
Abstract
Background and Objectives:
There are a few problems restraining the effective operation of telemedicine in China. On the basis of practices of the Henan Province Telemedicine Center of China (HTCC), the purpose of this study was to design a telemedicine system jointly driven by videoconferencing and data exchange to address the issues limiting the further development and implementation of telemedicine.
Methods:
Based on service-oriented architecture, the organizational design of the telemedicine system was gradually refined from top to bottom to complete its hierarchical layout. Technologies including multiprotocol stack adaptation, self-adaptive multilink network transmission, information exchange of heterogeneous medical systems, and open application system architecture were also used to construct the system.
Results:
The telemedicine system realizes the integration of videoconferencing, data acquisition and exchange of heterogeneous medical information systems, and the actual applications and expansion of telemedicine services. The HTCC currently covers more than 500 telemedicine centers, workstations, and service points, forming a five-level “province-city-county-township-village” telemedicine network linkage. The HTCC handles nearly 30,000 teleconsultation cases per year, helping patients save about ¥120 million Chinese Yuan RMB (approximately US $17.5 million).
Conclusions:
The proposed telemedicine system achieves satisfactory operation effects, along with social and economic benefits. It has the potential to increase the coverage of medical resources in remote regions, and it can play a role in solving other problems facing telemedicine development in China. The findings also inform measures for further improvement in telemedicine's implementation effects, service quality, and application scope in China and globally.
Introduction
Although there is no uniform definition, telemedicine mainly refers to the use of modern information and communication technologies to construct a network-based information platform to connect medical institutions, health care professionals, and patients in remote regions. 1 Its main purpose is the cross-regional exchange of information and health care services delivery to increase public access to disease diagnosis, treatment, and prevention, and for the continuing education of health care providers and others in the interests of improving individuals’ health and their communities. 1,2 Telemedicine can overcome area and temporal limitations and provide medical services for distant regions not currently covered by health care resources. 3,4 Currently, 42.65% of China's population lives in rural areas. Compared with developed countries, the development gap between urban and rural areas in China is vast, and regional development is extremely unbalanced (National Statistics Yearbook of China 2017 * ). For example, 80% of China's current health care resources are concentrated in cities; two-thirds of these are concentrated in megacities. 5,6 Thus, telemedicine has become a strategic measure in China that can alleviate the problem of geographically unequal allocation of medical resources, increase the disease diagnosis and treatment capability at a grassroots level, and equalize urban and rural health care services. 5,7,8
In recent years, telemedicine has undergone rapid development in China. According to the National Health and Family Commission report, in 2013, 2,057 medical institutions provided telemedicine services in China. 9 In 2017, 22 provinces established provincial telemedicine platforms, covering 13,000 medical institutions in more than 1,800 counties and conducting ∼60 million teleconsultation cases. 10 However, to date, there is no unified national operating pattern for China's telemedicine services, as the platforms in different provinces and cities are discretely constructed, resulting in mutually independent and chaotic architectural designs. The lack of a provincial or national uniform operation and management platform obstructs the interconnection between different telemedicine systems. 11 Thus, telemedicine systems have become new “data islands,” similar to those of other medical information systems, which are violations of the open, sharing, and interactive attributes of telemedicine. 1,5,12
The major issues in the construction and operation of telemedicine in China include the following. First, relevant regions, hospitals, or companies inconsistently interpret and practice national standards, leading to the constructions of disparate system architecture and data transmission standards. 4,13 This obstructs the effective integration of heterogeneous medical information, as well as data intercommunication, which leads to “data islands.” Second, there are differences in the communication standards and audio–video transmission protocols followed by diverse video-system terminal products, 14,15 leading to videoconferencing with various incompatible networks and terminal types, which limits the intercommunication of video terminals and the popularization of telemedicine services. Third, existing telemedicine systems are overly dependent on the single videoconferencing architecture, and patients’ medical information is mostly transmitted in the form of “auxiliary streams” (computer screen streams), which cannot self-adapt to complex network environments. 16,17 Hence, the synchronous exchange and transmission of medical data and audio–video information are easily affected by network quality, which influences the implementation effectiveness, service quality, and telemedicine application scope.
The Henan Province Telemedicine Center of China (HTCC) is the first provincial telemedicine service organization to be established in China. Over the course of its 20-year development, its coverage and system functions have gradually been expanded and improved. Currently, the HTCC is the National Telemedicine Center of China. This study aims to establish a telemedicine system based on the HTCC's practices that is jointly driven by videoconferencing and data exchange and can support various telemedicine services. Through unified standards, normative procedures, and effective sharing and interconnection mechanisms, the cross-regional telemedicine systems inside and outside Henan province are interconnected to develop an operation mode of “one platform, one network, and one set of data center systems” for the HTCC. 14,18 The new telemedicine system can overcome the problems of interregional data barriers and hardware/software incompatibility. Through the development and implementation of the telemedicine system, this study can provide a real-life example for China, and even regions worldwide, to construct a standardized system for cross-regional telemedicine, overcome “data island” issues, connect multisource medical information, and ultimately achieve platform-based and regionalized telemedicine operations.
Methods
Requirements Analysis
To solve the problems in China and improve telemedicine implementation and service quality, this study, based on user-oriented (e.g., doctors, patients, and managers) questionnaire surveys, focus group discussions, and expert consultation, summarized the following functional and application demands that a new telemedicine system should meet. 2,19,20
Device access
The system should support access to diverse videoconferencing software and hardware terminals and should convert the data formats produced from distinct protocols and networks. This will enable different types of terminal devices to interact with each other across various network modes. 19
Transmission linkage
It is necessary to ensure compatibility with virtual private networks (VPNs), the internet, cellular networks, and satellite, as well as the ability to self-adapt to different network modes. The system should be able to transmit medical data safely and reliably even under poor network quality conditions.
System connection
The system should achieve seamless connection with various information systems in hospitals and establish a comprehensive service system for data acquisition and integration. In the same system interface, authorized consultation experts/physicians/managers can examine patients’ medical records, instructions, tests, and imaging information per their own requirements.
Data interaction
At the “acquisition-transmission-storage-display” stages, the system should meet the application requirements of diverse telemedicine services for audio–video data and medical information. The system should support the demands of health care services for diverse information from testing, examination, surgery, and hospitalization.
Standards and specifications
Compliance with national industry standards, a set of telemedicine system standards and clinical service specifications should be established or improved. These standards could be used to clarify system functions, service scope, operation processes, information security, data exchange, information monitoring, and quality control to provide a foundation for large-scale telemedicine application. 20,21
System Design Conception
Considering the issues inherent in telemedicine system construction, this study employed service-oriented architecture (SOA) to conduct top-down gradual refinement and then completed the system's hierarchical layout and architectural design. The specific modules in the telemedicine system mainly include application function, technical systems, data interaction, information security, network systems, and physical deployment. The different modules are interconnected (Fig. 1). 19,22 –24
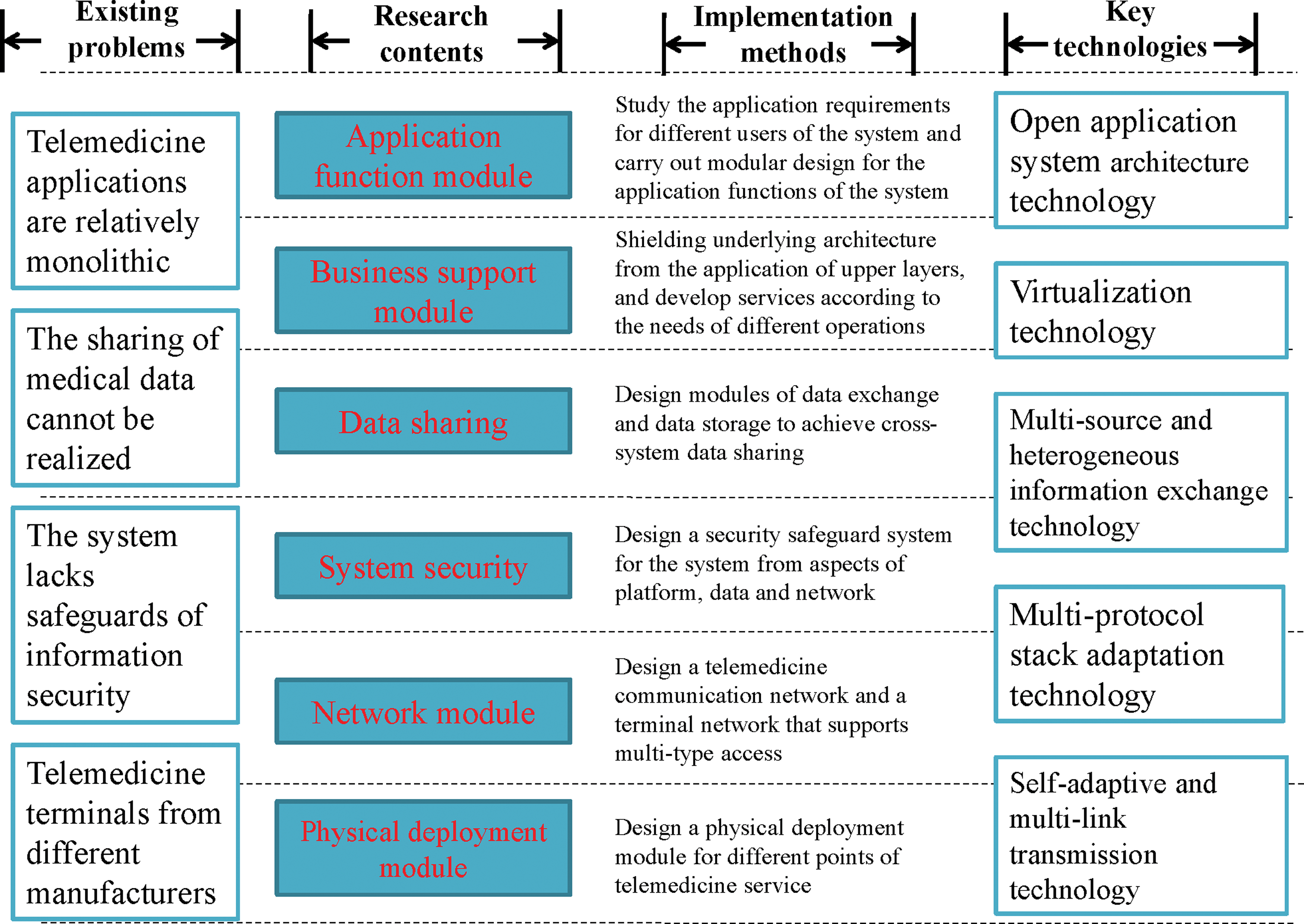
The conception and flow for the design and establishment of the telemedicine system. Color image available online.
Application function module
From the perspectives of telemedicine participants, service needs, procedures, and maintenance supervision, an analysis of existing telemedicine information systems was performed. According to the actual needs of different participants, system function modular design was conducted to support the telemedicine system's application function expansion.
Business support module
With data exchange as the core, the underlying architecture was shielded from upper layer applications to develop services for diverse business needs. To support the normal operation of application functions at different system layers, necessary screening was performed according to the specific services’ feasibility, scalability, and normativity.
Data sharing module
Telemedicine system data mainly include medical information, audio–video data, and basic system data. According to the characteristics of different types of data, standardized conversion and message encapsulation were performed on data acquisition methods, transmission protocols, and storage rules. Then, the medical data sharing and exchange between heterogeneous systems were achieved to support telemedicine services and applications.
Network module
To date, different medical institutions usually have various types of network links with medical data originating from multiple platforms, leading to large transmission volumes and low information security. To address these challenges and achieve the integration of diverse networks, techniques including intranet VPN, internet protocol filtering, address conversion, and protocol constraints were employed to formulate a safe and reliable telemedicine network architecture.
Physical deployment module
According to the functional positioning and actual needs of different levels of telemedicine institutions in provinces, cities, and counties, the performance parameters of business operations were estimated. Then, the requirements of the network environment and the physical device performance of the telemedicine system deployment were evaluated to develop physical deployment frameworks for different types of organizations.
Security module
Information security is key to telemedicine system design. From the perspectives of technology, organization, and management, the various scenarios of telemedicine applications were thoroughly analyzed. Then, the telemedicine system built security safeguards including physical security, network security, audio–video system security, data security, and application security to establish a secure system that can be continuously improved. These considerations and designs ensure the telemedicine system's security.
System Architecture Design
Based on system construction conception, the system architecture design was developed. The front-end processors and other devices were relied upon to complete the collection of medical information and video data. Multiple types of network links were used for data transmission to ensure the security and transmission quality of the data interaction. In addition, basic platforms, including a data exchange platform and a unified video platform, were established. On this basis, open deployment of application subsystems such as teleconsultation, distance education, and remote specialty diagnosis was developed to ultimately construct a telemedicine system jointly driven by videoconferencing and data exchange. 25,26
The system architecture consists of five layers: data source, data access, data exchange, platform, and application layers (Fig. 2). The data source layer is responsible for accessing information related to diverse types of telemedicine services, including various information systems of hospitals, and business data of third-party platforms and video terminals. The data access layer is used to pre-normalize the collected data through the front-end processors and complete data transmission relying on various types of networks in the telemedicine system. The data exchange layer is mainly for the virtualization of the storage and server resources of the system, realizing the storage of data, completing the data exchange based on data middleware, and providing the required data to the superior applications through the middleware. The platform layer provides support for the operations of telemedicine services by establishing a heterogeneous data exchange platform, a unified video platform, a cloud platform of integrated services, and an expert resource library. The application layer is used to carry out various telemedicine services on the basis of the unified videoconferencing platform and data exchange platform support.

Overall framework and structure of the telemedicine system jointly driven by data exchange and videoconferencing. HIS, hospital information system; LIS, laboratory information system; PACS, picture archiving and communication system; VPN, virtual private network. Color image available online.
Key Technologies
Based on the overall architecture design, multiterminal access, network transmission, data sharing, and cloud platform construction were analyzed. Technologies including multiprotocol stack adaptation, self-adaptive multilink network transmission, information exchange of multisource heterogeneous medical systems, and open application system architecture were employed to construct the telemedicine system.
Multiprotocol stack adaptation technology
In view of the poor compatibility between audio–video terminals of different brands, the system adapted audio–video communication protocols that comply with international standards, such as H.323, Session Initiation Protocol (SIP), and Hypertext Transport Protocol (HTTP). Multiprotocol stack adaptation technologies were employed to create a strong protocol conversion capability. This enabled support for the simultaneous access of hardware terminals (with different protocols or multibrands) and software terminals based on distinct operating system (e.g., Windows, iOS, or Android). The technologies achieved interconnection between multibrand devices from diverse manufacturers and met the requirements for large-scale access of various services from hospitals, nursing institutions, and individual health management organizations.
Self-adaptive multilink transmission technology
In China, the current telemedicine system has diverse operation modes and transmission links, and the coding and communication protocols also differ. Therefore, based on the dual-protocol stack and double-encoding protocol, we employed self-adaptive multilink network transmission technology, under the condition of multiple links access, to support stable public–private network traversing and self-adaptation to the audio–video codec. This technology ensures the videoconferencing effectiveness during telemedicine services. For example, under the premise of ensuring an overall 1080P or 720P effect, the system could dynamically adjust the resolution in the split screen for every meeting site according to the size of the venue. This could reduce the repetitive compression of the multipoint control unit (MCU) and the traffic pressure of network devices, which would ensure that the system met the high reliability requirements of clear audio–video conversation and information sharing necessary for telemedicine.
Heterogeneous information exchange technology
To meet the requirements of cross-system data interaction and sharing, the information exchange technology of multisource heterogeneous medical systems based on the enterprise service bus (ESB) and databases was applied in the information access layer. Furthermore, a unified telemedicine system interface was also opened to achieve integration of medical information systems, or information transmission and the sharing of the telemedicine system. During cross-system interaction, a patient primary index system was established to solve the problem of distinct systems being unable to interact due to data inconsistency. The unique patient identifier can realize the interconnection of multiple homogeneous or heterogeneous medical information systems. In addition, the Health Level 7 (HL7) protocol was used for standardized data conversion to achieve barrier-free information transfer and sharing between heterogeneous medical and telemedicine systems.
Open application system architecture technology
To meet the business integration requirements between the telemedicine system and other platforms/systems, as well as the needs of new businesses that may arise in the future, it is essential to ensure the system's openness. SOA techniques were used to customize abundant application programming interfaces (APIs) to support the development of up-to-date data interfaces for new applications. This fosters system flexibility, openness, and reusability and ensures the normal operation of telemedicine services during system maintenance and updating, which lengthens the current system's life span.
Cloud platform virtualization technology
Considering future expansibility, virtualization technology was employed to integrate server resources to achieve high scalability, reliability, and utilization. Through the abstraction of server physical resources, the virtualization platform transformed the central processing unit and internal storage into a set of logical resources that are uniformly managed, flexibly scheduled, and dynamically allocated. Then, on a single physical server, these logical resources were used to build multiple simultaneously operating and mutually independent execution environments for the virtual machine. This can improve the system's utilization of computing, storage, and networking and may enhance the telemedicine services’ reliability.
Data Docking Scheme
The development and operation of telemedicine services are inseparable from medical data support. The system developed a series of interface schemes for data from electronic medical records (EMR), the hospital information system (HIS), laboratory information system (LIS), picture archiving and communication system (PACS), and electrocardiograms (ECG), all of which were used to realize the docking with the connected hospitals’ various business systems (Table 1). Regarding the diverse informatization situation of different hospitals, each interface solution provides two types of interconnection methods: viewing direct connection and web service interface docking. Hospitals can choose suitable interface schemes according to their actual conditions.
The List of Relevant Interface Schemes
ECG, electrocardiograms; EMR, electronic medical records; HIS, hospital information system; HTCC, Henan Province Telemedicine Center of China.
Results
Considering the actual problems in China's telemedicine, the current study designed a telemedicine system jointly driven by videoconferencing and data exchange. Based on the system, the HTCC has developed a five-level “province-city-county-township-village” telemedicine network covering the entire Henan province.
Functional Realization of the Telemedicine System
According to the different telemedicine system users’ functional requirements, the constructed system achieved the following three functions: integration of videoconferencing, data acquisition and exchange of heterogeneous systems, and telemedicine services application and expansion. Videoconferencing integration achieved the cross-terminal integration and interaction of videoconferencing. Data collection and exchange of heterogeneous systems enabled telemedicine information acquisition and transmission among diverse medical institutions. Based on these two core functions, the application and expansion of various telemedicine services were ultimately realized.
Videoconferencing integration
Based on traditional videoconferencing systems, this function enriches API compatibility and supports flexible connections with the internet, cellular networks, and VPNs. The conversion of different communication protocols was achieved through local MCU and integrated servers. This function supports the registration of different videoconferencing hardware and software terminal brands and is compatible with diverse MCU and the conferencing terminals that follow universal standards/protocols. Without changing the operating habits, this function realizes the audio–video conversation of software/hardware video terminals registered in distinct systems. In addition, the function also supports dynamic dual streams, electronic whiteboards, one-click conferencing, predefined conferences, autonomous meeting entries, conference push notifications, multiple displays, automatic matching code streams, conference status monitoring, and remote maintenance.
Acquisition and exchange of heterogeneous system data
Data acquisition and the exchange of multisource heterogeneous systems are core functions of this telemedicine system. Based on the HL7 protocol, the system establishes the medical industry standard data set in the master data management system and provides ESB services and data extract transformation load (ETL). This enables the system to support the adaptive access to heterogeneous databases and files, as well as service access methods such as Simple Object Access Protocol, JavaScript Object Notation, File Transfer Protocol (FTP), HTTP, and HTTP over Secure Socket Layer. The system supports the combination of multisource data, data routing, data row and column transposition, dictionary queries, loop dispatching, load balancing, and data processing of parallel computing. Additionally, the system supports the access to the routing address list, protocol conversion, message format conversion, node security certification, asynchronous transmission of mass data, and breakpoint resume.
Support and expansion of telemedicine services
The system provides technical support for protocols, transmission, data management, data processing, services, containers, and APIs. Additionally, the system supports various types of operating systems (e.g., Unix, Linux, and Windows) and the smooth migration between different platforms. The system provides message-oriented middleware, universal file transfer GPRS tunneling protocol, service management protocol, and data integration ETL, which can adapt to various types of heterogeneous database platforms and operating systems. Meanwhile, the system also supports WS-Security 1.1 specifications and protocols for the secure sockets layer, and it provides data encryption and decryption, identity certification, and digital signature.
Supported by the abovementioned component system architecture and features, to date, the system has conducted various telemedicine services, including teleconsultation, remote specialty diagnosis (e.g., telepathology, telediagnosis of medical images, and tele-ECG), remote surgery teaching, and distance education. Based on the system, clinical services including online consultation, hospital appointment and registration, daily rounds, multidisciplinary consultation, bidirectional referral, intensive care unit care, online clinical pharmacy services, mobile payments, patient follow-ups, and health assessment and management are also conducted. The telemedicine services involve the clinical departments of internal medicine, surgery, obstetrics and gynecology, pediatrics, and relevant medical technology departments (Table 2).
The Clinical Department's Distribution of Comprehensive Teleconsultation, in 2017, from County-Level Centers of the Henan Province Telemedicine Center of China
Business Process of the Telemedicine System
Based on the telemedicine system, the “province-city-county-township-village” five-level telemedicine VPN was used to centralize expert resources from the connected hospitals and to establish the HTCC expert library, through which the HTCC provides telemedicine services for the connected grassroots medical institutions. To support the implementation of telemedicine services, the HTCC has devised specific functional departments, adapted a personal responsibility system, clarified management regimens, and standardized the service procedure. A call center has been established to manage the telemedicine system's large-scale operations and services, according to the “call-response-scheduling-implementation-assessment” procedure. The ESB provides a basic connectivity hub to support data exchange between the front-end servers of each grassroots subcenter and the HTCC's system server.
Effects of the Telemedicine System's Application
System characteristics
The system is an integration of videoconferencing, heterogeneous medical information, and telemedicine services, and it achieves flexible access to multiple terminals, networks, and systems. Our system allows consultation experts to communicate with remote patients and doctors through audio–videoconferencing, and it provides real-time access to the patients’ medical records stored in the data center. This can support precise patient diagnosis and treatment plan development. The system's major characteristics are summarized as follows.
Universal standard protocols
The system adapts to protocols such as H.323, SIP, HL7, HTTP, and FTP, and it supports video coding protocols based on H.264 and H.265 scalable video coding/advanced video coding. Through standardized protocols, the system enables the interaction of medical data and high-definition audio–video information among experts from diverse medical institutions.
Flexible network access approaches
The system is equipped with amenable network adaptability, and it supports access modes such as satellite, Wi-Fi, cellular networks, and VPN dedicated networks, as well as the transfer of information between public and private networks. This enables participants from various businesses to access the platform through diverse networks.
Integration of heterogeneous information systems
In accordance with international and Chinese national medical information standards, the telemedicine system provides international standard APIs. Through the open and unified APIs, domestic and foreign devices in compliance with international protocols can both be integrated into the system. The telemedicine system integrates most of the medical information systems in hospitals, including HIS, PACS, radiology information system, EMR, and LIS. According to the unique primary index (patients’ ID), the system extracts necessary data from the applicant hospitals’ information systems. Related medical records are retrieved from online-connected hospitals to reconstruct relatively complete information for a specific patient, through which the system enables the acquisition and integration of data from heterogeneous information systems.
System performance
Since the telemedicine system went online 4 years ago, there has not been a large-scale network interruption, and there has been no experiencing of server downtime in terms of conferencing, data transmission, or information recording. Amenable and satisfactory system performance is a key guarantee for the smooth operation of telemedicine services. The system's performance indicators are mainly manifested as follows.
High security
The system is based on China's information security level 5. Through approaches including authority certification, audio–video encryption, medical data encryption, redundancy, disaster recovery, firewalls, and traffic cleaning, the system can ensure the security of telemedicine information at the “acquisition-transmission-storage-application” stages.
High reliability
The system adapts mechanisms including intelligent network monitoring, dual-link intelligent switching, system host hot standby, and dual-active data centers to ensure reliable data transmission and storage. Even in the case of a 30% network packet loss, the normal transmission of 720P 30Hz audio–video data and medical information can still be achieved, which guarantees the telemedicine services’ quality.
High portability
The rich and open system APIs support the access of PC, page version web, Android/iOS mobile app, and third-party applications, ensuring that the system has acceptable scalability. To date, an average of five new applications are launched annually in the system, which increasingly enriches the application functions.
Convenient maintenance
The system enables automatic version detection and one-click updating. It supports the functions of e-mail, short message, and app push notifications, as well as the visualization of network topology, online devices status, network status, system and operation logs, and alarm information. This greatly improves routine maintenance and system administrators’ management efficiency, and it ensures uninterrupted 24/7 system operations. In recent years, the system has successively added more than 24 applications subsystems online. Good telemedicine system management and maintenance with a wider scope, more functions, and more devices is achieved, without an increase in labor.
Coverage and amount of telemedicine services
In 2011, the HTCC's audio–video network was deployed in various cities and counties under Henan province's jurisdiction. In 2014, full coverage of all cities and counties in the entire province was completed. At this time, the network also started to radiate toward surrounding provinces (Shanxi, Shandong, and Hubei) and remote regions (e.g., Sichuan, Hunan, Xinjiang, and Fujian province). Currently, the HTCC has covered 19 municipal level centers, 176 county centers, 230 grassroots workstations (townships), and 85 grassroots service points (villages/communities), forming a five-level “province-city-county-township-village/community” telemedicine network linkage within the province.
As the HTCC achieved coverage of all province cities and counties in 2014 and the number of connected medical institutions increased, the number of teleconsultations also showed a stable increase. In December 2014, the telemedicine system jointly driven by videoconferencing and data exchange was officially implemented online, resulting in a significant increase in teleconsultation cases in 2015. The regular business volume of nearly 30,000 comprehensive teleconsultation cases subsequently became stable.
Economic benefits
County-level hospitals connected to the HTCC can retain local patients for treatment through teleconsultation and remote specialty diagnosis, thereby reducing patients’ medical costs and food, accommodation, and travel expenditures. In 2017, compared with transferring to a superior hospital for treatment, each patient treated at a local county-level hospital in China was able to save about ¥7,680 Chinese Yuan (approximately US $1,100) (Table 3). Concretely, the county-level hospitals linked to the HTCC conducted 20,752 comprehensive teleconsultations in 2017 (Table 2). Among these, 15,964 patients remained at local hospitals for treatment, saving them about ¥120 million Chinese Yuan (approximately US $17.5 million) in hospitalization costs and food- and travel-related expenses.
Cost Savings for Each Patient Applied for Teleconsultation in the Henan Province Telemedicine Center of China and Were Treated at Local Hospitals a
Costs listed are in Chinese Yuan.
The average level of patient costs at national grade 2 and above public hospitals from January to October 2017 was used as a reference for hospitalization costs.
For per patient, one accompanying person was assumed. Then, the total patients’ costs of food, accommodation, and transportation were calculated, which were estimates of the local corresponding average expenses. The average length of hospitalization was referenced from the 2017 China Statistical Yearbook, which was 9.4 days.
Discussion
Based on the existing problems with telemedicine and the requirements analysis of China's current situations, this study proposed the conception, design, and implementation of a telemedicine system jointly driven by data exchange and videoconferencing. Taking the HTCC as an example, the effectiveness of the development and implementation of the telemedicine system was investigated. Our results have been promoted as national construction guidelines and industry standards for demonstrating and popularizing telemedicine nationwide. To the best of our knowledge, this is the first study based on the integration of videoconferencing and data exchange to develop and practically operate a telemedicine system at the provincial level. These findings provide a reference for further promotion and application of the telemedicine system in China, and even other regions worldwide, thereby further improving telemedicine's implementation effects and service quality.
Against the backdrop of China's “internet and health care” development strategy, telemedicine is playing an increasingly helpful role in promoting health care levels in remote and poor regions, satisfying the needs of underserved areas for superior medical resources, and ultimately improving health care quality and efficiency in areas that have not been effectively covered by medical services. 1,10,12 Since 2010, the Chinese government has allocated nearly ¥100 million Chinese Yuan (approximately US $14.5 million) on four occasions to support grassroots telemedicine's development, implementation, and popularization. This was seen in 22 central and western provinces, where 12 subordinate hospitals directly under the National Health and Family Planning Commission and 12 western provinces were organized together to establish a teleconsultation network that included 12 ministry affiliated hospitals, 98 tertiary hospitals, 3 secondary hospitals, and 726 county-level hospitals. 7,9,10 Telemedicine has become an imperative strategy for promoting and implementing “Healthy China Planning.” It is also critical for driving the construction of hierarchical medical systems in China; in other words, the “initial diagnosis at grassroots, bidirectional referral, acute and chronic treatment classification, and upper and lower medical institution linkages.” 10,27 This is crucial for alleviating the unequal distribution of health care resources, reducing medical costs, and ensuring that everyone enjoys equal rights and opportunities for obtaining medical services.
The HTCC has undergone long-term construction of a technical platform and practical operation. Currently, it has established the first five-level “province-city-county-township-village” telemedicine network covering the entire province. It also provides China with an open and sharing comprehensive telemedicine service platform, including 35 tertiary hospitals and more than 200 secondary hospitals in Henan province. 18 In addition, the HTCC's teaching and coordination network and teleconsultation subcenters are connected to more than 1,000 primary hospitals in Henan, Xinjiang, Shanxi, Sichuan, Shandong, and Guizhou provinces, enabling the vertical circulation of medical resources toward remote areas. 28,29 The HTCC has developed into a national telemedicine demonstration base and regional collaborative medical service center—with the largest scale, most advanced technology, widest coverage, and soundest functions in China. In January 2018, it was established as China's National Telemedicine Center. Annually, the HTCC network performs nearly 30,000 comprehensive teleconsultations, more than 1 million remote specialty diagnoses, and more than 300 instances of distance education (through which nearly 300,000 medical staff have been trained). 14,18,29 Thus, the telemedicine system demonstrates considerable implementation effects and achieves appreciable social and economic benefits. The practical operation of the HTCC provides a solid platform, and software/hardware support, for the design and application of the telemedicine system discussed in this study.
The telemedicine system proposed by the current study can process multiple protocol stacks and integrate traditional audio, video, and web conferencing. Software-defined and virtually extensible local area network technology is employed to achieve network virtualization, and the connection of terminals with international protocols (e.g., SIP and H.323) is supported. 21,30 –32 The system is also compatible with the access of video hardware and cloud MCU, and the system's applications integration is completed based on technologies like web service, ESB, and SOA. 19,33 –35 These designs effectively address the issue of network and device incompatibility in terms of telemedicine videoconferencing. The system adapts distributed, virtualized, modularized, and componentized system architecture for flexible deployment and service expansion, which can achieve information interaction in multisource heterogeneous medical information systems’ data collection, transmission, storage, and visualization processes. 14,19,26,29,36,37 Thus, the system can effectively connect and integrate the “data islands” between diverse medical institutions and telemedicine systems.
The system can conduct the synergistic fusion of video systems and medical information systems. It can also integrate big data analysis techniques such as machine learning and convolutional neural networks—based on the Hadoop platform—to support physicians’ clinical diagnoses and medication decisions. 16,28,37 In addition, the system opens and shares various APIs to support the development and access of mobile terminal systems (e.g., iPad, Android, and iOS) and third-party applications (e.g., WeChat and Sina Weibo) that meet the needs of physicians and patients for medically related consultation services. 14,18,29,37
Several challenges with the current system must be acknowledged. First, the present telemedicine system only supports audio–video devices that comply with international standard protocols. Although some nonstandard devices can also be accessed by the system in a back-to-back way, new equipment needs to be purchased to support the operations, which increases construction costs. Second, the system realizes the interconnection and sharing of medical information by establishing a series of unified standard interfaces. However, related system interface transformation costs are relatively high, and the cycles are usually long. This limits the telemedicine system's large-scale rapid growth. Third, the medical information security protection mechanism has not been completely established for the current telemedicine system. Telemedicine services’ scope and content, charging standards, and responsibility allocation mechanisms are not yet mature. Finally, the development of emerging technologies such as big data analysis and application, cloud computing, and artificial intelligence also poses new challenges to the architecture, service models, and data security of the existing telemedicine system.
Conclusions
The present study first performed an analysis of the current development status of telemedicine and the related challenges encountered in China. Then, we proposed a countermeasure for the existing issues—the construction framework of the telemedicine system jointly driven by data exchange and videoconferencing. Finally, the practical development and operation of the HTCC were used to investigate the performance effects of the system. The results indicate that the telemedicine system can effectively solve problems such as “data islands,” the incompatibility of networks and terminals, and poor telemedicine information transmission quality to achieve satisfactory implementation results with appreciable social and economic benefits.
According to our knowledge, this is the first study to integrate data exchange and videoconferencing to jointly drive telemedicine services. The telemedicine system can effectively integrate the “data islands” among multisource heterogeneous medical information systems. It is compatible with complex networks and various terminals, and it can also self-adapt to diverse network environments and patterns. The system achieves synchronous exchange and transmission of medical data and audio–video information, which can effectively improve telemedicine's implementation effects, service quality, and application scope. The design and implementation of the telemedicine system and the HTCC's practical operations have value for promoting the circulation and coverage of superior medical resources in rural villages, mountainous areas, and other remote less-developed regions. Additionally, they can help alleviate the unequal distribution of medical resources, accelerate the up-down linkages of medical resources and information sharing, reduce medical expenditures, and promote the construction and development of a new pattern for the hierarchical medical system in China.
Footnotes
Acknowledgments
National Natural Science Foundation of China (Grant No. 71673254); special funds from central government for the guidance of local science and technology development National Key R&D Program of China (Grant No. 2017YFC0909901); special funds of major science and technology project in Henan province (2016) (Grant No. 151100310800); the Science and Technology Program for Public Well-Being of Henan province (Grant No. 172207310001) and Humanities and Social Science Project of the Ministry of Education (Grant No. 16YJAZH074). The funders played no role in the design, development, or interpretation of the present work. The views expressed in the article are those of the authors and do not necessarily reflect the position of the funding bodies.
Authors’ Contributions
J.Z., Y.K.Z., and J.H.G. conceptualized, designed and initiated the study. Y.K.Z., J.H.G., B.Z.C., J.M.S., L.L.W., and X.Y.H. drafted the initial article. D.X.S., H.T.C., H.L.H., and X.Q.S. involved in the development of methodology and discussion of article structure. J.Z., Y.K.Z., J.H.G., and B.Z.C. reviewed and revised the article. All authors read and approved the final article as submitted.
Disclosure Statement
The authors declare that they have no actual or potential competing financial interests.