
Abstract
Introduction
Solid organ transplantation is a life-saving treatment option for many end-stage diseases. However, it requires strict adherence to immunosuppressant medications, and poor adherence is associated with serious consequences, including graft rejection and mortality. 1 –4 Research has consistently identified adolescents as most at-risk for medication nonadherence. 5,6 The causes of nonadherence in adolescents are multifactorial and exacerbate the burden of the chronic illness. Individual factors that impact nonadherence include disease and medication knowledge, forgetfulness, cognitive abilities, coping, and psychosocial functioning. 7,8 In addition, factors associated with normative developmental tasks of adolescence—establishing autonomy and self-identity, perceived injustice, sense of immortality, peer acceptance, and focus on body image—contribute. 9,10
Research supports multicomponent interventions to improve adherence in adolescents. 11,12 Individual interventions can promote self-monitoring and behavioral modification, utilize problem solving to address barriers to adherence such as peer acceptance concerns, or provide treatment for mental health problems, which can negatively influence adherence. Group interventions decrease the sense of isolation, and the interpersonal context leverages peer influence, which is particularly salient during adolescence. 13 A number of significant challenges exist when hosting group interventions for adolescent patients, including school attendance, other social priorities, and the distance from the medical center since it requires increased time and cost to travel. Few patients who reside outside a metro area can obtain individual or group behavioral health services that are sensitive to unique transplant concerns as these services are largely only available at urban-based medical centers.
Telehealth
Behavioral health provider shortages and practical, psychosocial, and stigma-related barriers to seeking behavioral health treatment necessitate novel ways to provide evidence-based care. Advances in health technologies have allowed care providers to address distance and access issues by using telemedicine to engage patients in any number of individual and group-based models with demonstrated effectiveness and health outcomes. 14,15 Patients are comfortable communicating with providers through telehealth, and most have the required technology. 16 Natural settings, such as the patient's home or school, are optimal settings for telehealth, and more research is needed for conducting home-based therapeutic services through telehealth. 17,18
Children and adolescents are well suited for interactive videoconferencing, 19,20 and telemental health has been successfully conducted with youth across many settings and demographics. 17,20 New interventions for youth with chronic illness have focused on utilizing videoconferencing to increase the possible audience and to appeal to adolescents' interest in technology. 21 –23 Adolescents, as digital natives, are especially well versed in technology use and are, therefore, prime audience members for using technology in interventions. 20,24,25 Hommel et al. have found videoconferening to be feasible and acceptable to youth and caregivers when conducting multicomponent behavioral interventions targeted at improving health behaviors through family interventions. 26 –28 However, to date, there are no telehealth adherence interventions focused specifically on adolescent solid organ transplant recipients.
Studies examining videoconferencing groups are limited to adults, but it is a very promising tool with similar satisfaction, retention of information, attendance, attrition, group cohesion, and effectiveness, especially for patients who struggle with an isolating condition. 17,29,30 Modalities (i.e., interactive videoconferencing vs. face-to-face) have comparable effectiveness and formation of group cohesion, and videoconferencing does not compromise the mechanism of change in group interventions. 29,31 Raymond et al. have piloted an intervention for young adults with diabetes, which included a group appointment with other young adults facilitated by a diabetes educator. 21 The participants reported high levels of perceived support from the peer interaction component of the group intervention. Another study has examined the use of videoconferencing in a school-based clinic with a multifamily group addressing pediatric obesity. 32 The family group was comparable in effectiveness and feasibility with no significant technological problems, suggesting that even with a large group, videoconferencing was an effective medium for treatment. In summary, no videoconferencing groups have been conducted with children, not to mention children with chronic illness or youth with solid organ transplants, specifically.
Purpose of this Study
The purpose of this study was to develop a home-based group telehealth intervention to address medication adherence with adolescent heart, kidney, and liver transplant recipients. This study describes the change in adherence to immunosuppression medication from pregroup telehealth intervention to postgroup telehealth intervention. It also explores the acceptability and feasibility from recruitment through group completion and considers both the participant and facilitator experience.
Materials and Methods
Participants
Solid organ transplant recipients (aged 13–17 years), who had received a heart, kidney, or lung transplant and who had been provided care at our urban-based pediatric hospital, were recruited. Exclusion criteria included the following: (1) non-English-speaking participants and (2) cognitive impairments or severe mental health concerns (e.g., psychosis). Exclusion criteria did not include specific technological requirements; however, some potential participants were excluded as they did not have internet or a webcam. Patient assent and parent consent were obtained, and this study was approved by the institution's review board.
Procedures
This study allowed participants to join the group from any private location using an internet-connected device equipped with a camera, speakers/microphone, and Vidyo™ videoconferencing software, a Health Insurance Portability and Accountability Act-compliant encrypted platform. Before the first group session, each participant partook in an individual orientation session with the facilitator, a licensed clinical psychologist specialized in pediatric solid organ transplant. Participants had the opportunity to practice a telehealth call, and instruction on video group etiquette and privacy standards was provided. Participants received reminder communications before their scheduled group session.
Group Intervention
The group protocol called for a closed, stable, and age-limited group heterogeneous by geography and transplant type. Each telehealth group cycle was limited to six participants to allow for optimal group dynamics and consisted of a 1-hour session delivered once a week for five consecutive weeks (Table 1). The intervention curriculum was designed at the adolescent level and borrows from cognitive-behavioral therapy, motivational interviewing, and the Information-Motivation-Behavior model, using the hope theory as the primary conceptual underpinning of the intervention 33 –35 and promoted the group therapeutic factors of cohesion, installation of hope, altruism, universality, impartation of information, and imitative behavior. 36 As a proxy of acceptability and feasibility, the facilitator tracked attendance and attrition across groups, as well as reasons for missed group sessions.
Transplant Adherence Group Intervention
Medication Adherence
Immunosuppression levels of each patient prescribed tacrolimus were retrospectively identified through chart review. Up to five laboratory measurements of tacrolimus before consenting to the group were collected, and all tacrolimus laboratory measurements were collected from participants for a year after the group intervention. Participants who had at least two measurements of tacrolimus pregroup and two measurements postgroup were included in the analysis of medication adherence. Coefficient of variation (CV) of tacrolimus levels was calculated in the pregroup and postgroup phase for each patient. A Wilcoxon signed-rank test was used to test for differences in the CV of tacrolimus from pre- to postgroup.
Participant Experience
To assess acceptability, participants were electronically administered a postgroup measure, the Telehealth Group Satisfaction Survey, for which they were compensated with a $10 gift card. This short, mixed quantitative, and qualitative survey was developed to assess participants' satisfaction with the group and the telehealth technology. This survey included 17 questions rated on a 5-point Likert scale rated from “strongly disagree” to “strongly agree.” Questions assessed the degree to which participants liked the content of the group, enjoyed using the technology, had difficulty using the technology, felt supported by other participants in the telehealth setting, would use telehealth again, and overall satisfaction. As suggested by the telehealth literature, 37 13 open-ended free text questions were included to inquire about participant experience of the group and of telehealth, as well as to ask for suggestions for group content or technology. Study data were collected and managed using Research Electronic Data Capture (REDCap). 38 Descriptive statistics were calculated for quantitative data, and grounded theory guided content analysis of open-ended questions to identify themes, capture suggestions for modifications, and provide exemplar quotes. 39
Facilitator Experience
To evaluate feasibility, the facilitator documented obstacles to implementation for each group session. 32
Results
Participants
See Figure 1 for recruitment data. See Figure 2 for the map of consented adolescents. Median distance from the hospital was 56.6 miles (interquartile range [IQR] = 14.2–164.2 miles), and 18 out of 55 (33%) lived >100 miles away from the hospital. Range was from <5 miles from the hospital to >600 miles away from the hospital.
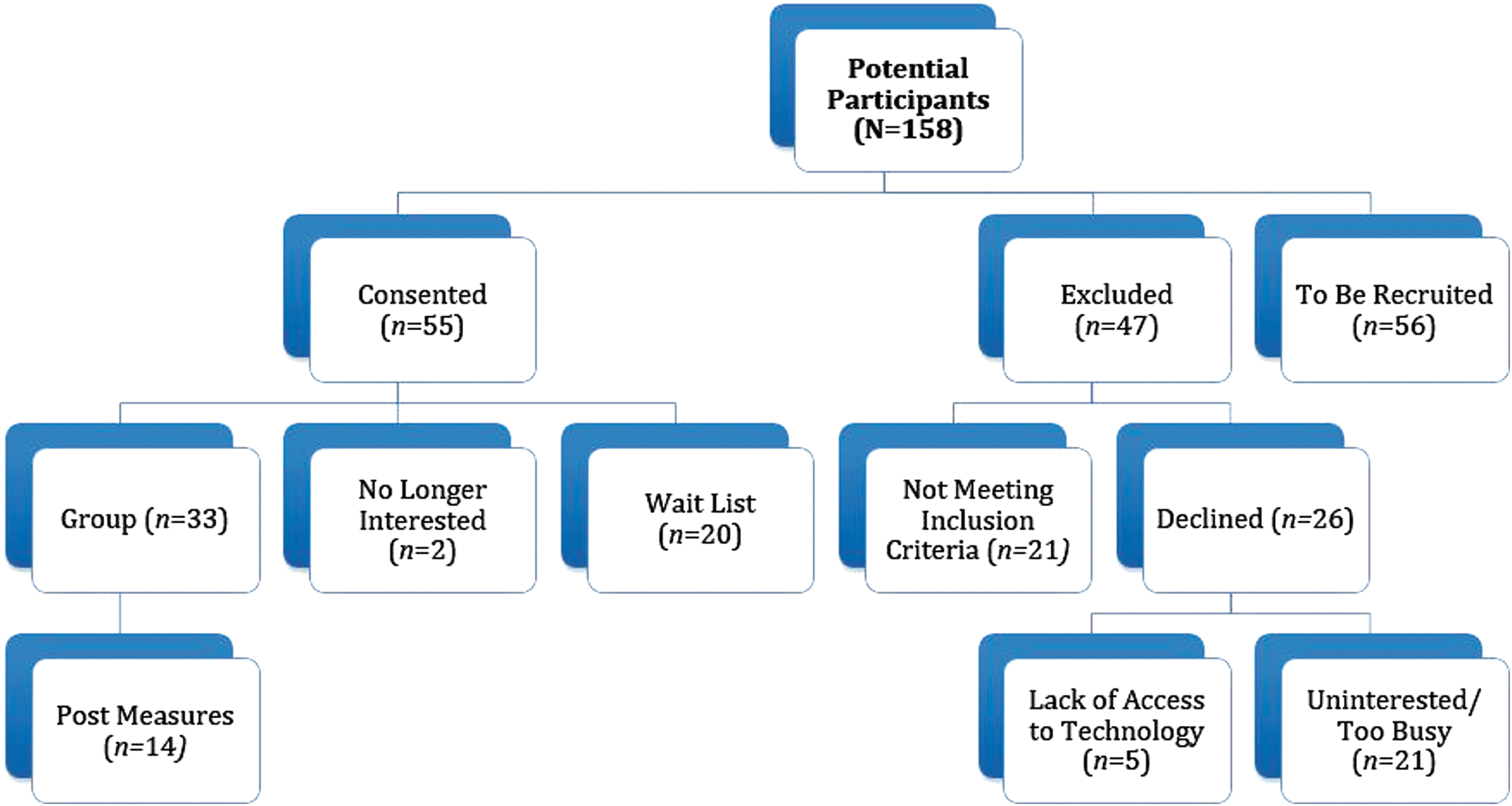
Recruitment.
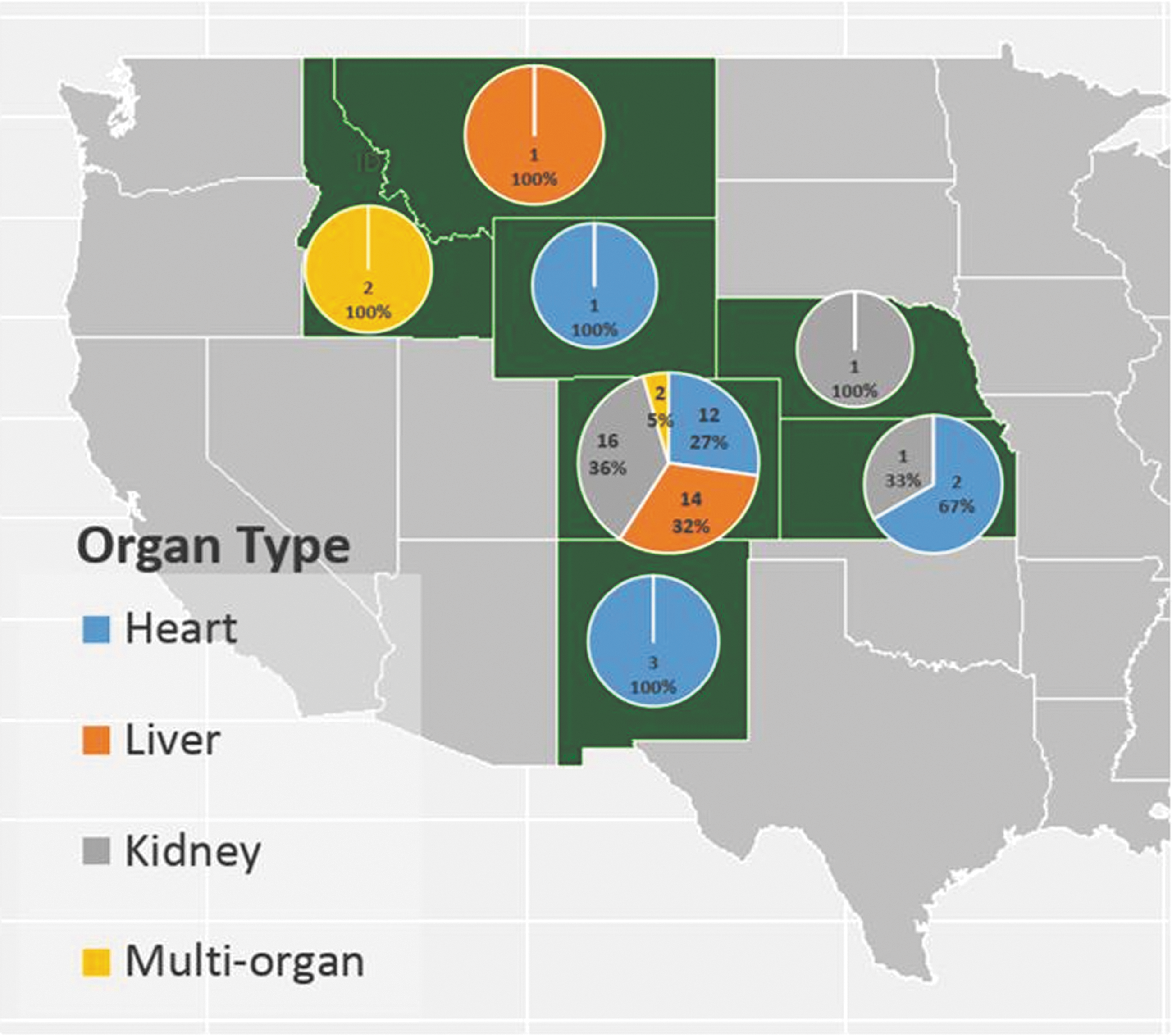
Map of geographic diversity by state and organ type.
Participants included 33 post-transplant group members, with 11 males (33%) and 22 females (67%). The age at the time of consent ranged from 13 to 17 years (mean = 15.2; standard deviation = 1.5). The most common transplant types were heart, kidney, and liver accounting for 30.3% (n = 10) of the sample each, with kidney and liver double-organ transplant accounting for 9.1% (n = 3). Time since transplant to first group visit ranged from 2 to 192 months (mean = 90.7; median = 74.3). The majority of participants were Caucasian (76%), whereas a small number of patients were African American (3%), Asian (3%), or multiracial (18%), with 18% endorsing Hispanic descent. Insurance type included private insurance (55%), Medicaid/Medicare (36%), Tricare (3%), and other (6%).
Seven groups were completed and ranged from three to six participants with an average of 4.71 participants per group. With five sessions per group across 33 participants, there were a total of 165 possible group sessions, with 105 completed group sessions (Fig. 3). Participants attended an average of 3.18 sessions out of 5 with 7 participants attending all 5 sessions of their group (10 attended 4 sessions, 4 attended 3 sessions, 6 attended 2 sessions, and 6 attended 1 session).
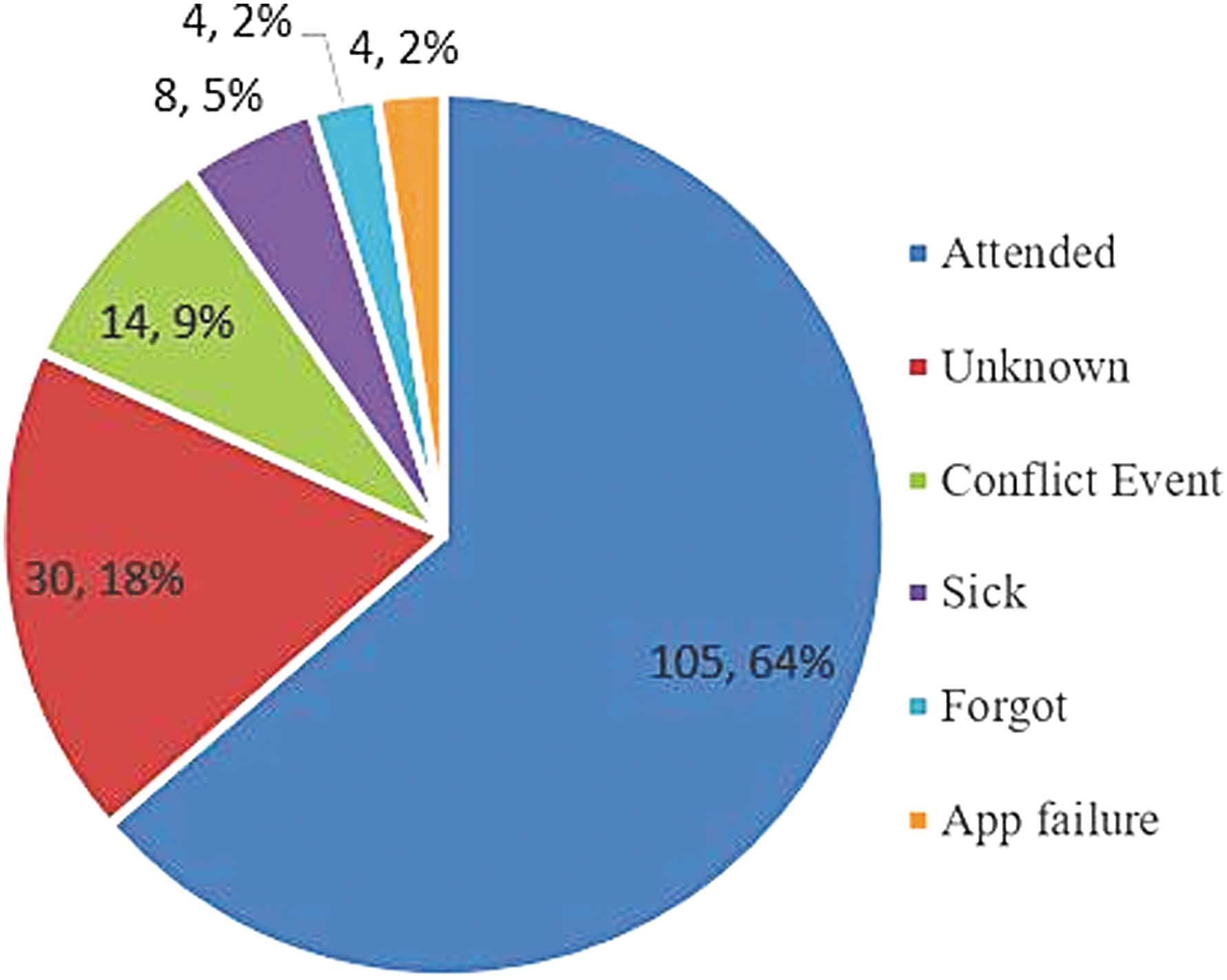
Attendance and attrition across 165 potential group sessions.
Medication Adherence
Seventeen patients (52%) had at least two tacrolimus measurements before enrolling in group and at least two measurements after group completion. Although not significant, the median CV of tacrolimus decreased from pre- to postgroup (median [IQR]: pregroup = 32.2% [25.8%, 39.78%]; postgroup = 23.5% [17%, 29.6%]; p = 0.16).
Participant Experience
Fourteen (42%) participants completed the postgroup Telehealth Group Satisfaction Survey (Table 2). Ten (83%) participants agreed that using telehealth reduced the inconvenience of unnecessary travel, and eight (67%) indicated that telehealth reduced the time missed from school or work. Five participants used a tablet (36%), five used a computer (36%), and four used a phone (29%); five (36%) participants reported that they experienced problems with the technology.
Participant Experience and Satisfaction
Endorsed = answered “agree” or “strongly agree” on Likert scale.
Median (IQR) of Likert scale, where 5 = strongly agree and 0 = strongly disagree.
IQR, interquartile range.
Open-ended answers (Table 3) highlighted the acceptability of the group, the positive aspects of meeting other transplant recipients, the impact on health behaviors, and the positive response to telehealth. Participants provided suggestions for the group content and the technology.
Participants' Open-Ended Responses Coded by Theme
Facilitator Experience and Adaptations
The facilitator identified unanticipated obstacles to implementation with regard to recruitment, group attendance, group participation, and technical difficulties, and adaptations were practiced to optimize group delivery.
First, there were challenges encountered during recruitment. It was difficult to consent participants in person due to infrequent clinic visits of targeted participants; as such, approval was obtained to complete consent over phone. Another challenge during recruitment and at the beginning of each group was attrition. This included participants who consented to the group and then never joined a group cycle despite several attempts to include them in a group. There were also participants who attended the first group and then did not return. This was potentially related to scheduling or organizational difficulties, lack of interest in the group despite consenting to it, or lack of parental oversight and accountability for showing up to the groups since parents are not transporting participants to an in-person group. Considerable effort was made to make each adolescent feel comfortable before participation to address reticence.
Second, there were barriers to consistent group attendance. A unique challenge to feasibility was participant admissions to the hospital during their designated group cycle. This required problem solving, including the need to assess willingness of patients to join the group while admitted, ensuring access to technology, and attempting to minimize distractions from hospital staff. Other challenges to group attendance included participants arriving late or leaving group early due to schedule conflicts, such as social and academic activities. To increase participation, we increased parental oversight in scheduling and sent more frequent e-mail and text reminders.
Participants demonstrated observable evidence of group cohesion and interaction with reciprocal positive feedback between participants. However, a third obstacle identified was group participation. Overall, participation was observed throughout the 105 sessions, with silence noted as an objective issue for 22 (21%) sessions and low interest noted as an objective issue for 24 (23%) sessions. Groups were kept smaller to improve visual display and allow each participant more opportunity to actively participate. However, because of the small size of the group, if participants missed the group, the facilitator needed to adapt to group sessions that may only be attended by one or two participants.
Last, we encountered some technical difficulties that impacted the feasibility of running this group (Fig. 4). Technical difficulties included frozen screens, slow internet connection, and an echo, with one group session terminated prematurely due to persistent technological problems. In addition, the video technology used for this group would highlight the person speaking and frequently change screen view. For example, the person responding would become bigger on the screen than those not speaking and on some mobile devices would be the only screen visible to the participant. To adapt to this feature and because of the delay in audio, the facilitator decreased the amount of vocalizations such as “mmhmm” and limited the use of short reflective responses; thus, it was important to exaggerate the nonverbal communications to show active listening (e.g., nodding and facial expressions).
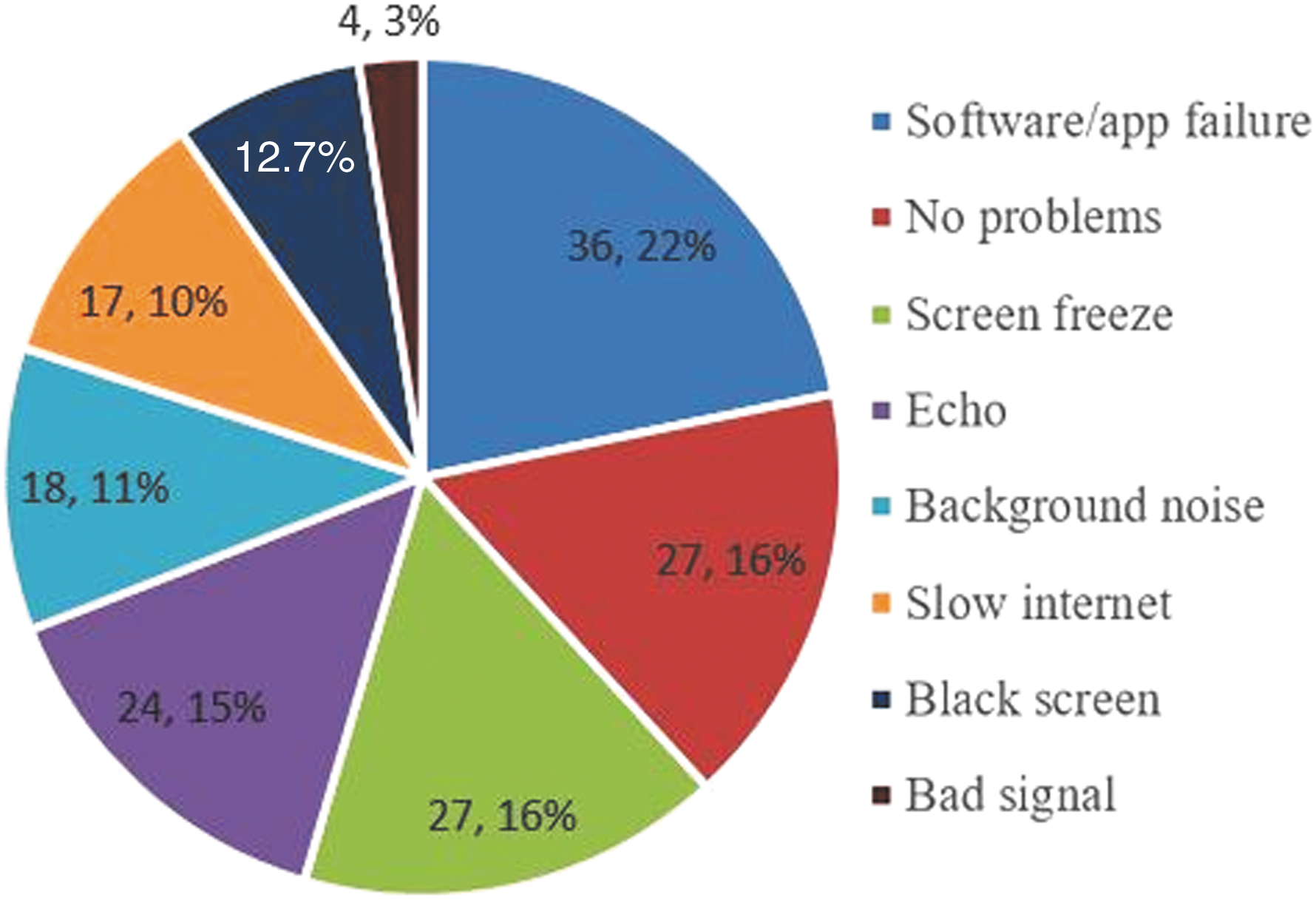
Technical problems across 165 potential group sessions.
Discussion
This home-based telehealth group intervention was acceptable to adolescent transplant recipients and feasible to implement. Participants were recruited across six states with a considerable geographic diversity; it would be very unlikely for many of these teenagers to have access to this type of intervention without telemedicine. Seven groups were successfully facilitated with 33 participants. Although statistically nonsignificant, we observed a decrease in the median CV of tacrolimus immunosuppressant medication, indicating that medication adherence generally improved after the group intervention. This innovative intervention has promising implications for medical outcomes of this vulnerable population.
The majority of participants were satisfied with the format, felt supported by the group members, believed the technology was easy to use, preferred telehealth over traveling to participate, and would recommend this intervention to others. In particular, they reported that the group was acceptable, identifying the connection to other transplant recipients as a salient factor. The group members enjoyed hearing each other's stories and identified with the unique challenges faced post-transplant. Connection and sense of community decreases isolation, normalizes challenges to decrease distress, and allows opportunities for both informational and emotional support regarding their shared identity as adolescent transplant recipients. 40 The participants described ways the group helped promote health behaviors, such as improving their adherence to their medication regimen. Suggestions included allowing more time for open-ended discussion and offering in-person group meeting opportunities.
The study was generally feasible; there were obstacles that would be universal for an adolescent group, regardless of modality, and there were obstacles that were telehealth specific. Several adaptations helped increase recruitment, improve attendance, and bolster group participation, although attrition after consent remained a barrier. The most commonly encountered technical difficulties were software issues, screen freezes, and audio problems. Many of the complications may be mitigated with funding for enhanced technical support and providing participants with internet and equipment.
Lessons Learned
We offer lessons learned across recruitment, group content, and technology considerations. Telephonic consent was crucial to timely recruitment of our geographically diverse patient population. Even so, additional engagement strategies are needed to recruit more male participants, or perhaps modifications to group structure or content are needed (e.g., offering an all-male group option). Youth also benefited from an orientation session that helped them to anticipate what the technology and the group would be like to increase comfort and confidence. Having parents involved in some aspects of the group, such as recruitment, scheduling, and accountability for attendance, was helpful, but teens enjoyed the opportunity for independent participation in the group with other peers. Frequent reminders from the facilitator across different communication streams addressed concerns for forgetfulness or lack of organization, improving attendance, and also decreasing challenges associated with small group size. Although optimal group size in-person may be larger (e.g., 7–9 participants 36 ), smaller groups were ideal for the audio and visual display. Incentives are helpful for measure completion, but may not have effect on attendance.
A strength of the group format is that it provided the necessary foundation for education and interventions, but it remained flexible to organic member interaction and feedback. The content of the intervention is certainly important, but participant responses highlighted that they appreciate some unstructured time to connect and spend together without agenda. The videoconferencing modality allowed for rapport between participants as well as with the facilitator, and connection to others is likely a key contributor to effectiveness.
With facilitator experience, modifiable technological challenges decreased, whereas less predictable technology obstacles will continue to arise. Although we recommended using a computer or tablet for the group, many utilized a mobile phone, typically due to the lack of access to a larger device. Mobile use is accompanied by some inherent limitations, such as a smaller screen that limits participants' ability to see and be seen by others. This also further emphasized the importance of the facilitators minimizing their use of short reflective responses and exploring the options related to software default settings to decrease the frequency of screen shifts. Owing to the teens' familiarity with technology, they had little difficulty naturally making accommodations for themselves. However, youth occasionally utilized cellular data rather than wireless internet, as recommended. A consideration would be to require a specific internet capacity or specific equipment as part of the inclusion or exclusion criteria for the group; yet, this may limit participation and prevent those with limited resources from benefiting from participation. Tablets and internet hotspots would allow universal access to a telehealth group. If this is not possible, arranging for local clinic or community sites where teens could access technology for the group would be another potential solution. Having a dedicated IT support can help decrease user, device, or internet barriers to smooth communication.
Limitations
The threats to the internal validity relate primarily to the selection of participants. We benefited from a small convenience sample of participants who already belonged to pre-existing groups (e.g., transplant time, availability for the group, and internet access at home), and a face-to-face control group would not be feasible given the distance of teens' residence from the hospital. As with other adherence research, there may also be a selection bias as more adherent teens may be more available for consenting and more likely to participate. Furthermore, socioeconomic status may have impacted both access to internet and device. Lastly, identification of teens who would be best served by telehealth versus other interventions (such as in-person therapy groups), alternative recruitment strategies, and modifications to the group format (e.g., open enrollment groups, booster sessions, and increased number of sessions) may increase sophistication of group design and utilize precision medicine strategies. 41
Generalizability is limited due to the small sample size, and results may not be applicable to other demographic variables and international populations. Generalizability of the telehealth platform is limited by patient and provider technical competence. Furthermore, given that multiple participants were from out of state, limitations to broader application outside of the research context are impacted by reimbursement and licensure across state lines. 42
Overall, results of this study are promising and support the continuation and expansion of the intervention, as well as encourage ongoing implementation of home telehealth services as a way to match patient preferences as well as address barriers to access to quality behavioral health care.
Footnotes
Acknowledgment
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure Statement
No competing financial interests exist.