
Abstract
Background:
Telemedicine as a technology is expected to resolve issues such as doctor shortages and disparities in medical services. However, high costs of system installation and maintenance inhibit its widespread use.
Introduction:
This study involved a cost minimization analysis for installation of a teleradiology system in the Hokkaido prefecture of Japan. Conditions under which system utilization is cost-efficient and system utilization is effective for cost reduction were analyzed.
Materials and Methods:
A cost minimization analysis was conducted using three geospatial points of 50, 100, and 200 km from Sapporo city, the prefectural capital of Hokkaido, assuming a central imaging diagnosis center in Sapporo. The analysis was conducted from the standpoint of both patients and requesting hospitals.
Results:
From the patient's standpoint, a cost reduction effect was observed at all three distances from system installation. In contrast, from the hospital's standpoint, a cost reduction effect was found only when teleradiology examination was conducted from a distance of at least 100 km from Sapporo.
Discussion:
Results show that the cost reduction effect for patients increased as the travel distance increased. Although the teleradiology service is beneficial for a wide range of patients, the financial burden on requesting hospitals is significant.
Conclusions:
The following conditions were found necessary to reduce the requesting hospital's financial burden: the hospital should be far from the imaging diagnosis center, an inexpensive system is to be selected, and the system needs to be utilized continuously.
Introduction
Japan is currently experiencing a significant decline in birth rate combined with an increasingly aging population, and this trend is more rapid than in other advanced nations. 1 This has led to a huge increase in national medical expenses. Therefore, there is a need to look for ways to provide financially efficient medical services consistent with current medical standards. Moreover, the number of doctors per capita in Japan is below the average of nations in the Organization for Economic Cooperation and Development and it is the sixth lowest among the 36 members despite the increasing demand for medical services due to population aging. 2 In addition, doctors tend to choose metropolitan areas as their places of employment and avoid rural areas. Therefore, it is not easy to resolve the shortage of doctors in rural areas.
Telemedicine technology is anticipated to resolve these soaring medical expenses and the issue of shortage and uneven distribution of doctors. Costs of telemedicine systems have dropped over the years and many low-cost options are readily available now in the world. Telemedicine has recently also been utilized in the regional medical revitalization plan in Japan, and several telemedicine research outcomes have been reported. 3 –6 Telemedicine benefits patients by reducing the burden on their time and body, and patients have reported increased satisfaction. In addition, there are benefits to doctors as well, such as less time spent traveling and being able to receive consultations from specialists while examining a patient.
Positive evaluations of the effectiveness of telemedicine have been found in reviews of cost–benefit and cost-effectiveness analyses for several diseases and general health care: diabetes, depression, heart failure, radiology, ICU, and general health. 7 –19 Daucourt performed a cost minimization analysis and reported that introducing teleradiology can help avoid transfers in an emergency and that the initial equipment cost would have an impact on results. 16 Matsumoto (2015) maintained that teleradiology is the only viable way to fill the distribution gap between radiologists in rural and urban areas. 20
However, telemedicine in Japan has not yet expanded, with only 742 hospitals (10.0%) providing the service and 185 hospitals (16.0%) using it. In addition, telepathology is provided by only 63 hospitals (0.8%), while tele-home-care service is provided by 17 hospitals (0.2%). 21 The reasons for this include (1) financial factors related to communication and labor costs; (2) human factors, including the transportation of system operators or medical practitioners who have a strong understanding of telemedicine; (3) legal factors, including the Personal Information Protection Law and the Pharmaceutical and Medical Device Act; (4) technical factors, including computer virus infections and machine problems; and (5) other factors related to the operational environment. In particular, financial factors are the biggest obstacle to increasing the popularity of telemedicine in Japan.
In recent years, information and communication technology and medical information devices have improved, while at the same time, equipment costs and service fees for installing and maintaining telemedicine systems have declined. However, using a telemedicine system continuously requires ongoing costs (i.e., monthly communication circuit usage fees) in addition to the initial investment (i.e., hardware and software). Because most of the costs associated with telemedicine cannot be recouped by diagnosis fees, such costs are borne by medical institutions. Therefore, there has been no increase in the number of medical institutions that have installed telemedicine systems.
Although past telemedicine studies place importance on technology development, there are few studies from a clinical sociological perspective. To expand telemedicine services in Japan, it is necessary to clarify their economic efficiency and cost-effectiveness and discuss their effectiveness and challenges, such as patients' and medical staff's burdens, system installation and operation costs, and network communication costs.
Cost minimization analysis is widely used as an evaluation method in medical economics when the outcome of a clinical technology is considered equivalent to that of an alternative solution. 16,17,19,22 –29 Unlike cost-effectiveness analysis, cost–utility analysis, and cost–benefit analysis, cost minimization analysis calculates only cost without considering the effect.
Teleradiology is a major telemedicine service already in common use in many countries. In this study, a cost minimization analysis was conducted to clarify the conditions under which teleradiology, a type of telemedicine, can be expected to become widespread in Japan. We examined the costs of both patients and requesting hospitals when telemedicine services are used.
Materials and Methods
Based on the assumption that the clinical quality of radiology image diagnosis would be the same, the following two conditions were compared: (1) the cost when the teleradiology examination is conducted and (2) the cost when in-hospital examination is conducted. A cost minimization analysis was conducted for a computed tomography (CT) scan examination using the following hypothetical scenario. The analysis was conducted from the standpoint of patients and requesting hospitals in cases where the patient's residence and the requesting hospitals were located 50, 100, and 200 km away from Sapporo city, the prefectural capital of Hokkaido.
Presumed Scenarios
Expenses incurred by patients
When teleradiology examination was conducted
Expenses that would be incurred by a hypothetical patient residing in a rural location were calculated when teleradiology examination was conducted. The examination images were transferred online to the system of the remote imaging diagnostic center located in the metropolitan area. Radiologists in the center then immediately interpreted the images and prepared a report. The patient's cost included only the examination expenses for one CT scan.
When in-hospital examination was conducted
Expenses that would be incurred by a hypothetical patient residing in a rural location were calculated for a radiographic examination in a hospital in the metropolitan area. Radiologists in the hospital then immediately interpreted the images and prepared a report. The patient's cost included examination expenses for one CT scan and travel costs.
Expenses incurred by hospitals
When teleradiology examination was conducted
Expenses incurred by a requesting hospital in a rural location that conducted the CT scan examination and transferred images to the remote imaging diagnostic center in a metropolitan area were calculated. Radiologists in the center interpreted the images and prepared a report. The number of examinations per month was presumed to be 30. The requesting hospital's costs were the initial installation and subsequent maintenance costs of the system. As the simplest configuration, the system could function to store image data and communicate between the hospital and the center.
When in-hospital examination was conducted
Expenses incurred by a requesting hospital in a rural location that conducted the CT scan examination were calculated. Radiologists who resided in a metropolitan area traveled to the hospital four times a month, interpreted images, and prepared a report. The number of examinations per month was presumed to be 30. The requesting hospital's cost included the doctor's round-trip travel costs.
Expense Data
The expenses for transportation fees, examination fees, and system installation and maintenance fees are shown in Table 1. The requesting hospital was assumed to be located in the rural regions of Hokkaido, and the imaging diagnosis center and radiologists were located in Sapporo. The imaging diagnosis center specialized in radiological diagnosis and was not an insurance medical institution (a medical institution authorized to treat patients with health insurance coverage). The requesting hospitals and patients' residences were located 50 km (Yoichi town), 100 km (Kucchan town), and 200 km (Oshamanbe town) away from Sapporo. The patient transportation fee was calculated as the railway round-trip fare. If the traveling distance was over 100 km, it was presumed that patients would use the limited express train.
Parameters for Simulation Analysis
CT, computed tomography.
The examination fee was calculated using the 2018 Medical Fee Points Table (Ministry of Health, Labour and Welfare, Japan). The diagnostic imaging examination was limited to a simple CT scan (multislice scanner model with at least 16, but less than 64, slice detector capacity). CT equipment was already installed. When requesting hospitals use a teleradiology service, they cannot include diagnostic imaging management levies 1 and 2 in the medical service fee. Furthermore, when requesting hospitals use an imaging diagnosis center that is not certified as an authorized insurance medical institution, they cannot include diagnostic imaging management levies by remote diagnostic imaging in the medical service fee. This is different from regular hospitals because most regular hospitals can include imaging diagnosis management levy 1 or 2 in the medical service fee. The patient's expenses were calculated by setting 10 yen equal to 1 point, with this amount multiplied by 0.3 as the patient's burden based on the national health insurance system.
System installation and maintenance costs were calculated by referring to fees published on the homepage of company A. The initial system installation cost was presumed to be paid in installments over 1 year. The hospital's monthly costs of teleradiology examinations were assumed to include this partial payment plus the monthly system maintenance cost. The amount paid to the radiologist was assumed to be the same in all conditions; therefore, it is excluded from the calculations. Since the internet line was already installed, the network cost between a hospital and the remote imaging diagnostic center was not included. In addition, the connection cost between Radiology Information System / Picture Archiving and Communication System and the teleradiology system was not included because it was assumed that image data were handed over by portable media.
Cost Minimization Analysis
Based on hypothetical scenarios, we calculated costs paid by patients for an examination and costs paid by the hospital each month using the following equations.
The patient's expenses
Teleradiology examination: (medical treatment fee a + b + c) × 10 × 0.3.
In-hospital examination: (medical treatment fee a + b + c + d) × 10 × 0.3 + transportation fee ([a]. CT scan, [b]. CT diagnosis, [c]. electric image management levies, and [d]. imaging diagnosis management levy 2).
The hospital's expenses
Teleradiology examination: (system installation fee ÷ usage period [months]) + system maintenance fee.
In-hospital examination: transportation fee × 4 (times/month).
Simulation Analysis
We simulated conditions where requesting hospitals providing the service could anticipate installation of the system to be cost-effective. The system installation cost, system usage duration, and number of examinations per month were set as shown in Table 2. The relationship between the expenses that the hospitals paid and the following three items was explored. In each relationship, an analysis was conducted using a simulation where the teleradiology examination was conducted at points that were 50, 100, and 200 km away from Sapporo and in the case of in-hospital examination.
Parameters for Sensitivity Analysis
The relationship between system installation cost and monthly expenses paid by hospitals
The system installation cost was increased or decreased by 50,000 yen based on 100,000 yen for sensitivity analysis. The hospital's costs for system installation and maintenance per month were analyzed using a fixed duration for system usage.
The relationship between system usage duration and hospital's monthly costs
The system usage duration was increased from one year up to 5 years in increments of 2 years. Holding the system installation cost constant, the amount that hospitals paid for system installation and maintenance per month was analyzed.
The relationship between the number of examinations per month and the cost for one examination
The number of examinations per month was increased from 30 cases to 100 and up to 300 cases. The amount that hospitals paid for system installation and maintenance per month was analyzed holding the system installation cost and system usage duration constant.
Results
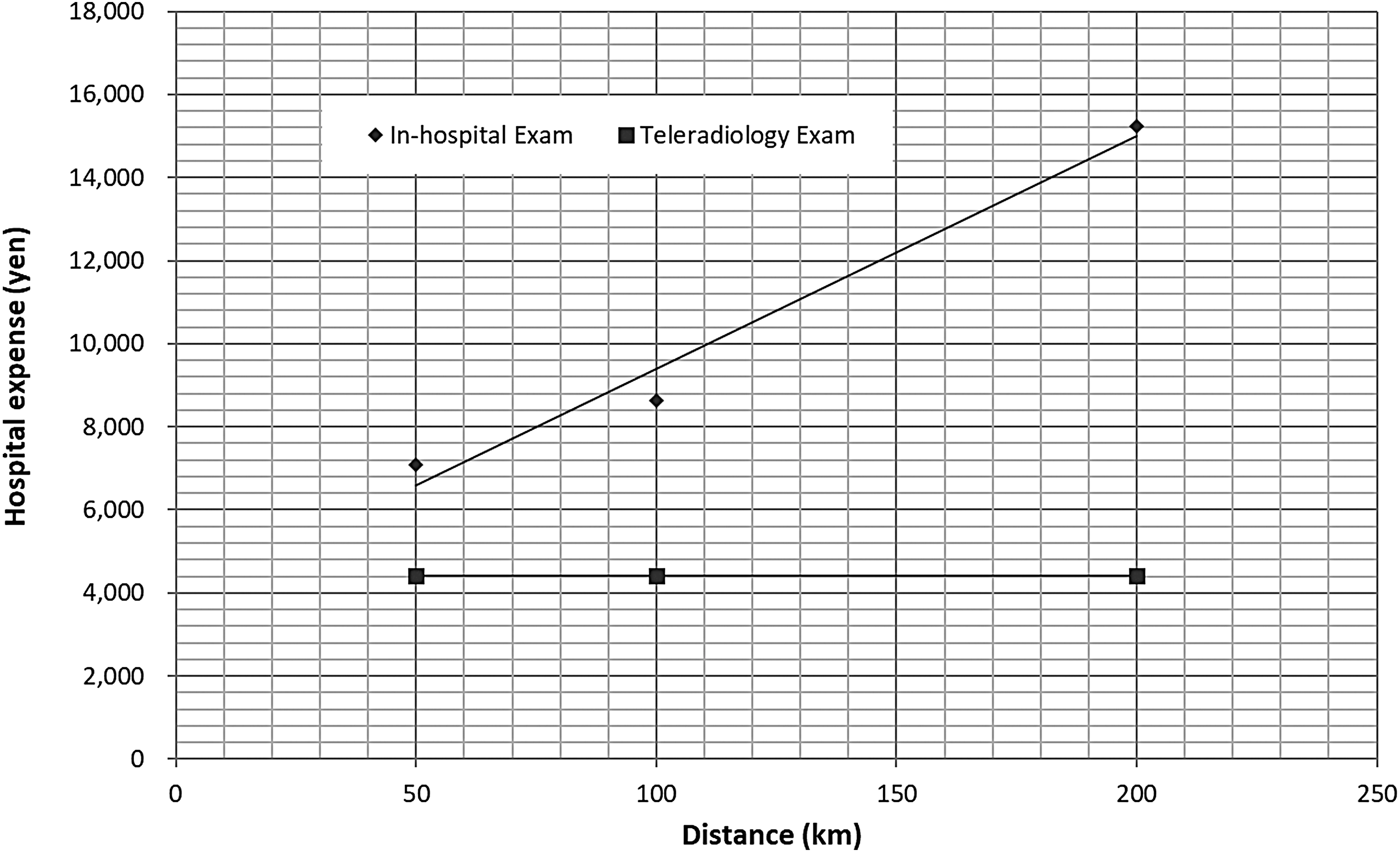
Patients' expenses for teleradiology examination and in-hospital examination are depicted in Table 3 and Figure 1. Patient expenses if in-hospital examination was conducted in relation to the distance from the hospital in Sapporo were 7,090 yen (50 km), 8,630 yen (100 km), and 15,240 yen (200 km). On the other hand, patient expenses if teleradiology examination was conducted were fixed at 4,410 yen. As such, the amount that patients would pay was lower for all distances if teleradiology examination was conducted.
Patient's cost (in yen) per examination using cost minimization analysis. KM, kilometers.
Patient Cost Per Examination Using Cost Minimization Analysis
KM, kilometers.
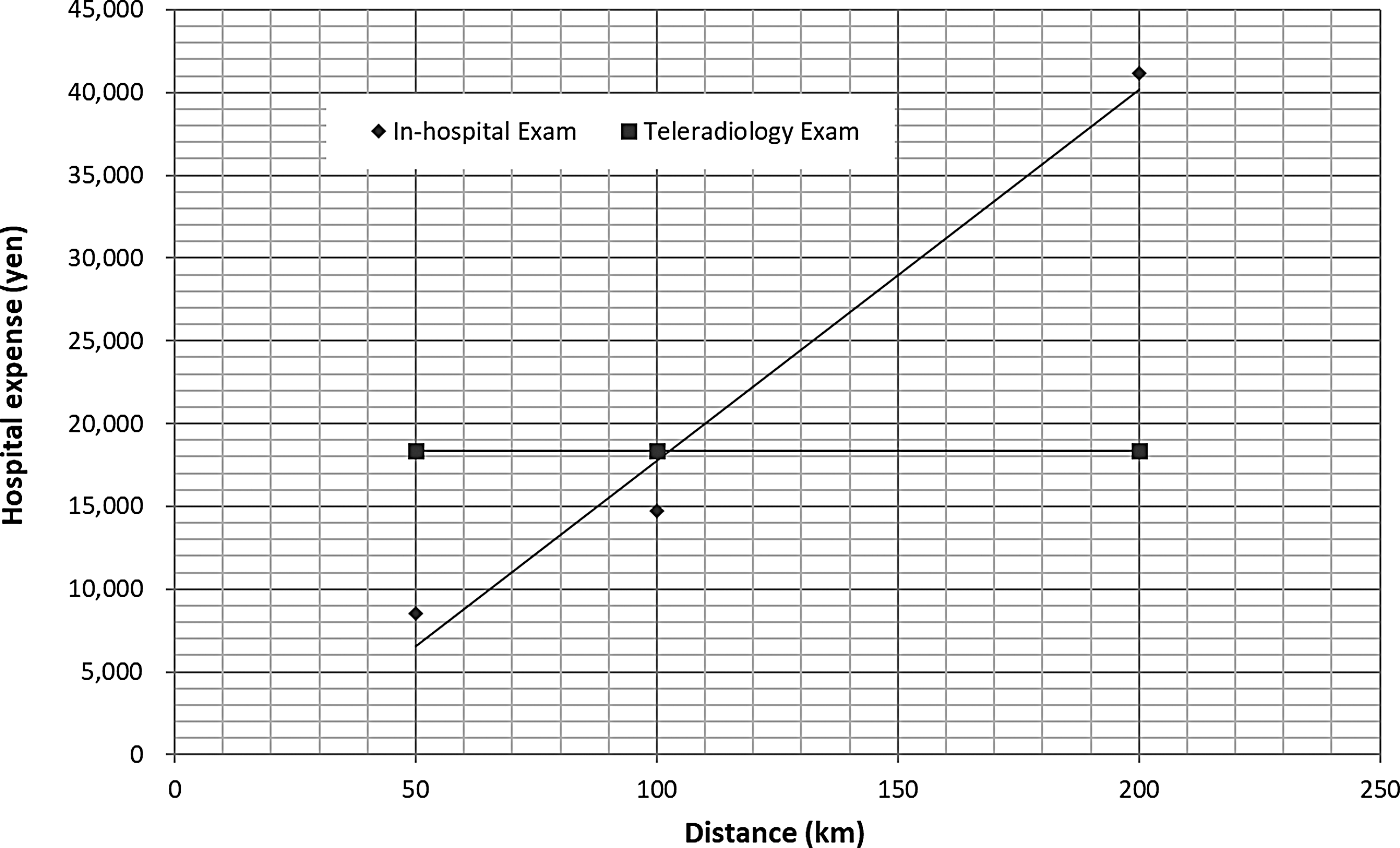
Next, the expenses that hospitals would incur are displayed in Table 4 and Figure 2. The expenses that hospitals would incur if the in-hospital examination was conducted in relation to the distance from the hospital in Sapporo were 8,560 yen (50 km), 14,720 yen (100 km), and 41,160 yen (200 km). On the other hand, the expenses that hospitals would pay if teleradiology examination was conducted were fixed at 18,333 yen. Therefore, only if the distance between the hospital and Sapporo was 100 km or greater would the expenses incurred by hospitals be lower if teleradiology examination was conducted.
Simulation analysis of hospital expenses (in yen) per month. KM, kilometers.
Hospital Expenses Per Month Using Cost Minimization Analysis
KM, kilometers.
The relationships between system installation cost and examination cost, between system usage duration and examination cost, and between the number of examinations per month and examination cost are displayed in Figures 3 –5 .

Sensitivity analysis of system installation cost and examination cost (in yen). KM, kilometers.

Sensitivity analysis of system usage duration and examination cost (in yen). KM, kilometers.

Sensitivity analysis of number of examinations per month and examination cost (in yen). KM, kilometers.
Discussion
Results revealed that the cost paid by a patient for the examination was lower when teleradiology examination was conducted, regardless of the distance. By installing the system, it was possible to reduce the patient's expenses by 2,680 yen (37.8%) at the 50-km, 4,200 yen (48.9%) at the 100-km, and 10,830 yen (71.1%) at the 200-km distance from Sapporo compared with when the system was not installed. This revealed that the cost reduction effect of system installation increased as the patient's travel distance increased. In addition, because patients who travel long distances need to miss work, the patients' burden may actually be larger than the travel expense. Therefore, the cost reduction effect of system installation is dependent on the distance factor.
On the other hand, to outweigh the cost of system installation, hospitals using a system need to be at least 100 km away from Sapporo. These results indicate that although teleradiology service is beneficial to a wide range of patients, the financial burden is significant for requesting hospitals.
Simulation results for the costs of system installation and monthly examinations showed that a cost reduction effect could be obtained at the 200-km mark, even if the system installation and maintenance costs are 1.5 times higher than what was set in this study. On the other hand, at the 50-km mark, the cost reduction effect is not obtained even if expenses related to system installation and maintenance were half of what was set in this study. If the cost incurred for system installation and maintenance is half of the amount set in this study, a cost reduction effect is anticipated at the 100-km mark. According to company A's price packages, which were used in this study as reference points to set system installation and maintenance costs, the 100,000-yen system installation is considered relatively low. It is difficult to set system installation costs lower than this price now. However, if it becomes possible to reduce the system installation cost to approximately half of this amount, then cost-effectiveness might be found at the 100-km mark.
The cost reduction effect due to system usage duration was found with 1 year of continuous usage for the 200-km mark, and ∼2 years at the 100-km mark, because system installation and maintenance costs were lower than the doctor's round-trip travel costs. However, no cost reduction effect was seen at the 50-km mark, even after 5 years of successive usage. Considering that the depreciation life span for such equipment is normally 5 years, a cost reduction effect through continuous usage of the system could be seen only if the hospital was at least 100 km away from Sapporo.
Figure 2 shows that the cost reduction effect for hospitals that had installed the system was seen regardless of the number of examinations per month if the distance was more than ∼100 km. Furthermore, Figure 5 shows that this trend is not dependent on the distance. It was found that the number of examinations does not have any direct impact on the cost reduction effect. Only if a requesting hospital was located ∼100 km or more away from the imaging diagnosis center would the hospital's financial burden be reduced by installing the system even if the number of examinations was ∼30 cases per month.
Conclusions
This study clarified the conditions under which installation of a teleradiology system will reduce the financial burden of both patients and hospitals. For patients, a reduction in the financial burden can be anticipated by system installation regardless of the distance between the requesting hospital and the imaging diagnosis center. For requesting hospitals, a reduction in the financial burden can be anticipated by system installation under the conditions that (1) it is at a certain distance from the imaging diagnosis center, (2) an inexpensive system is selected, and (3) the system is used continuously. However, if condition 1 is not satisfied, the financial burden will not be reduced, even if conditions 2 and 3 are met.
Limitations of this study include the possibility that the expenses paid by patients were underestimated as the initial visit fee and reexamination fees were also required for face-to-face consultations with doctors. This study focused only on radiological examination; however, this is merely one stage of the diagnostic process. Therefore, our future task is to conduct an analysis that considers costs and the burden throughout a patient's entire medical care process. Furthermore, expenses paid by hospitals for a radiologist and an imaging diagnosis center as remuneration were not included. Although the remuneration was defined as equal between the scenarios in this study, this assumption might be inaccurate. Because the price set for system installation and maintenance and image diagnosis was expected to vary among companies, a comparison among companies is also considered a future task.
Footnotes
Disclosure Statement
No competing financial interests exist.