
Abstract
Background:
It has been suggested that patients with anorexia nervosa (AN) who are resistant to first-line treatment would benefit from second-level interventions targeting specific features, an adaptive form of intervention. Guided self-help programs administered via mobile technology have the dual focus of instigating behavior change and managing anxiety associated with eating disorders in the moment and in users' naturalistic environments.
Introduction:
We evaluated the feasibility, acceptability, and preliminary augmentative effects of mobile-based, guided self-help interventions (Recovery vodcasts) after initial unsuccessful first-line treatments for patients with AN.
Materials and Methods:
Patients with AN who were unsuccessful in their treatments were recruited to access Recovery vodcasts as augmentation treatment for 3 weeks in Korea. Acceptability and feasibility of the intervention were evaluated, and qualitative feedback was collected. Preliminary treatment effects of adding the Recovery vodcasts were assessed, including eating disorder pathology, anxiety and depression symptoms, and body mass index.
Results:
The Recovery vodcasts were acceptable for patients with AN. The patients' psychopathologies of eating disorders improved with augmentation of the vodcasts in their first-line treatments. In addition, there was a tendency toward improvement of affective symptoms. The participants' feedback suggested that the intervention could be improved.
Conclusions:
The study demonstrated that the Recovery vodcasts were well accepted by Korean patients with AN. Moreover, augmentation of the Recovery vodcasts could facilitate improvements in psychopathology of eating disorders, anxiety, and mood symptoms for patients with AN.
Introduction
It has been suggested that patients with anorexia nervosa (AN) who are resistant to first-line treatment may benefit from an adaptive form of intervention. 1 There is an interest among researchers in adaptive interventions, which allow for more individualized treatment and possible augmentation of intervention options (i.e., intervention type and/or dosage) over time. 2 This approach is based on the notion that individuals differ in their responses to intervention. This conceptualization has two components: (1) intervention is individualized based on the characteristics and specific needs of participants; and (2) intervention may be adjusted over time; that is, it will continuously be modified in response to participants' ongoing performance and changing needs. 3
Many adults with AN are chronic, debilitating, and at severe enduring stage of illness, 4 with a poor response rate to current treatments. A new paradigm for treating such patients has been advocated, in which treatment centers on improving the quality of life, minimizing distress, and increasing hope for future. 5 This recovery-based approach has been endorsed by people with eating disorders. 6 One way that this approach has been done is through recovery stories. 7
The National Institute for Clinical Excellence (NICE) guideline recommends that eating disorder services should provide support and care for all known AN patients in contact with specialist services, whether or not these services have a specific intervention in mind, and even in cases where the patient has refused intervention. 8 Support should include psychoeducation about the disorder as well as monitoring of weight, mental and physical health, and any risk factors. Anxiety, low motivation, and social difficulties predict a poor response to inpatient care, 9 suggesting that patients exhibiting these symptoms may be optimal recipients of supplemental interventions such as programs for guided self-help. Guided self-help programs administered via mobile technology have the dual focus of instigating behavior change and managing anxiety associated with eating disorders in the moment and in users' naturalistic environments. 10 These strategies have previously been shown to support behavioral changes in people with eating disorders. 11
Treasure and colleagues have developed a guided self-help intervention for AN that relies on the principles of a recovery-based approach (i.e., inspiring hope, connectedness, and change) combined with the components of cognitive-behavioral approaches (i.e., psychoeducation and anxiety reduction through relaxation training), which were conveyed through a series of video clips (“vodcasts”). 10 The initial tests with the vodcasts to support eating among the adult outpatients in United Kingdom showed promise in terms of feasibility, acceptability, and effectiveness. 12 Next, following further consultation with patients and clinicians in the United Kingdom, a directory of vodcasts and a written workbook to support change was developed targeting illness-maintaining factors using information gathered through interviews with patients who recovered describing the process of change. 13 The recovery-oriented vodcasts were preferred by outpatients more than the inpatients, which suggested that mobile-guided self-help had the potential to engage outpatients with AN in behavior changes. 14
The current study was conducted to examine the feasibility, acceptability, and preliminary augmentative effects of the Recovery vodcasts for Korean patients with AN to determine whether the intervention can benefit patients from a non-Western culture. Our hypothesis was that those who did not respond to their initial intervention would benefit from the augmentation of the Recovery vodcasts.
Materials and Methods
Participants and Recruitment
A total of 22 patients with AN or atypical AN were recruited from the outpatient clinic of Seoul Paik Hospital in South Korea. An AN diagnosis was confirmed using the Structured Clinical Interview 15 based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). 16 All of the participants had taken the first-line (psychological and/or pharmacological) treatments since their first visit to the clinic. The first-line psychological treatments included specialist supportive clinical management (SSCM), Maudsley model of anorexia treatment for adults (MANTRA), and family-based treatment (FBT). MANTRA is an empirically-based cognitive interpersonal treatment linked to underlying obsessional and anxious/avoidant personality traits that are central to the prolongation of AN. 17,18 The treatment has a clear structure and hierarchy of therapeutic procedures described in a patient manual. 19 The SSCM treatment 20 combines features of clinical management and supportive psychotherapy. Clinical management includes education, care, and support, while fostering a therapeutic relationship that promotes adherence to treatment. Supportive psychotherapy aims to assist the patient through use of praise, reassurance, and advice. Additional therapy content was determined by each patient. FBT encouraged families to work out for themselves so as to best help their adolescents with AN to return to a healthy weight. FBT is a three-phase treatment, in which the first phase is characterized by attempts to absolve the parents from the potential guilt they may feel for the onset of the disorder and by complimenting them on the positive aspects of their parenting. 21 During the second phase, parents were counseled on how to help their child in an age-appropriate manner to transition back to healthy eating. The third phase focused on establishing a healthy relationship between the adolescents and their parents. In this study, FBT was centered around a therapist manual. 22
After assessment at first visit, patients who agreed for regular visits to the clinic received MANTRA, while the patients who couldn't visit regularly received SSCM. Patients below the age of 18 received FBT. Each psychotherapy session was ∼50 min long and delivered as weekly individual therapy; FBT was provided twice per month after the initial phase.
The inclusion criteria were: (1) outpatients with AN or atypical AN, (2) ≥16 years old, and (3) unsuccessful response to first-line (psychological and/or pharmacological) treatments. Unsuccessful response was defined as low compliance and frequent no-shows without reasonable excuse or no improvement in body mass index (BMI) for over a minimum of 8 weeks despite continuous treatment. The exclusion criteria were: (1) acute medical risk requiring immediate inpatient treatment, (2) a BMI <13.5 kg/m 2 , (3) severe comorbidity (e.g., psychosis), and (4) suicide risk. All participants were fully informed of the purpose and nature of the study. Participants on a steady prescription of antidepressant medication for a minimum of 4 weeks were eligible for inclusion into the study (n = 12). Figure 1 presents a consort diagram describing the participants' adherence to the study. Out of the 22 participants who were approached for the study, 4 dropped out during the course of the study; 3 explained that they had no time to come for intervention or assessment, and contact was lost with 1 participant. Thus, 18 patients completed the final assessments.
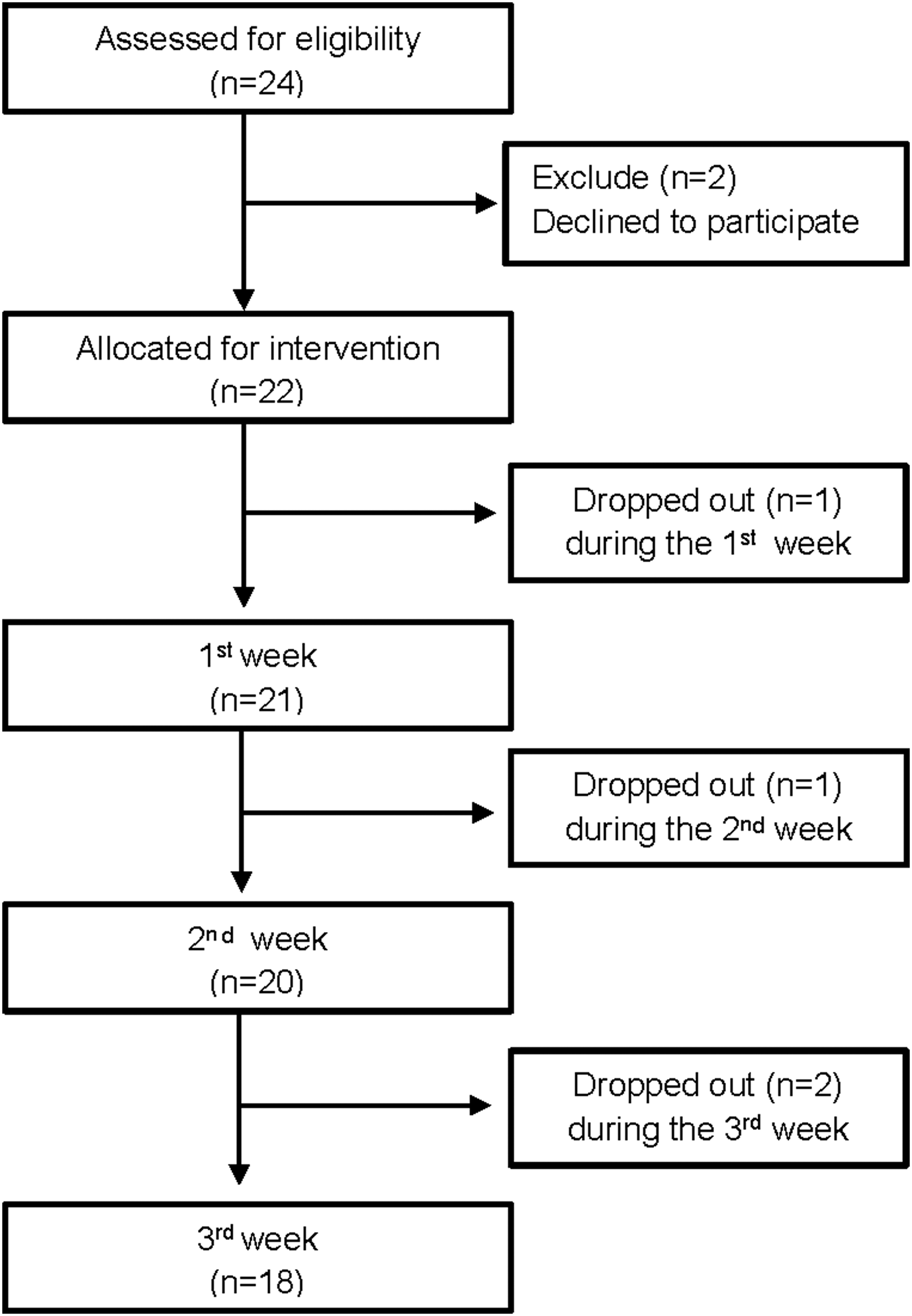
A consort diagram describing participants' adherence to the study.
The study was approved by the Institutional Review Board at Seoul Paik Hospital of Inje University (IRB-2016-203) and was registered with the Clinical Research Information Service (
Recovery Vodcasts
Treasure and colleagues have produced recovery stories in the form of 2–3-min videos (illustrated audio clips named “Recovery vodcasts”) that describe recovery tips from people who have dealt with eating disorders in the past. 10 The films were overlaid with images that complimented the topic of the film. Thus, the voice but not the original images of the contributed were retained. The Recovery vodcasts addressed the cognitive, emotional, and interpersonal components that perpetuate the symptoms of AN. 17 They were provided as an augmentation to the patients' usual treatments in the study. The Recovery vodcasts were played using a portable movie player (PMP).
In tailoring the contents to Korean patients, the narrations in the vodcasts were dubbed into Korean, after being translated into Korean by the authors and reviewed by a bilingual psychologist whose first language is English. Korean subtitles were also used in the vodcasts. Our focus group of people who have recovered from AN reviewed the materials and chose 21 vodcasts based on cultural acceptability and ease of understanding for Korean patients (see Appendix Table A1 for the titles of vodcasts used).
Outcome Measurements
Feasibility and acceptability
Feasibility and acceptability of the Recovery vodcasts were assessed using Visual Analogue Scales (VAS) ranging from 1 (not at all) to 5 (very much) for two items: “How much were you able to focus on the Recovery vodcasts?” and “How satisfied were you with the Recovery vodcasts?” In addition, participants were encouraged to provide qualitative feedback on the Recovery vodcasts.
Eating Disorder Examination Questionnaire
The Eating Disorder Examination Questionnaire (EDE-Q) is a 28-item self-report scale that measures the severity of eating-related psychopathology on four subscales over a 28-day period. 23 The Korean EDE-Q has been proven to be reliable and valid. 24
Depression, Anxiety, and Stress Scale-21
Depression, anxiety, and stress were assessed according to the Depression, Anxiety, and Stress Scale-21 (DASS-21), 25 a self-report questionnaire containing 21 items.
Positive Affect and Negative Affect Schedule
The Positive Affect and Negative Affect Schedule (PANAS) 26 is a 20-item self-report measurement that measures two separate dimensions of mood using items rated on a five-point Likert-type scale. The Korean PANAS has been proven to be reliable and valid. 27
Clinical Impairment Assessment
Functional impairments were assessed using the Clinical Impairment Assessment (CIA). 28 The CIA includes three subscales for symptoms of personal, social, and cognitive impairment with higher overall scores and subscale scores (“personal,” “social,” and “cognitive”) indicating higher severity of impairment.
Visual Analogue Scales
Unpleasant body feelings were measured using a Likert scale ranging from −5 (none) to +5 (very unpleasant), with 0 being “neutral” as assessed by a previous study using vodcasts. 14 Distress related to eating disorder was measured using a Likert scale ranging from 0 (none) to +7 (very distressed).
Procedure
Participants were given instructions on how to use the self-help materials (vodcasts on PMP, vodcast menu, and daily monitoring forms). They were then asked to choose vodcasts that best matched their needs, view each vodcast as much as they could, and reply to the daily text messages from the researcher for the next 3 weeks. A weekly face-to-face guidance meeting (a 30-min session) was scheduled with a researcher experienced in working with eating disorder patients to discuss the use of vodcasts.
All patients were routinely assessed, measuring their height, weight, EDE-Q, and DASS since their first visits to the clinic for treatment of their eating disorders. After enrolling in the study, the participants took assessments involving a clinical interview, self-rating questionnaires (EDE-Q, DASS, CIA, VAS, and PANAS), and measurements of height and weight. After the 3-week intervention with vodcasts, the participants repeated the same assessment procedure and completed the final assessments to estimate the intervention's feasibility and acceptability with two VAS and a qualitative feedback form.
Statistical Analyses
Thematic analyses were conducted from qualitative data and synthesized into major themes that were identified. Three positive and two negative themes were found. The percentage of participants who mentioned the themes is presented.
Repeated-measures analyses of variance (rANOVA) with time (first visit, enrollment, and end of intervention) as a factor were conducted on BMI, EDE-Q, or DASS. If there was a significant effect of time, a post hoc test was carried out with Bonferroni correction. As subsidiary analyses, variables that were measured only at enrollment and end of intervention (CIA, PANAS, unpleasant body feelings, and self-reported distress) were analyzed using paired t-tests. The results of the differences are presented as mean and effect size if appropriate (Cohen's d for paired t-tests, partial eta squared for rANOVA). 29 Two-tailed t-tests were used, and p values <0.05 were considered significant. All statistical analyses were done using SPSS version 22.0 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.).
Results
Clinical Characteristics of Participants
Table 1 shows the clinical characteristics of patients with AN. They had a mean age of 25.27 ± 8.53 years, and their mean BMI was 16.93 ± 2.69 kg/m 2 at enrollment. Their mean age of onset was 18.32 ± 4.57 years, and the mean duration of illness was 7.34 ± 8.55 years. According to the BMI criteria in DSM-5, 8 patients were at extreme (<15 kg/m 2 ), 1 at severe (15–15.99 kg/m 2 ), 2 at moderate (16–16.99 kg/m 2 ), and 11 at mild (≥17 kg/m 2 ) stages of illness severity. Eighteen participants (81.8%) had psychiatric comorbidities at the time of enrollment.
Clinical Characteristics of Each Patient with Anorexia Nervosa at Enrollment
Drop-out over the study period.
Alcohol, alcohol use disorder; bipolar, bipolar disorder; FBT, family-based treatment; MANTRA, Maudsley model of anorexia treatment for adults; OCD, obsessive compulsive disorder; OCPD, obsessive compulsive personality disorder; PD, personality disorder; SSCM, specialist supportive clinical management.
The participants' mean BMI at the time of their first visit to the clinic was 16.85 ± 3.36 kg/m 2 , and the mean time elapsed between the first visit and enrollment was 45.61 ± 55.28 (range 13–244) weeks. Seventeen patients had psychological treatments (SSCM, MANTRA, or FBT) as first-line treatments. The mean number of sessions of psychotherapy was 13.00 ± 11.63 (range 4–43) for SSCM, 8.75 ± 9.50 (range 4–23) for MANTRA, and 5.50 ± 1.00 (range 4–6) for FBT. Five patients had been given only pharmacotherapy (antidepressants) as first-line treatment without psychological treatments.
Usage, Feasibility, and Acceptability
Participants reported using the vodcasts for 74.2 ± 50.4 (range 17.1–225) min per day for 3 weeks. Figure 2 shows the feasibility and acceptability of vodcast intervention in patients with AN. The acceptability of PMP delivery of recovery stories was assessed by asking about interest and satisfaction with vodcasts. Thirteen participants (72.2%) reported they found the vodcasts satisfying and of interest.

Bar graphs show how the participants rated
The qualitative analyses of participants' feedback for the intervention resulted in three positive and two negative themes. The positive opinions were that the vodcasts provided emotional support (43%), treatment accessibility (11%), and appropriate information regarding eating disorders (10%). Meanwhile, the negative opinions included boredom from repeated viewing of vodcasts (32%) and inconvenience of device usage (4%).
Changes in Psychopathology of Eating Disorders and Affective Symptoms Through Use of Recovery Vodcasts
Table 2 shows the effect of Recovery vodcasts on various outcome measures, including psychopathology of eating disorders and other affective symptoms. Results from rANOVA revealed significant differences on the global score (Δη 2 = 0.59; p = 0.001) and all subscales of the EDE-Q over the course of intervention. Post hoc paired comparisons with Bonferroni correction showed that all subscales of EDE-Q had significant reductions following the implementation of vodcasts. There were borderline significant differences in the results from rANOVA on affective symptoms (Δη 2 = 0.31; p = 0.053), including depression (Δη 2 = 0.30; p = 0.055) and anxiety (Δη 2 = 0.31; p = 0.050) subscales over the period of intervention.
Eating Disorder Psychopathology, Affective Symptoms, and Clinical Impairments at Three Time Marks: First Visit, Enrollment into the Intervention, and End of 3 Weeks Intervention
Data are shown as mean (SD).
The mean duration from first visit to enrollment (preintervention) was 45.61 ± 55.28 weeks.
Analyzed with repeated-measures analyses of variance.
Analyzed with paired t-tests.
Means with different superscript letters are significantly different from each other at p < 0.05 in a Bonferroni post hoc comparison.
BMI, body mass index; CIA, Clinical Impairment Assessment; DASS-21, Depression, Anxiety, and Stress Scale-21; EDE-Q, Eating Disorder Examination Questionnaire; PANAS, Positive Affect and Negative Affect Schedule; VAS, Visual Analogue Scales.
There was a large-sized reduction in distress related to eating disorders (d = 1.57; p = 0.001), a medium-sized reduction in negative affect (PANAS; d = 0.50; p = 0.021), and a small-sized improvement in unpleasant body sensations (d = 0.37; p = 0.040) and social function (CIA; d = 0.44; p = 0.027) after the augmentation of vodcasts. There was no significant change in BMI over the study period.
Discussion
The aim of this study was to examine the feasibility and acceptability of adapting treatment to include recovery-orientated self-management materials in the form of vodcasts for Korean patients with AN who had failed to respond to their first-line psychological and/or pharmacological treatments. We found that adding the Recovery vodcasts was feasible and acceptable for these patients. A majority of participants found the treatment acceptable, although some found the requirement to view each vodcast three times a day to be boring. The results suggest that Recovery vodcasts may be of use as an augmentation therapy. In addition, the intervention was associated with changes in eating disorder psychopathology and affective symptoms but not in BMI over the course of the study.
Though the findings of the study were largely positive, a few limitations should be considered. First, we had a small number of subjects. Future studies need a larger sample size. Second, the design of this study was limited due to lack of a comparison group. Third, the intervention used in the present study was an abridged version of what was originally developed. The full recovery-based intervention of the Maudsley model of treatment for adults with anorexia nervosa (iMANTRA) 30 includes workbooks and over 60 vodcasts. The lack of accompanying workbooks may have reduced the effectiveness of vodcast intervention. Also, we selected only a small number of original vodcasts that we found to be most applicable to Koreans, but including a wider variety may have broadened the applicability and made the intervention less boring. Fourth, our intervention program lasted only 3 weeks, although the iMANTRA described in Self-Help and Recovery Guide for Eating Disorders (SHARED) program is 6 weeks long, 30 which is being currently carried out in the United Kingdom. Thus, the duration of the study may have been too short to demonstrate improvements in other symptoms such as BMI. However, it might not be a significant limitation of this study, considering that the aim of this study was to look at feasibility and acceptability. Finally, the PMP provided for vodcast intervention was more inconvenient to use than an iPad or a smartphone. This may have contributed to boredom, since a web platform or an app that introduces more gamifying elements may offer more engaging possibilities.
In summary, we suggest a treatment plan informed by the recovery approach that utilizes recovery stories with treatment goals that focus not only on weight gain alone but also on social functioning and quality of life. The findings here may be of value to the advancement of treatment of AN. The present study indicates that an adaptive approach with the addition of Recovery vodcasts was acceptable and feasible for Korean patients with AN.
Footnotes
Acknowledgments
This work was supported by a 2015 Inje University research grant. We thank Dr. Han Choi for reviewing the script and Mr. Byung Soon Whang for administrating vodcasts via mobile technology.
Disclosure Statement
No competing financial interests exist.
List of Vodcasts Used in the Study
| MODULE | TITLE |
|---|---|
| Introduction | Freedom from Eating Disorders Thoughts |
| Introduction | Theories of Growth |
| Introduction | Focusing on Your Own Goals |
| Introduction | Starting to Take Risks |
| Introduction | A Turning Point |
| Module 1 | Making New Rules |
| Module 1 | Getting Rid of Visual Reminders |
| Module 1 | The Slippery Stage of Recovery |
| Module 2 | Revising Unrealistic Expectations |
| Module 2 | Taking Care of Yourself |
| Module 3 | Can't Doesn't Mean I Don't Want To |
| Module 3 | The Role of Relationships |
| Module 3 | Comparing Myself to Others |
| Module 4 | Staying on Track |
| Module 4 | Preventing a Lapse from Becoming a Relapse |
| Module 4 | Overcoming and Understanding Fear |
| Module 4 | Managing Food Around Others |
| Summary | Carpe Diem! |
| Summary | Recovery as a Journey |
| Summary | Celebrate the Moment |
| Summary | Benefits of Recovery |
Module 1: cognitive area (based on cognitive flexibility and the importance of looking at a bigger picture instead of focusing on the details); module 2: emotional area (based on the importance of positive and negative emotions in response to self and others and their regulation, building self-compassion and self-esteem); module 3: social area (based on reciprocal understanding, strengthening relationships, and on interactions between people with eating disorders and other people); module 4: nutritional area (based on food and brain).