
Abstract
Results:
In total, 100 patients were recruited (smartphone: 5 and pedometer: 50). No significant differences were detected between groups in rates of uptake (80.0% vs. 88.0%, p = 0.28), adherence (92.5% vs. 79.5%, p = 0.12), or completion (76.0% vs. 86.0%, p = 0.20). Physical functions were significantly improved in both groups.
Introduction
Many studies have confirmed that physical activity interventions consisting of aerobic or/and resistance exercise programs promote physical function, reduce fatigue, and improve quality of life. 1 –3 Generally, 150 min of moderate-intensity (50–80% of maximum heart rate) aerobic exercise per week is recommended for cancer survivors. 4
Long-term survival rates are higher in prostate cancer patients than in patients with other cancers. In the United Kingdom, 10-year survival rates have been reported as 83.3% 5 and 98%. 6 Traditional exercise programs for cancer patients are usually performed in scheduled clinical sessions under the guidance of certified exercise professionals. Given the average age range of prostate cancer patients, the associated cost and accessibility of exercise interventions have complicated their practical application in clinical settings. Thus, regular home exercise can help these patients maintain physical function for the duration of their lives.
Conventional monitoring devices such as the pedometer have been effective in promoting home exercise among patients with various diseases, as well as the general population. 7,8 Recent advances in information and communication technologies such as smartphones and the internet have shown the potential for effective home exercise promotion through remote clinical monitoring and consultation. 9 –11
Use of a smartphone application with a wearable measuring device has shown positive effects in changing physical activity behaviors. 12 Smartphone applications can also provide patients with more information about physical activities, dietary advice, and exercise guidelines. 13 –15 A randomized controlled trial of a smartphone-based home-care model revealed that post-myocardial infarction patients had improved participation in cardiac rehabilitation, with higher uptake, adherence, and completion rates than patients following a traditional center-based program. 16
The objective of this study was to compare the effectiveness of smartphone-based and conventional pedometer-based exercise monitoring systems in promoting home exercise among prostate cancer patients. We also compared changes in physical function between groups.
Methods
Study Design
We conducted a prospective, randomized, open-label trial in a hospital in Seoul, South Korea. Patients were randomly assigned to the smartphone and pedometer groups at a ratio of 1:1 using a computer-generated random number table. Many patients did not own a smartphone with an Android operating system; so patient allocation was adjusted according to access to an Android smartphone. Approval for this study was obtained from the Institutional Review Board and written informed consent was obtained from all patients.
Participants
A total of 100 patients were allocated to the smartphone and the pedometer groups. The inclusion criteria were (1) 50 years of age or older, (2) histologically confirmed prostate adenocarcinoma, and (3) treatment with radical prostatectomy, radiation therapy, or androgen deprivation therapy (ADT).
The exclusion criteria were (1) treatment within the past month for other active malignant disease, (2) severe cardiopulmonary disease, (3) bone pain due to bone metastasis or risk of pathologic fracture, (4) inability to perform a 2-minute walking test (2MWT), (5) total knee or hip replacement arthroplasty, or (6) inappropriateness of exercise participation based on a physician's judgment. Patient enrolment and intervention were conducted from August 2015 to January 2016.
Intervention Protocol
The smartphone and pedometer groups engaged in 12 ± 1 weeks of home-based aerobic and resistance exercises. Physiatrists set individual aerobic exercise goals for each participant based on the results of a 2MWT. Resistance exercises were guided by the physiatrist, based on each participant's general and musculoskeletal condition.
Participants with average or longer 2MWT distances for their age group were prescribed 150 min of moderate-intensity aerobic exercise per week. Those with below-average 2MWT distances for their age group were prescribed 90 min of exercise per week. Moderate intensity was defined as a rating of perceived exertion of 11–13 (light to somewhat hard) on the Borg scale, or as activity that increased heart rate and breathing difficulty, while not hindering speaking. Borg scale, or the Borg rating of perceived exertion, is a measurement of physical activity intensity level based on physical sensations a person experiences during exercise. 17 Resistance exercises targeted four to eight major muscles using a Thera-Band (Hygenic Corporation, Akron, OH). Participants were directed to perform 2 sets of 10 repetitions of each exercise twice per week.
At 6 weeks, if participants with a goal of 90 min per week had achieved their goal every week during the previous 6 weeks, their goal was adjusted to 150 min per week for the remaining weeks of the intervention. Participants with an initial goal of 150 min per week were encouraged to continue this exercise level, regardless of goal achievement. Telephone-based consultation was provided to patients performing resistance exercise at week 3. Participants who had successfully performed all prescribed resistance exercise twice per week and could easily perform two sets of exercises were instructed to perform three sets of exercise. At week 6, participants who had completed three sets of exercise more than twice per week during the previous week received a new Thera-Band with increased resistance.
Patients in the smartphone group were provided with a newly developed smartphone application called Smart After-Care® (BIT Computer Co. Ltd., Seoul, South Korea) and a wearable InbodyBand® digital pedometer (InBody Co. Ltd., Seoul, South Korea), which sends data to the application (Fig. 1). Participants in this group were instructed to wear the InbodyBand on their wrists daily, except during sleep. The number of steps and minutes of physical activity measured by the pedometer were recorded by the application at week 1. At the beginning of week 2, the smartphone application provided a weekly goal, based on the 2MWT results. The goal was assigned as a total time per week to be allotted to usual physical activity and prescribed aerobic exercise. For example, if the patient's baseline 2MWT distance was within normal range and the total duration of activity during week 1 was 300 min, the smartphone provided a goal of 450 min per week at the beginning of week 2.

Smart After-Care® smartphone application.
Every week, the achievement rate was displayed on the Smart After-Care application, without distinguishing between usual physical activity and aerobic exercise. The application also provided a video clip of prescribed resistance and stretching exercises. Patients were instructed to enter the number of sets of each resistance exercise they performed. Nutrition information was provided by the application, and participants received weekly feedback consultations about the intervention by telephone.
Patients in the control group received an exercise brochure and diary developed for this study. They were instructed to use a conventional pedometer to record the number of steps and minutes of physical activity performed, and to record the number of resistance exercise sessions performed weekly. These records were checked by clinicians at weeks 6 and 12 ± 1 during follow-up visits.
Outcome Measures
The primary outcome measures used in this study were uptake, adherence, and completion of exercise intervention using a smartphone or pedometer from August 2015 to January 2016. Uptake was defined as attending the baseline assessment and uploading or recording at least one set of exercise data. Adherence was defined as uploading or recording at least three sets of data per week for a minimum of 8 weeks during a period of 12 ± 1 weeks. Completion was defined as attendance at the assessment conducted at 12 ± 1 weeks. 18
The secondary outcomes were physical status, including weight, body mass index (BMI), appendicular skeletal muscle mass (ASM), and physical functions, including cardiorespiratory endurance, upper and lower extremity strength, and gait speed. These were assessed at baseline and at 12 ± 1 weeks. Muscle mass was measured using a direct segmental multifrequency bioelectrical impedance analysis system (In-Body S10®; Biospace Co. Ltd., Seoul, South Korea). ASM was calculated as the sum of arm and leg skeletal muscle. Relative skeletal muscle mass index (RSMI) was defined as ASM divided by the square of body height in meters. 19
Cardiorespiratory endurance was assessed by 2MWT performed in a 15.2-m hallway out-and-back course. Patients were instructed to walk as quickly as possible during 2 min and the distance covered was recorded. 20
Upper extremity muscle strength was assessed by handgrip strength using a hand-held dynamometer. Participants were instructed to apply maximal power for 3 s with the shoulder adducted and neutrally rotated, elbow extended, and forearm and wrist in neutral position. The best score for each hand among three attempts was recorded. A 30-s chair stand test and one repetitive measure of knee extension were performed to determine lower extremity muscle strength. In the 30-s chair stand test, participants were asked to sit on a chair (seat height 40 cm, without armrests, but with backrest) with a straight back and both arms folded across the chest. While the examiner counted, the patient was instructed to stand up and sit down repeatedly and encouraged to complete as many cycles as possible within 30 s. 21,22 Finally, gait speed was assessed during a 4-m walk at normal pace.
Statistical Analyses
Data analysis was performed using IBM SPSS® Statistics, v. 24.0 (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.). The uptake and completion primary outcome measures were assessed using an intention-to-treat analysis. Adherence was assessed only in those who completed the program. All three outcomes were estimated in both groups and statistical significance was assessed by a χ2 test or Fisher's exact test. Secondary outcome measures were assessed in participants based on baseline and 12 ± 1 week data. Baseline differences between the two groups were assessed by independent t-tests for continuous variables and χ2 tests for categorical variables. Within-group differences from baseline to 12 ± 1 weeks were analyzed by paired t-tests. Repeated-measures ANOVA (analysis of variance) was performed to assess between-group differences. Statistical significance was assessed at a level of p < 0.05.
Results
In total, 100 participants were recruited for this study. Among the 50 smartphone group participants, 2 were excluded following randomization due to delayed medical history reports that indicated exclusion criteria (Fig. 2). Two subjects in the pedometer group refused to participate in baseline assessment for personal reasons, leaving 48 patients in each group for baseline assessment. No significant differences were detected among baseline characteristics between groups (Table 1, p > 0.05).
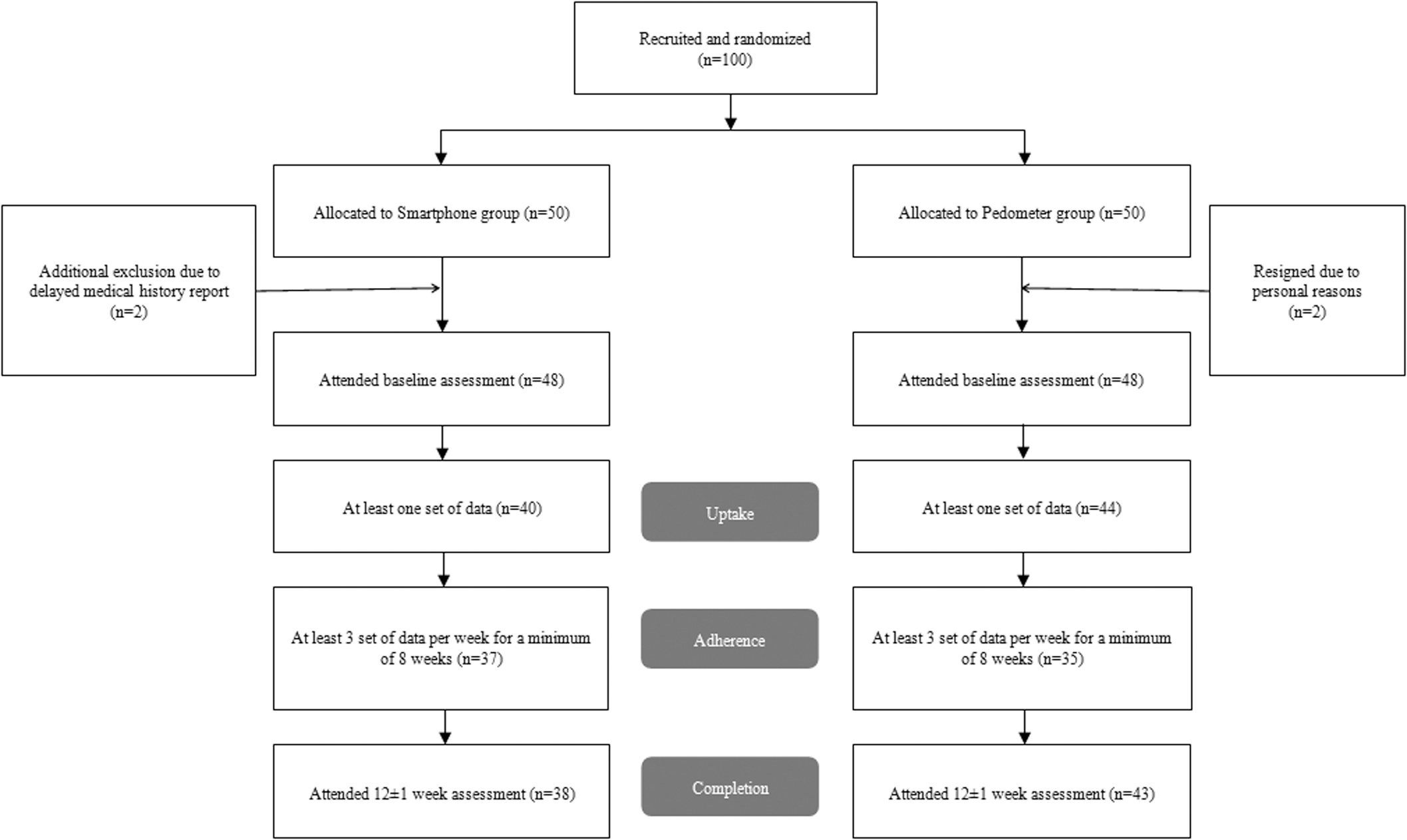
Recruitment process and flow of participants through smartphone-based exercise monitoring and conventional monitoring using pedometer.
Demographic and Clinical Characteristics at Baseline
BMI, body mass index; RM, repetitive measure; RSMI, relative skeletal muscle index.
Primary Outcomes
There were no significant differences in rates of uptake (40/50 = 80.0% vs. 44/50 = 88.0%, p = 0.28), adherence (37/40 = 92.5% vs. 35/44 = 79.5%, p = 0.12), or completion (38/50 = 76.0% vs. 43/50 = 86.0%, p = 0.20) between groups (Fig. 2).
Secondary Outcomes
Table 2 lists the secondary outcomes at baseline and at 12 ± 1 weeks. Most physical functions were significantly improved in both groups. There were significant changes in the smartphone group in all categories, except RSMI between baseline and 12 ± 1 weeks (p < 0.05). There were significant changes in the pedometer group in all categories, except RSMI and grip strength between baseline and 12 ± 1 weeks (p < 0.05). However, none of these changes was significantly different between groups, except weight (p > 0.05). Weight was not significantly different between groups at each time point (p > 0.05).
The Group Difference in Physical Status and Function
p < 0.05, significantly different between baseline and 12 ± 1 week.
Discussion
Our results revealed that the smartphone group had similar uptake, adherence, and completion rates to the pedometer group. Varnfield et al. 18 compared the effect of smartphone-based cardiac rehabilitation with that of a traditional center-based program and observed higher uptake (80% vs. 61.7%, p < 0.05), adherence (93.8% vs. 67.6%, p < 0/05), and completion (80% vs. 46.7%, p < 0.05) rates for smartphone use than for the traditional center-based program. The target diseases differ between that study and ours, making a direct comparison difficult; in addition, patients in that study were approximately 10 years younger than the patients in our study, and young people tend to accommodate new technologies more easily.
Nevertheless, the smartphone group in our study had uptake, adherence, and completion rates similar to the smartphone group in the cardiac rehabilitation study. These similar results indicate that smartphone-based rehabilitation could be an effective method for improving physical activity among patients who cannot easily participate in center-based programs due to economic or accessibility issues.
Regardless of the exercise method, both groups improved in most physical function categories. In a study by Galvao et al., 23 prostate cancer patients with a history of ADT had improved physical function following supervised resistance and aerobic exercise. 23 Thorsen et al. 24 reported promising effects of physical activity on muscular fitness, physical function, fatigue, and health-related quality of life in prostate cancer survivors.
Androgens are important determinants of body composition because they promote lean body mass over fat mass. 25 In contrast, ADT decreases lean body mass and increases fat mass (i.e., sarcopenic obesity). Saylor and Smith 26 reported that ADT decreased lean mass and increased fat mass in prostate cancer patients, and decreased insulin sensitivity, while increasing total cholesterol, high density lipoprotein, and triglycerides. Smith et al. 27 also reported that ADT decreased lean body mass in prostate cancer patients. In this study, both groups had increased body weight, BMI, and body fat; however, RSMI did not change during the follow-up period. We included some patients without hormone therapy and with wide variations in the duration or period of hormone therapy. Thus, it is difficult to determine hormonal effects on changes in physical status or function.
There were a few limitations to our study. First, we did not have an education-only group, and therefore cannot rule out the possibility of improvement by repeated measurement. Second, the intensity of the exercises was assessed subjectively by the patients. Finally, patients were enrolled in only one hospital. However, to our knowledge, this was the first home-based program using a smartphone application to investigate the effects of exercise intervention in prostate cancer patients.
Conclusions
The smartphone-based exercise monitoring system was comparable to a pedometer-based system in promoting physical activity in terms of uptake, adherence, and completion. Exercise monitoring, regardless of the method, was effective in improving physical functions. Further studies involving larger numbers of patients are necessary to fully elucidate the advantages and disadvantages of smartphone-based exercise monitoring systems.
Footnotes
Acknowledgments
This research was supported by the National Information Society Agency (NIA) and funded by the Ministry of Science, ICT and future Planning (Smart After-Care Service for Cancer and Cardiac Disease).
Disclosure Statement
No competing financial interests exist.