
Abstract
Background:
At-home attending intensivists often must return to the hospital to assist residents.
Introduction:
To determine if using telemedicine communication between in-house pediatric residents and at-home attending intensivists impacts the rate of attending return to the hospital and improves resident education.
Methods:
In this single-center prospective study at an academic children's hospital's pediatric intensive care unit (PICU), 40 patients younger than 18 years were randomized into video or telephone arms. Residents and intensivists completed anonymous surveys after each encounter. Video-conferencing encounters between residents and at-home, on-call intensivists were compared with standard telephone calls for admissions to PICU.
Results:
Video and telephone arms had 21 and 19 patients enrolled, respectively. Data comparison was performed using Mann–Whitney U, chi-square, and Kruskal-Wallis analysis. Clinical illness severity rating for intensivists and residents was not significantly different for video communication compared with telephone (p = 0.63 and p = 0.42, respectively). Intensivists reported no significant difference in ease of use (p = 0.87). There was perceived improvement in resident education with the use of telemedicine (52.6% vs. 76.2%; p = 0.11).
Discussion:
Video communication was easy to use but did not change the rating of illness severity or need for intensivist to return to the hospital. There was perceived improvement in resident education with the use of telemedicine, and it may serve as a useful tool in demonstrating acute clinical changes to out-of-hospital intensivists.
Conclusions:
Larger-scale studies in teaching hospitals with out-of-hospital pediatric intensivists need to be conducted to further evaluate the role of telemedicine in patient management and resident education.
Introduction
Telemedicine is the “remote delivery of health care services and clinical information using telecommunications technology.” 1 Telemedicine has been used for several decades and shown to have significant advantages. Specifically, within the critical care setting, telemedicine has allowed rural and community hospital emergency departments (EDs) to access critical care specialists when managing acutely ill patients. 2 However, the overall effect of telemedicine on resident education remains unclear. 3 Studies have shown that respiratory distress is the most common reason that outside hospitals consult pediatric critical care specialists via telemedicine. 4,5 Non-children's rural and community hospitals frequently lack the experience and training to treat critically ill pediatric patients. Patients who present to hospitals without pediatric expertise may be at risk of safety issues or unnecessary intervention. Telemedicine increases access to pediatric specialists and can be utilized in a variety of clinical situations. It has been shown to improve a variety of outcomes, including mortality, morbidity, and length of stay, when used for EDs and pediatric intensive care unit (PICU) patient transfers. 6 Attending physician perception, patient-centered outcomes, and cost-effectiveness of telemedicine have all been described as benefits of telemedicine.
Adult intensive care units (ICUs) began integrating tele-ICU systems of various forms in 2000. Since then, there has been variable growth in its implementation. The number of hospitals using tele-ICU systems increased from 16 (0.4% of total) to 213 (4.6% of total) between 2003 and 2010. 7 Many large centers use alerting systems to detect early physiologic deterioration and reminding systems to address best practices. Studies on adults showed improved patient outcomes in terms of lower mortality and length of stay. 8
This study examines the use of telemedicine communication between pediatric residents and attending intensivists who take out-of-hospital overnight calls. As of 2017, there were 193 pediatric residency programs in the country; however, only 65 have critical care fellow staffing overnight, and many units have out-of-hospital intensivist coverage. 9 Few pediatric studies have evaluated the difference in clinical assessment and intervention when using telemedicine compared with standard telephone communication in an ICU setting with pediatric patients. There is also minimal research on how this could serve as an education tool. While becoming standard in adult medicine, a true electronic ICU (eICU) model does not exist in any form in pediatric critical care. This study creates a rudimentary eICU model in which pediatric residents at the bedside of ICU patients admit, monitor, and communicate with attending physicians at home via a telemedicine platform.
The objective was to determine if using telemedicine communication with in-house pediatric residents impacts the rate of return of pediatric intensivists to the hospital when taking overnight calls from home. A secondary aim explored whether video conferencing impacted the comfort level and educational benefits of the resident physicians who work in this model.
Materials and Methods
This single-center prospective study was IRB-approved and conducted at a community children's hospital with a pediatric residency program. Parents provided informed consent for their children's participation in this study. Study participants were aged 0–18 years. Child and youth assent was attempted when appropriate according to age and clinical status. Patients were excluded if family consent was not given or if the attending intensivist was already physically present at the time of admission.
Patients were randomized into video or telephone arms via secured envelope. Communication with the on-call intensivist was made via video telemedicine or standard phone communication for new admissions or clinical deterioration of existing admitted PICU patients. iPads (Apple, Cupertino, CA) were used to conduct telemedicine via a secure Wi-Fi connection and a Health Insurance Portability and Accountability Act (HIPAA)–compliant software application (Vidyo, Hackensack, NJ). Encounters were not recorded. When a patient was enrolled under the telephone arm, the resident and intensivist communicated via standard telephone.
After each patient encounter, the attending intensivist and resident on call completed anonymous surveys. Intensivists were sent daily reminder e-mails for completion of online survey, while residents had reminder notes at the PICU resident workstation for completion of paper surveys. All enrolled patients had fully completed intensivist and resident surveys ( Appendix A1 and A2 ).
The survey also evaluated resident perception of education gained from the encounter, comfort level with managing the patient on site independently, and whether there was a need for in-person intensivist response. The Pediatric Index of Mortality (PIM2) score 10 was calculated for each enrolled patient to compare illness severity between the two modes of communication. A few survey questions used Visual Analog Scale (VAS) method for obtaining answers. A VAS consists of a line and two anchors, one at each end. The anchors often consist of verbal materials that mark opposite ends of a semantic dimension. 11 It is often used in epidemiologic and clinical research to measure the intensity or frequency of various symptoms. 12
Forty patients were included in the study between August 2016 and March 2017 (Table 1).
Demographics
Data Analysis
Mann–Whitney U, chi-square analysis, and Kruskal-Wallis tests were used for analysis with p < 0.05 accepted as significant. Means were only used for descriptive purposes and not for analysis of final data.
Results
Video and telephone arms had 21 and 19 patients enrolled over a period of 8 months, respectively (Table 2). Intensivists reported that video and telephone had no difference in ease of use (p = 0.87) (Table 3). Both intensivists and residents had similar clinical illness severity rating between video and telephone (p = 0.63 and 0.42, respectively); hence, there was equal distribution of patients between the two groups. There was also no difference in the length of stay for patients enrolled in either arm (p = 0.87). The residents did report better educational experience when using video communication; however, there was no statistical difference noted (52.6% vs. 76.2%; p = 0.12). Patients in both arms had similar clinical severity as measured by PIM2 score, but, due to small sample size, there was no statistical significance (median = 0.8; p = 0.55). Residents had similar perceived comfort level in managing patients with either forms of communication (median = 10; p = 0.31). The need for procedural intervention was cited as the main reason for attending intensivist to already be in-house (62%) (Table 4).
Comparison of Variables Analyzed Between Telephone and Video Groups
All data computed using Mann–Whitney U test.
Length of stay in the PICU in days.
Scale of 1–10 with 1 being less clinically ill and 10 being highest illness severity.
Scale of 1–10 with 1 being less clinically ill and 10 being highest illness severity.
Calculated by chart review and all data obtained from the first hour of admission.
Scale of 1–10 to rate the ease of use of the chosen mode of communication, 1 being less easy and 10 being easiest.
Scale of 1–10 to rate comfort level in managing the patient with current method of communication, 1 being less comfortable and 10 being most comfortable. Two to six assessed by Visual Analog Scale.
LOS, length of stay; PICU, pediatric intensive care unit; PIM2, Pediatric Index of Mortality.
Comparison of Variables Analyzed Between Telephone and Video Groups
Reasons for Attending Intensivist's In-Person Evaluation and PIM2 Scores
Intensivist decision to evaluate patient in-person based on initial transport call.
Patients requiring invasive procedure or endotracheal intubation upon arrival.
Intensivist presence in PICU from prior admission overnight.
Mandatory presence of intensivist in hospital for all admissions via air transport.
PICU, pediatric intensive care unit; PIM2, Pediatric Index of Mortality.
Intensivist presence accounted for 21 disqualified admissions as they often received new admission alerts before the resident team. There were a total of 81 overnight admissions in this 8-month period, and 20 patients did not meet enrollment requirements (Fig. 1).
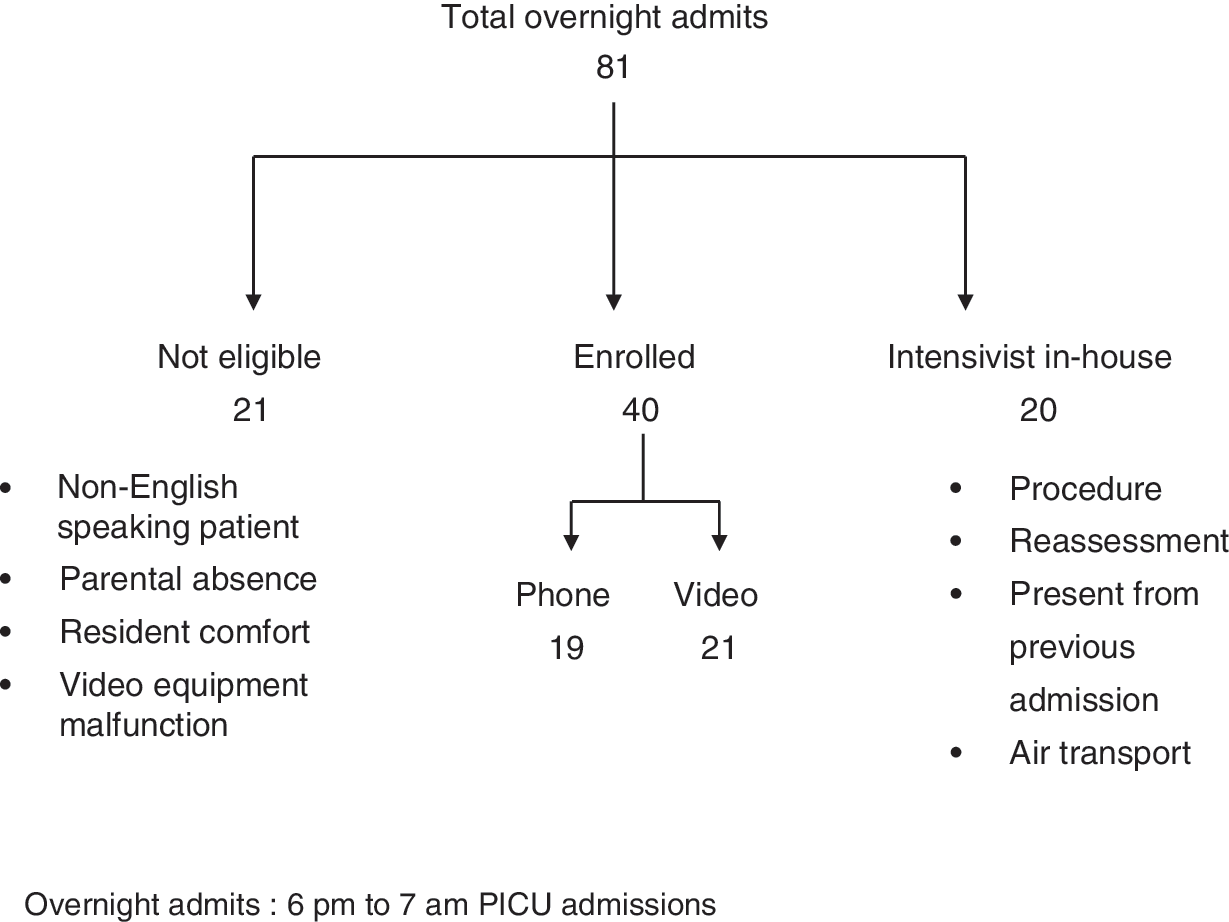
Study design flowchart. PICU, pediatric intensive care unit.
Discussion
This study focused on determining if telemedicine, when compared with standard telephone communication, would have decreased rate of intensivist return to hospital for in-person patient evaluation. The most common reason for attending intensivist's in-house presence was for “procedural intervention,” which included endotracheal intubation, central venous line, or arterial line placement. It is commonly accepted that attending intensivist's presence is required due to the difficulties that can be encountered with pediatric airways and smaller vasculature size compared with adults. This affects the structure of most staffing models in PICUs in the United States and is a likely reason that an eICU model has not been adopted as readily as in adult ICUs, where airway skills in particular are possessed by both physicians and respiratory care staff. However, if an in-house fellow or nurse practitioner with the ability to independently perform these procedures was present, an eICU model with attending intensivist's supervision via telemedicine may prove viable and answer some of the current concerns of physician specialist shortages.
A secondary objective evaluated was the benefit of telemedicine in resident education. This study showed that a larger percentage of residents found video communication more beneficial than phone communication. Although there was no evaluation of knowledge gained from this experience performed, telemedicine communication can be a positive educational experience. This model could be implemented as a tool in PICUs that rely on residents for initial patient evaluation, similar to the one studied. A cross-sectional survey by Coletti et al. of residents rotating through the medical intensive care unit showed similar results with a positive educational experience perceived by residents rotating through an ICU staffed overnight by off-site intensivist. 13 Some theories of why these perceptions exist include direct face-to-face interaction with the attending intensivist, improved attending intensivist's engagement and willingness to teach via a new technology, and a greater sense of resident autonomy. This mixture of remote supervision and autonomy may have resulted in perception of a better educational experience.
Yager et al. 14 showed in their retrospective study that telemedicine use in a PICU model with remote staff intensivists overnight provided continuity of care when the same intensivist was available at night. Further study to identify the continuity effect on patient outcomes is warranted.
In consideration of the technical challenges that often come with new ideas, this study also found that video communications and telephone had comparable ease of use. Technological hurdles are common reasons for implementation failure. Once the initial hurdle of obtaining uninterrupted Wi-Fi connectivity was overcome, the residents were able to connect to out-of-hospital intensivists within seconds. This study suggests that an easy-to-use, reliable software application with prompt IT support and simplified login access can enhance adoption and utilization by staff.
The sample size of the study was a limitation in achieving statistically significant results. The admission volume, resident compliance in enrollment, Wi-Fi connectivity issues, and the study focus to enroll only English-speaking families were major contributors to the small sample size. Another major limitation to the study was the hospital process of PICU admissions, which involved the intensivist receiving the initial intake admission call from the ED, an outside hospital, or the inpatient floor resident. Hence, the intensivist had the opportunity to make the initial decision of coming to the hospital for assessment before having a chance to interact with the PICU resident via video. Knowing this limitation, we evaluated the acuity of study participants by comparing the PIM2 scores between the enrolled and unenrolled group based on the presence of intensivist in the unit. We did find that the more critically ill patients (based on higher PIM2 score) promptly received intensivist in-person evaluation and thus were not enrolled. This suggests that the patients enrolled in the study were of overall lower clinical severity and appropriately did not warrant the attending intensivist's presence. This practice of in-person evaluation decreased our enrollment and led, in part, to the failure to statistically answer whether this rudimentary eICU model has benefit. Table 4 lists the patients who were evaluated in-person with calculated PIM2 scores.
The role of telemedicine is evolving with the development of advanced and reliable applications that provide integrated solutions to hospitals and private practices and increasing patient access to health care providers. Originally used strictly as a communication tool, it has been shown to increase access, improve outcomes, and reduce costs. 8,15
A true pediatric eICU study would need several safety nets in place for success. First, it would need a continuous remote monitoring system staffed by knowledgeable PICU nurses with appropriate alarm guardrails in place. Second, it would require continuous two-way audio and video communication with the patients upon admission. And finally, reliable in-house airway and vascular practitioners for emergency access would be necessary. A study of this kind may prove that intensivists are not needed as often as currently thought, that perhaps they need to be in-house at all times, or that certain circumstances require direct presence while others do not. With growing numbers of PICUs, there continues to be a deficit of intensivist staffing, and an ePICU model may prove to be an important and viable option.
Conclusions
Telemedicine can have comparable ease of use with telephone communication, and there is positive educational benefit in academic setting. However, larger studies are needed to show benefits in the rate of return of out-of-hospital intensivists in an academic setting.
Footnotes
Acknowledgment
This effort was funded by the Nemours Fund for Children's Health.
Disclosure Statement
No competing financial interests exist.