of the regression analysis for behavior intention on behavior, which was significant and thus supported H1. Table 2 gives the results of the regression analysis for satisfaction on behavior, which were positively correlated and thus supported H2. The results of the regression analysis for performance expectancy, effort expectation, social influence, and facilitating conditions on behavior intention are given in Table 3. As given in Table 4, effort expectancy and relatives' influence have no noteworthy influence on behavior intention. Effort expectancy and relatives' influence were significantly positively correlated with behavior intention. The regression analysis of table of error, learnability, efficiency, memorability, and satisfaction of usability analysis is given in Table 5. Finally, Table 6 shows no significant multicollinearity problem among dimensions. Error and memorability were significantly positively correlated with behavior intention and thus positively associated with users' satisfaction.
Regression Analysis of Behavior Intention on Behavior
ANOVA, analysis of variance; MS, mean square; SS, sum of square.
Regression Analysis of Satisfaction on Behavior Intention
Regression Analysis of Performance Expectancy, Effort Expectation, Social Influence, and Facilitating Conditions on Behavior Intention
The Influence of Performance Expectancy, Effort Expectation, Social Influence, Facilitating Conditions, and Relatives' Influence on Behavior Intention
p<0.01
SE, standard error; VIF, variance inflation factor.
Regression Analysis of Error, Learnability, Efficiency, Memorability, and Satisfaction of Usability Analysis
The Influence of Error, Learnability, Efficiency, and Memorability of Usability Analysis on Satisfaction
p<0.01
In sum, effort expectancy, relatives' influence, error, and memorability have significant influences on users' behavior intention and satisfaction (Fig. 5). For emerging technology products and services like telehealthcare, consumers attach critical importance to usability and the operating system interface. How relatives are cared for also influences their behavior intention. In consequence, stakeholders should ensure that older adults understand how to use the equipment during the initial stages of implementation if they are to successfully promote use of this technology among that demographic.

Verification of telehealthcare technology acceptability model.
Discussion
Smart devices promise to improve telehealthcare services at low cost. In Taiwan's telehealthcare market, the devices should enable better communications between the cared-for, caregivers, and doctors. They may also enable rapid, timely medical intervention, averting unnecessary admissions to hospitals. Unfortunately, the problems with smart device usability and user experience have been documented, and in response telehealthcare service designers should incorporate user-oriented equipment designs, manufacturing, and operation to minimize processing time and avoid the collection and retention of erroneous physiological data. 2,28,29
This study achieved three meaningful results. First, users' behavior intention and satisfaction significantly affected behavior. Second, effort expectancy and relatives significantly affected behavior intention. Third, error and memorability significantly affected satisfaction.
Health care professionals felt positive about telehealthcare, whereas participants felt (on many occasions) that telehealthcare led to a reduction in costs in terms of time savings and the avoidance of travel. Although there were key benefits from home telehealthcare, organizational, ethical, legal, design, usability, and other matters need to be resolved before widespread implementation can take place.
Technology is in transition even while it is pervasive. Although telehealthcare equipment is innovative, many of the participants in this study were experienced technology users. They suggested the incorporation of more functions and accessories into a single device. At present, there are people for whom telehealthcare can enhance quality of life. To meet their needs, telehealthcare requires enhanced technology, improved usability, and an expanded scale of services.
In addition, factors related to users' technology acceptance such as ease of use, user satisfaction, and adoption behavior have been found to be significant in meeting users' needs. 32,36,37 The results of this study suggest that one way to enhance the acceptance and adoption of telehealthcare equipment is to improve the overall social background and cognition of users. Government and private enterprises can therefore play a key role in the promotion of telehealthcare. Error and memorability in the operation of equipment can affect satisfaction, and therefore small improvements in equipment operation may greatly enhance users' experience with telehealthcare devices.
From the user's perspective, the study revealed that smart devices were not meeting the needs of elderly patients. Given the findings from literature and user involvement throughout the journey-mapping approach, these views must be addressed. We highlighted that people were made to adapt to the equipment rather than the equipment tailored to meet their needs.
Conclusions
This study used a mixed-methods approach to gather data. The qualitative data provided an in-depth perspective on users' experience of a telehealthcare device. The quantitative data provided perspective on users' technology acceptance. This study provides valuable insight and recommendations to marketers who seek to create positive experiences for telehealthcare device users.
In conclusion, telehealthcare is a viable and necessary evolution in health care for elderly patients in Taiwan, a significant demographic that will include 20% of the population by 2025. However, there are serious limitations to the current field of telehealthcare devices. Essential measurements are missing and key features are not user-friendly. In addition, no consideration has been given to emergency or other critical contingencies. For telehealthcare to become widespread in Taiwan, these limitations must be addressed. Critically, governments will need to act to promote telehealthcare systems if they are to meet the needs of an aging society.
Consequently, this study suggests (1) that the government provide assistance and professional administrative planning with social welfare as the starting point, (2) allocating resources and connecting people with private enterprises so that people could gain user experience with smart devices, and (3) implementing research from the perspective of experiential marketing that could offer a richer understanding of both product development and users' characteristics in the health care service industry.
Footnotes
Disclosure Statement
No competing financial interests exist.
Correlation Analysis of the Study Variables
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) | R | 1 | 0.134 | 0.436 * | 0.074 | 0.212 | 0.196 | 0.397 * | 0.378 * | 0.253 | −0.153 | 0.164 | 0.316 |
| Sig. | 0.466 | 0.013 | 0.688 | 0.244 | 0.281 | 0.025 | 0.033 | 0.0163 | 0.404 | 0.368 | 0.078 | ||
| (2) | R | 0.134 | 1 | 0.471 ** | 0.623 ** | 0.608 ** | 0.420 * | 0.563 ** | −0.006 | −0.039 | 0.550 ** | 0.624 ** | 0.343 |
| Sig. | 0.466 | 0.006 | <0.001 | <0.001 | 0.017 | 0.001 | 0.973 | 0.831 | 0.001 | <0.001 | 0.054 | ||
| (3) | R | 0.436 * | 0.471 ** | 1 | 0.399 * | 0.308 | 0.250 | 0.646 ** | 0.037 | 0.237 | 0.252 | 0.432 * | 0.579 ** |
| Sig. | 0.013 | 0.006 | 0.024 | 0.086 | 0.167 | <0.001 | 0.841 | 0.192 | 0.165 | 0.013 | 0.001 | ||
| (4) | R | 0.074 | 0.623 ** | 0.399 * | 1 | 0.558 ** | 0.432 * | 0.615 ** | −0.059 | −0.206 | 0.486 ** | 0.530 ** | 0.492 ** |
| Sig. | 0.688 | <0.001 | 0.024 | 0.001 | 0.014 | <0.001 | 0.748 | 0.258 | 0.005 | 0.002 | 0.004 | ||
| (5) | R | 0.212 | 0.608 ** | 0.308 | 0.558 ** | 1 | 0.792 ** | 0.550 ** | −0.057 | −0.147 | 0.434 * | 0.422 * | 0.535 ** |
| Sig. | 0.244 | <0.001 | 0.086 | 0.001 | <0.001 | 0.001 | 0.755 | 0.423 | 0.013 | 0.016 | 0.002 | ||
| (6) | R | 0.196 | 0.420 * | 0.250 | 0.432 * | 0.792 ** | 1 | 0.490 ** | 0.166 | −0.199 | 0.150 | 0.199 | 0.515 ** |
| Sig. | 0.281 | 0.017 | 0.167 | 0.014 | <0.001 | 0.004 | 0.363 | 0.274 | 0.411 | 0.275 | 0.003 | ||
| (7) | R | 0.397 * | 0.563 ** | 0.646 ** | 0.615 ** | 0.550 ** | 0.490 ** | 1 | −0.063 | 0.168 | 0.603 ** | 0.795 ** | 0.835 ** |
| Sig. | 0.025 | 0.001 | <0.001 | <0.001 | 0.001 | 0.004 | 0.731 | 0.357 | <0.001 | <0.001 | <0.001 | ||
| (8) | R | 0.378 * | −0.006 | 0.037 | −0.059 | −0.057 | 0.166 | −0.063 | 1 | 0.094 | −0.393 * | −0.302 | −0.134 |
| Sig. | 0.033 | 0.973 | 0.841 | 0.748 | 0.755 | 0.363 | 0.731 | 0.608 | 0.026 | 0.093 | 0.466 | ||
| (9) | R | 0.253 | −0.039 | 0.237 | −0.206 | −0.147 | −0.199 | 0.168 | 0.094 | 1 | 0.192 | 0.090 | 0.206 |
| Sig. | 0.163 | 0.831 | 0.192 | 0.258 | 0.423 | 0.274 | 0.357 | 0.608 | 0.292 | 0.625 | 0.258 | ||
| (10) | R | −0.153 | 0.550 ** | 0.252 | 0.486 ** | 0.434 * | 0.150 | 0.603 ** | −0.393 * | 0.192 | 1 | 0.768 ** | 0.548 ** |
| Sig. | 0.404 | 0.001 | 0.165 | 0.005 | 0.013 | 0.411 | <0.001 | 0.026 | 0.292 | <0.001 | 0.001 | ||
| (11) | R | 0.164 | 0.624 ** | 0.432 * | 0.530 ** | 0.422 * | 0.199 | 0.795 ** | −0.302 | 0.090 | 0.768 ** | 1 | 0.632 ** |
| Sig. | 0.368 | <0.001 | 0.013 | 0.002 | 0.016 | 0.275 | <0.001 | 0.093 | 0.625 | <0.001 | <0.001 | ||
| (12) | R | 0.316 | 0.343 | 0.579 ** | 0.492 ** | 0.535 ** | 0.515 ** | 0.835 ** | −0.134 | 0.206 | 0.548 ** | 0.632 ** | 1 |
| Sig. | 0.078 | 0.054 | 0.001 | 0.004 | 0.002 | 0.003 | <0.001 | 0.466 | 0.258 | 0.001 | <0.001 | ||
p<0.05, ** p<0.01.
(1) Performance expectancy, (2) effort expectancy, (3) social influence, (4) facilitating conditions, (5) behavioral intention, (6) use behavior, (7) error, (8) learnability, (9) efficiency, (10) memorability, (11) satisfaction, and (12) relatives.