
Abstract
Introduction:
The high prevalence of chronic illnesses is a serious public health problem in the United States, and more than 70 million older adults have at least one chronic illness. Patient portals (PPs) have an excellent potential to assist older adults in managing chronic illnesses; however, older adults' PP adoption rates have been low. Lack of support for older adults using PPs remains a critical gap in most implementation processes. The main aim of this study was to assess the impact of an older adult friendly Theory-based Patient portal e-Learning Program (T-PeP) on PP knowledge, selected health outcomes (health decision-making self-efficacy [SE] and health communication), PP SE and use, and e-health literacy in older adults.
Materials and Methods:
A two-arm randomized controlled trial was conducted with older adults (N = 272) who had chronic conditions. Participants were recruited online, and data were collected at baseline, 3 weeks, and 4 months. The main intervention effects were tested using linear mixed models.
Results:
The average age of participants was 70.0 ± 8.5 years, and 78.3% (n = 213) were white. At 3 weeks, the intervention group showed significantly greater improvement than the control group in all outcomes except PP use. At 4 months, the intervention effects decreased, but PP SE remained significant (p = 0.015), and the intervention group showed higher frequency of PP use than the control group (p = 0.029).
Conclusion:
The study findings showed that the T-PeP was effective in improving selected health and PP usage outcomes. Further studies are needed to test the long-term effects of T-PeP using more diverse samples.
Introduction
The high prevalence of chronic illnesses is a serious public health problem in older adults. 1,2 Approximately 80% of American older adults have at least one chronic condition. 3 People with chronic conditions must manage many health-related tasks (e.g., follow-up on treatment plans and appointments) and communicate with their care providers frequently. Many older adults may also need to share their health information with their family caregivers. Patient portals (PPs) are a robust patient-focused health information technology (IT) program that patients use to access their electronic health records (EHRs) and communicate with providers. Most PPs also include other tools, such as appointment scheduling and medication refill programs. 4,5 Prior findings demonstrated positive impacts of PPs on the management of chronic conditions, 6,7 adherence to treatment plans, 8,9 and patient–provider communication. 10,11 With the recent Medicare EHR Incentive Payment program, 12 PPs are freely available to patients from most health care providers. Currently, PP adoption rates vary in the literature. 13 –15 A meta-analysis of 40 studies reported an overall mean adoption rate of 52%, with markedly varying rates among studies. 13
Older adults are often assumed to use PPs less frequently than younger adults 13,16,17 ; however, a few recent studies have reported that more than 50% of older adults in their samples have PP accounts. 15,17,18 These rates are significantly higher than general older adults in the community. These adoption rates might not reflect actual PP use among this population. 13 When older adults were admitted to hospitals or visited clinics, staff members might have helped them sign up for PP accounts 19,20 because providers needed to meet the requirements for the Medicare EHR Incentive Payment program. 12 Prior studies also suggest that although older adults have PPs, many do not use them because of their unfamiliarity with the technology, insufficient training, etc. 19 –21 Based on a general population survey (2017 Health Information National Trends Survey; N = 3,285), 22,23 only 32.4% of adults aged 50 and older and 27.9% of adults aged 65 and older used PPs (“access your online medical record”).
Despite the rapid increase in older adult online users, many older adults are not technologically savvy and require additional support for learning to use e-health programs. 21,24,25 Currently, most older adults in the community receive little or no PP training support from their providers. This is a critical gap in the nation's health IT initiative because without appropriate support older adults will not be able to use this robust health tool effectively, missing an important opportunity to improve their health. In an effort to fill this gap, in our previous studies 19,26 we developed and tested the older adult-friendly Theory-based PP e-Learning Program (T-PeP) to provide older adults with necessary support for using PPs. The aim of this online trial was to test the effects of T-PeP on selected health-related outcomes and PP use in community-dwelling older adults with chronic illnesses. We hypothesized that participants who used the T-PeP intervention would demonstrate greater improvement than the control group at the end of T-PeP (3 weeks) and at 4 months in PP knowledge, self-efficacy (SE) for using PPs and making health decisions, perceived patient–provider communication, e-health literacy, and PP use (having PP, usage frequency).
Theoretical Framework
T-PeP was developed and implemented with the guidance of SE theory, which emphasizes the importance of personal beliefs about the ability to perform selected behaviors/tasks (SE) and the expected outcomes from those actions. 27 This theory fits well with the project because older adults will use PPs if they believe that they can use the technology and benefit from it. 28 Older adults' beliefs about the health outcomes of using PPs can be a good motivator. 27,29 SE theory describes four sources of efficacy beliefs 27 : (1) successful performance of the behavior; (2) social persuasion; (3) modeling others' successful performances; and (4) relief of emotional stress (e.g., technology anxiety). These sources of SE were provided through various components of T-PeP, such as web modules (text, video, and pictures) and discussion forums. For example, participants were encouraged to set goals based on the content they learned through modules and share their success stories and/or challenges on the discussion board. In the modules, they were informed of potential difficulties with technology and were provided help desk support.
Methods
Design and Participants
This was a two-arm parallel-group randomized controlled trial comparing the T-PeP group with the no-intervention control group. The study was approved by the Institutional Review Board at the University of Maryland, Baltimore.
Individuals were eligible if they were aged 50 or older with at least one chronic disease (e.g., heart disease, diabetes, and cancer), * had access to the internet/e-mail, could use the internet/e-mail independently, resided in the United States, and could read and write English. Participants were recruited online from SeniorNet, 32 a leading older adult online organization, that provides adults aged 50 and older with technology education and maintains an active online community 32 (January 17, 2017 to June 23, 2017). It also has 25 learning centers throughout the nation. 32 The members' median age is 60–70 years, and the majority (∼80%) are white. In an effort to recruit more minority participants, we also worked with leaders in three SeniorNet learning centers located in areas with high minority populations and one large retirement center community in Maryland (flyers with the study information were distributed).
A brief description of this study and a hyperlink to the study's website were posted on the SeniorNet website, and it was also advertised through its e-newsletters. Detailed information about the study was provided on the study website (participants from other sites were referred to the study website directly). If an individual decided to participate, he/she clicked on the “Continue to Participate” button and an interactive eligibility criteria form opened. Only those who met all inclusion criteria could proceed to the online consent form. At the end of the consent process, the participant filled out the contact information form, and the project manager contacted the person within 72 h through phone to provide more detailed information about the study. The telephone follow-ups also served as a mechanism to validate the demographic information and cognitive status (e.g., ability to understand the study procedures) of the participant. Upon the follow-up phone call, the participant was placed on a waiting list until ∼40–60 participants (a team) were recruited. Once a team was filled, the participants completed the baseline survey and were randomly assigned to one of the two study conditions (T-PeP or control) using a block randomization method.
Measures
Demographic and descriptive variables
Demographic variables included age, sex, education level, and health conditions (e.g., chronic illnesses). Internet experience was assessed by years of use and mobile device use. In addition, participants were asked about their experiences with PP training, about their sources of PP information (registration desk, doctors, nurses, etc.), about type of information (none, brochures, instructions on the web, etc.), and one open-ended question.
Outcome measures
Specific outcome measures included PP knowledge, SE for PP use and health decision-making, patient–provider communication, and PP use. In addition, the level of e-health literacy was assessed using the e-Health Literacy Scale (eHEALS), an eight-item measure on a five-point Likert scale with scores ranging from 8 to 40. 33 This tool has been used in prior studies with older adults and shown to be internally consistent and valid. 34
PP knowledge was assessed using an eight-item questionnaire developed by experts and tested in other studies. 19,26 The items focused on how to obtain the accounts and their functions, and the calculated alpha of the measure in this study was 0.54. 19
PP SE was assessed using a modified four-item Self-Efficacy for Computer-Based Personal Health Record (PHR) scale of the PHR Self-Efficacy tool. 35 The original scale assesses three areas of PHR competency (general PHR SE, SE for paper-based PHR, and SE for computer-based PHR) on an 11-point Likert scale (0, not at all confident; 10, very confident). The validity of the measure was assessed using criterion validity testing. 35 The scale was tested in our prior study, 19 and its calculated alpha was 0.88.
SE for health decision-making was assessed using the Decision Self-Efficacy Scale, including nine items on a five-point Likert scale (0, not confident; 4, very confident). The scale assesses the person's ability to obtain information, ask questions, and make a choice. 36 –38 Two items on the original scale were not included because they were beyond the scope of PP functions. The scale was tested for older adults in an e-health study (α = 0.83; criterion validity). 39
Patient–provider communication was assessed using the three areas of the Components of Primary Care Index 40,41 : interpersonal communication, provider's knowledge about the patient, and care coordination, including 12 items on a 5-point Likert scale (1, strongly disagree; 5, strongly agree). The original scale assesses four areas, including “patient preference to see the usual doctor.” The three areas were chosen because they are associated with communication between the patient and the provider. The validity of the measure was examined using factor analysis, 41 and its calculated alpha was 0.88. 19
PP use was assessed using the number of patients who had PP account(s) and the frequency of PP usage reported in the scheduled surveys.
Intervention: T-Pe P
The 3-week T-PeP was developed for older adults to learn to use PPs to manage their health. It explains how to sign up for the PPs, use different PP functions, give access to other persons, and use PPs to better manage their health (See Table 1 for detailed content.) T-PeP includes learning modules, moderated discussion boards, and a virtual library (VL). Considering variations in the types and usability of PPs nationwide, T-PeP was developed as a vendor-agnostic (“not tied to a specific vendor”) program. The T-PeP was tested in our prior studies. 19,26 For the current study, the content was further refined and expanded, including more short demo videos of specific PP functions. Participants were encouraged to use those functions in their own PPs and share their experiences through discussion forums. A discussion forum accompanied each module, and trained nurse moderators facilitated the discussions. The VL included links to other helpful sites that included relevant information.
Learning Modules and Topics
EHR, electronic health record; PHR, personal health record.
The password-protected T-PeP was developed using our established e-health intervention platform. The program was developed to be older adult friendly following the National Institute on Aging (NIA) guidelines. 42 Web pages (e.g., learning modules) were developed using the SoftChalk™ program, 43 which accommodates various mobile devices using optimized design. The Blackboard (BB) e-learning program, 44 the upper layer of the web architecture, helped structure learning content and provided discussion boards. The traditional BB user interface was redesigned to simulate a regular web page. 44 The BB program also controlled user access and facilitated group-based online trials by allowing duplication of the intervention site and scheduled release function.
Procedures
After randomization, the intervention group participants started using T-PeP. The instructions and course schedule for the program were posted on the study website. A new learning module and an accompanying discussion forum opened on the T-PeP website weekly for 3 weeks, and an e-mail notification was sent to participants. Participants were encouraged to visit the T-PeP website at least once a week to review the new module and share their thoughts and experiences on the discussion boards. The nurse moderator facilitated the discussions and monitored them daily to identify any untoward postings. Participants could further explore PP-related topics and selected health information using the VLs.
No specific intervention was provided to the control group participants, but at the end of the trial, they had access to T-PeP for 3 weeks. All participants completed an online follow-up survey at the end of 3 weeks. To maintain contact with participants, an e-mail informing them of upcoming follow-up surveys was sent monthly. An incentive of a $20 check was mailed to participants who completed the 3-week survey and another $20 check upon completion of the 4-month survey.
Fidelity Monitoring of the Intervention
Participants' use of the learning modules and discussion board was monitored weekly through the usage reports generated from BB. Monitoring was performed per module and per group because new modules and discussion forums opened weekly and groups were on different study schedules. Program usage was based on the frequency of visits (captured by logins) to each component.
Data analysis
Descriptive analysis (mean, standard deviation [SD], range, frequency, and proportion) was conducted on each variable to describe the sample and check the assumptions on the models used for the main analysis. Baseline differences between the intervention and control groups were examined on demographic characteristics, health conditions, and baseline outcome scores using t tests for continuous variables and chi-square tests for categorical variables.
The intent-to-treat approach was adopted in the primary analysis. Linear mixed models (LMMs) were used to compare the differences of changes in continuous outcomes between the T-PeP group and the control group. Generalized LMM with binomial distribution was used for the binary outcome (i.e., having a PP). For each outcome, LMMs included a random intercept to account for correlation between the repeated measurements. The fixed effects included group (T-PeP vs. control), time indicator variable (baseline, posttreatment, and/or follow-up), and the group-by-time interaction term. The significance of the group-by-time interaction tested whether the change (baseline to 3 weeks or baseline to 4 months) differed between T-PeP and control conditions. 45 We used empirical “sandwich” standard errors due to their robustness properties. The ordinal logistic regression model was used to compare the frequency of PP usage at 3 weeks and at 4 months within group included in the model. Within-group effect sizes were calculated as the model-based difference of the outcome from baseline to 3 weeks and from baseline to 4 months, divided by baseline SD, respectively. Between-group effect sizes were calculated as the model-based difference in change divided by the pooled SD of the outcome at baseline. 46
There was a difference in attrition rates between the T-PeP and control groups (18.1% T-PeP vs. 5.2% control for 3 weeks; 17.4% T-PeP vs. 6.7% control for 4 months). The attrition was more likely for those with lower computer knowledge, with lower education, and who were not married, as well as those with frailer health (e.g., heart and lung problems). Thus, as a sensitivity analysis, we refit the mixed-effect models using model-based standard errors (SEs). Under normality, using model-based SEs, results in tests are less likely to be biased to the extent that the “missingness” of outcomes is dependent on observed data (i.e., baseline outcome measurements). 45 SAS 9.4 was used for the analysis. 47
Within the intervention group, we also assessed the potential effects of T-PeP usage on the changes in major outcomes (“dose effects”) using LMMs. The fixed effects included time, usage (sum of frequencies of module, discussion board, and VL use), and time-by-usage interaction. A random intercept was included to account for the correlation between repeated measures within each participant. The significance of the interaction term indicated the effects.
Power calculation
Sample size calculation was based on the repeated measures. Initially, a sample size of 242 (121 per group) was calculated based on detecting a small-to-medium intervention effect (Cohen's d = 0.2748), assuming the correlation among the repeated measures as 0.7 and an overall attrition rate of 20%. In an effort to oversample the minority participants (10%), the sample size was increased and a total of 272 participants were recruited.
Results
Demographics
A total of 473 individuals who visited the study website completed the online eligibility form. Among those, 160 did not meet the criteria, 16 declined to participate, and 25 submitted the consent form but did not start the study (Fig. 1, CONSORT diagram). A total of 272 older adults from 29 states participated in the study. The participants were randomized into either the T-PeP (n = 138) or control (n = 134) group. After intervention, 240 participants completed the 3-week survey, and 239 completed the 4-month follow-up survey.
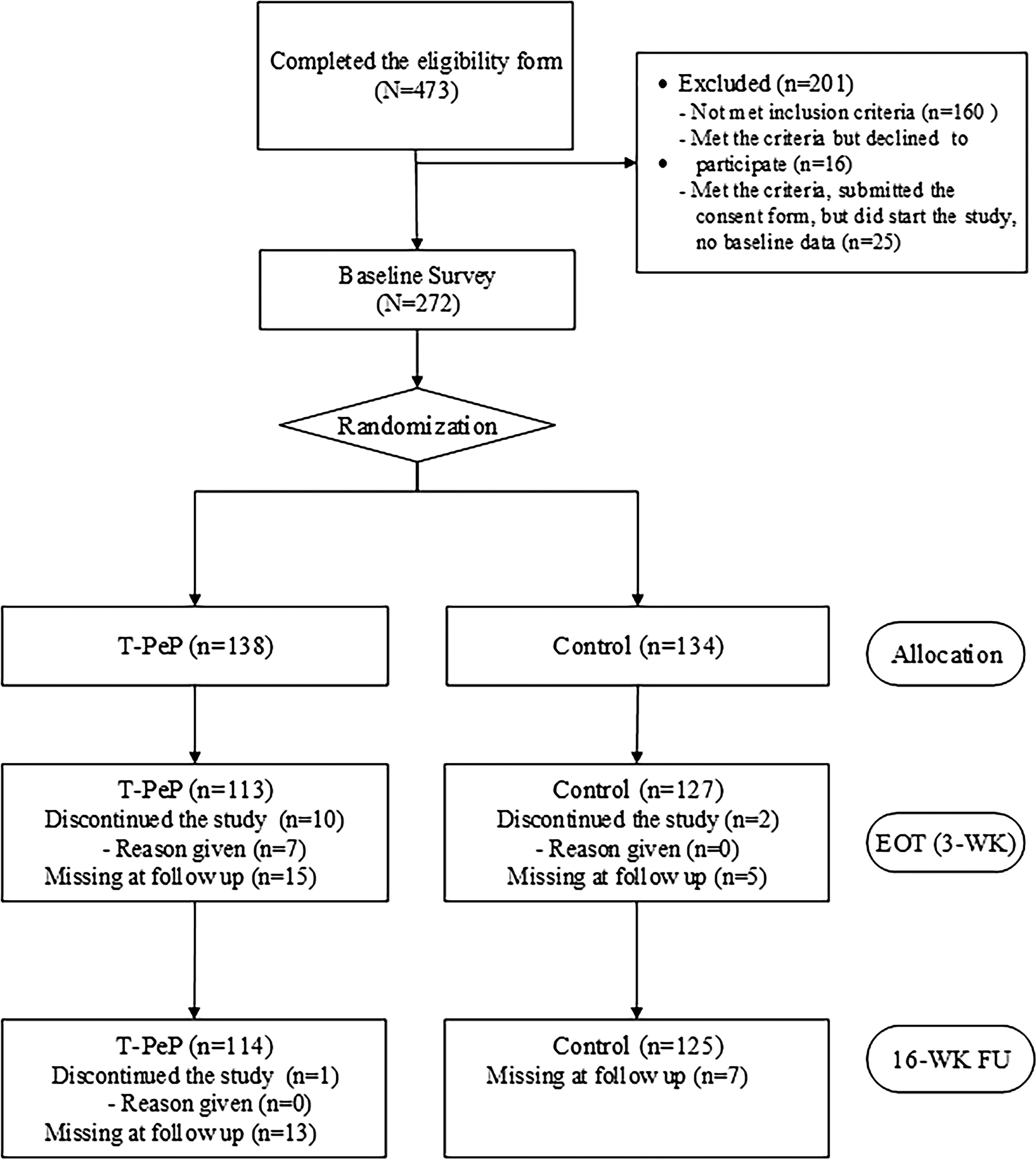
CONSORT diagram showing the flow of participants through each stage of the trial.
Thirteen participants dropped out of the study (i.e., expressed the wish to stop participating and no follow-up survey sent), and an additional 20 participants did not respond to the 3-week survey (the 4-month follow-up survey was sent), the 4-month survey, or both surveys. Overall attrition rates using the proportion of “missing” participants who did not return the survey were 11.8% (n = 32) at 3 weeks and 12.1% (n = 33) at 4 months. When participant demographics and internet use characteristics were compared between the intervention and control groups at baseline, only one variable (seen physician in last 3 months) was significantly different between the groups, which could have occurred by chance variation.
Table 2 summarizes participant characteristics. The majority of participants were female (n = 191, 70.2%) and white (n = 213, 78.3%), with a mean age of 70.0 ± 8.5 years (range, 50–92 years). Most participants had some college or higher level of education (n = 258, 94.9%). The most frequent chronic illness was high blood pressure (n = 174, 64.0%), followed by arthritis (n = 160, 58.8%) and depression (n = 63, 23.2%). The average years of web experience were 19.3 ± 7.7, and the mean hours spent using the web per week were 22.9 ± 17.1. The majority (n = 213, 78.3%) of participants reported their level of computer knowledge as competent or higher.
Baseline Descriptives and Comparison by Intervention and Control Groups, N = 272
Comparison of means (t test) or proportion (χ 2 ) between intervention and control groups.
Chronic conditions with >15% are included.
SD, standard deviation.
The majority (n = 194, 71.3%) reported having at least one PP account at baseline, with a mean of 2 ± 1.2 (range, 1–6). The majority of participants who had PP accounts received the information about PPs either through their health care providers (n = 101, 52.1%) or registration desks (n = 72, 37.1%). About half of participants (n = 96, 49.5%) learned to use PPs through information on web pages, and 35.1% (n = 68) learned through brochures or printed instructions. About one quarter (n = 49, 25.3%) of participants received no training. A total of 170 participants submitted comments on their experience with training. Among those, 55 participants commented that they received no instructions or were self-taught, and 23 participants reported receiving minimal information. (More in-depth analysis on older adults' current PP usage has been published elsewhere). 20
Outcome Measures
Table 3 presents the group means and SDs for outcome variables at baseline, at the end of treatment (3 weeks), and at 4-month follow-up. Table 4 presents the results of primary LMM analyses examining the differences of changes in outcomes from baseline to 3 weeks and from baseline to 4 months. Overall, the T-PeP group had greater improvement than the control group for most of the outcomes at the end of intervention, but the intervention effects reduced at 4 months. Results of the sensitivity analysis were similar to the main analysis.
Group Means and Standard Deviations at Baseline, Posttreatment, and Follow-Up of the Participants, N = 272
PP usage was measured at 3 weeks and 4 months.
PP, patient portal; T-PeP, Theory-based PP e-Learning Program.
Results of Hypothesis Testing from Linear Mixed Models
Coefficient estimation of the group-by-time interaction term in LMM and GLMM or of group term in ordinal logistic regression.
Having PP was estimated through generalized LMM with binomial distribution.
PP usage was compared using ordinal logistic regression models at 3 weeks and 4 months.
LMM, linear mixed model.
At 3 weeks, participants in both the intervention and control groups improved their PP knowledge and PP SE. The T-PeP group showed greater improvement than the control group (t [237] = 2.36, p = 0.019, effect size [ES] = 0.27 for knowledge; t [237] = 3.05, p = 0.003, ES = 0.29 for PP SE). While the control group did not change significantly, the intervention group improved the scores of health decision-making, patient–provider communication, and e-health literacy. Differences of changes between T-PeP and control groups were observed for health decision-making (t [237] = 2.38, p = 0.018, ES = 0.25), for patient–provider communication (t [237] = 2.90, p = 0.004, ES = 0.25), and for e-health literacy (t [237] = 2.49, p = 0.014, ES = 0.27). Having PP account(s) at 3 weeks, an indication of newly activated PPs, did not show significant improvement within each group, nor did it differ between groups. However, the intervention group demonstrated a tendency of higher levels of PP use than the control group (OR = 1.69, p = 0.06) at 3 weeks.
As for the change from baseline to 4-month follow-up (Table 4), most of the outcomes showed improvement within each group but not for between-group differences. The only significant difference was observed for PP SE (t [476] = 2.43, p = 0.015, ES = 0.23), and the frequency of PP use among T-PeP group was higher than among control group (OR = 1.79, p = 0.029).
Fidelity Monitoring of the Intervention
During the trial, an overall of 83.3% of intervention group participants used the T-PeP. The mean usage (frequency) of the program (e.g., the learning modules, discussion boards, and VL) was 22.7 ± 26.7 times. The main analysis of this study used an intent-to-treat approach. We, however, used LMMs to compare whether the amount of T-PeP usage affected outcomes of the intervention group. No significant effects were found for any of the outcome variables in this study.
Discussion
The findings from the study suggest the effectiveness of the T-PeP in improving older adults' PP use for their health. To date, there has been no national data on older adults' PP use. Our findings from 29 states showed that a large proportion (71.3%) of older adults who used the internet reported having two PPs on average. However, the majority of these individuals received minimal or no training, which may result in ineffective use of PPs. At 3 weeks, the T-PeP significantly improved older adults' PP knowledge and SE but not the number of participants who had PPs or PP usage. PP usage became significant at 4 months, which seems logical as participants might have needed some time to learn to use PPs. These findings are consistent with the guiding theoretical framework of this study, SE theory, 27 and highlight the importance of appropriate training in older adults when technology-based health interventions are used.
In addition, T-PeP improved participants' SE for health decision-making and patient–provider communication, which indicates that PPs can empower and engage patients in their care. Although limited, some prior findings also suggested the effectiveness of PPs on improving patients' health decision-making 49,50 and patient–provider communication. 10 In a cross-sectional survey of veterans (N = 819; mean age, 62 years), older adults perceived secure e-mail messaging as a useful tool for communicating with health care teams. Findings from the analysis of 9,408 PP e-messages sent from patients to 401 surgical providers showed that 339 message threads (67.8%) contained information directly associated with medical decision-making. 50
The positive impact of T-PeP on e-health literacy suggests that PPs are a new e-health technology type that older adult online users can learn. In other words, e-health literacy might not be a suitable outcome for older adults who already have years of internet experience and if the e-health program was developed to improve health outcomes. Learning about PPs can affect both health-related outcomes and e-health literacy on technology. In a prior large online trial (N = 899; mean age, 62.5) that tested the effects of an 8-week online health program that was focused on bone health in older adult online users, 48 findings showed improved selected health-related outcomes but not e-health literacy.
At 4 months, PP SE remained significant (p = 0.015), and PP usage, which was nonsignificant at 3 weeks, became significant (p = 0.029). These findings suggest excellent potential for using older adult friendly online training modules for e-health interventions in health care. With the rapid growth of health IT and mobile technologies, future health care will use more technology-based interventions, and provision of appropriate levels of user training is vital. Specifically, older adult training needs must be met as older adults are major consumers of health care services. To date, health care informaticians have mainly focused on evaluating and implementing health IT systems for staff use. These staff also need to be trained to consider patient training as part of their implementation strategies.
Overall, the intervention effects on other outcomes (knowledge, SE, health decision-making, and perceived patient–provider communication) attenuated at 4 months, which is consistent with other behavior findings. In fact, many behavior management interventions (e.g., weight control) have used short-term intensive interventions followed by long-term maintenance sessions (“boosters”). 51 –54 Some trials that applied this approach in online settings 55,56 reported effectiveness of the booster interventions. 57,58
Throughout the study, older adults' receptiveness to and willingness to adopt PPs were confirmed. We were able to recruit 272 older adults within a 6-month period, and the attrition rates exceeded our expectation (11.8% at 3 weeks and 12.1% at 4 months). In addition, findings on the number of PP accounts that current older adults have were insightful. Until now, the nation has paid little attention to using PPs for older adults. Considering the volume of health care services that older adults use and the number of providers they have, PPs offer many opportunities for managing and improving the health of this growing population.
Generally, the magnitude of intervention effects in the T-PeP intervention showed small-to-medium ES for most outcome variables (range, 0.25–0.29). ESs within each group (T-PeP, 0.14–0.62; control, 0.12–0.35) were higher than those in between groups. Several prior studies also reported similar findings. 59 –61 Based on meta-analysis reports, 59,60 online interventions were efficacious in changing health behaviors; however, their ESs were often small (<0.2). Theory-based approaches, additional communication with participants, and just-in-time reminders have been shown to improve the effects of online interventions. 59,60
Limitations
A major limitation of the study is the generalizability of the findings related to the sample characteristics. Participants were recruited online, and the majority of them were highly educated. Although these participants might have been more familiar with technology than the general American older adult population, they may be representative of the rapidly growing older adult population that is online. In addition, we made efforts to engage more minority participants and included 21.7% of minority participants, which is close to the national racial distribution. 62 The data were collected using self-reported online surveys only. In future studies, inclusion of actual data from PPs would result in more robust outcome data. Due to the project time line, we could not assess the long-term effects of the intervention. In future trials we plan to examine the effects of long-term interventions on long-term health outcomes.
Conclusion
Currently, a large number of older adults are living with multiple chronic illnesses, and management of their health in the community is a public health problem. Although PPs have great potential to engage these individuals in self-management, little is known about older adults' use of PPs. The findings of this study show that a large number of older adults have PP accounts, with little training, and that the T-PeP is effective in improving their knowledge and use of PPs, health decision-making, and communication with their providers. Further studies are needed with more diverse older adult samples and to test the program's long-term effects.
Footnotes
Acknowledgment
This study was supported by Grant R21HS024739 from the Agency for Healthcare Research and Quality.
Disclosure Statement
No competing financial interests exist.