
Abstract
Background:
Up to 86% of oral cancer (OC) patients present at the late stage where survival is dismal. Limited access to specialist diagnosis is a significant factor for late presentation. The increasing use of smartphones presents an opportunity to use digital technology to facilitate early detection of OC.
Aim:
To evaluate the feasibility of using Mobile Mouth Screening Anywhere (MeMoSA®) to facilitate early detection of OC.
Methods:
A mobile phone app named MeMoSA was developed and the feasibility of integrating this for documentation of oral lesions, and communication between dentists and specialists for management decisions were evaluated. The experience of dentists and specialists in using MeMoSA was determined using qualitative questionnaires.
Results:
Communication between specialist and dentists using MeMoSA stratified cases and streamlined referral of patients. Twelve of 48 patients were found to have oral lesions or signs suspicious of cancer and 3 required referrals. The patient's compliance for referral was tracked with MeMoSA. All dentists agreed that MeMoSA could facilitate early detection of OC and believed that MeMoSA could assist in the identification of oral mucosal lesions through direct communication with specialists and continuous learning in the recognition of high-risk lesions.
Conclusions:
MeMoSA has the potential to be used to promote equitable health care and streamline patient management that could result in early detection of OC.
Introduction
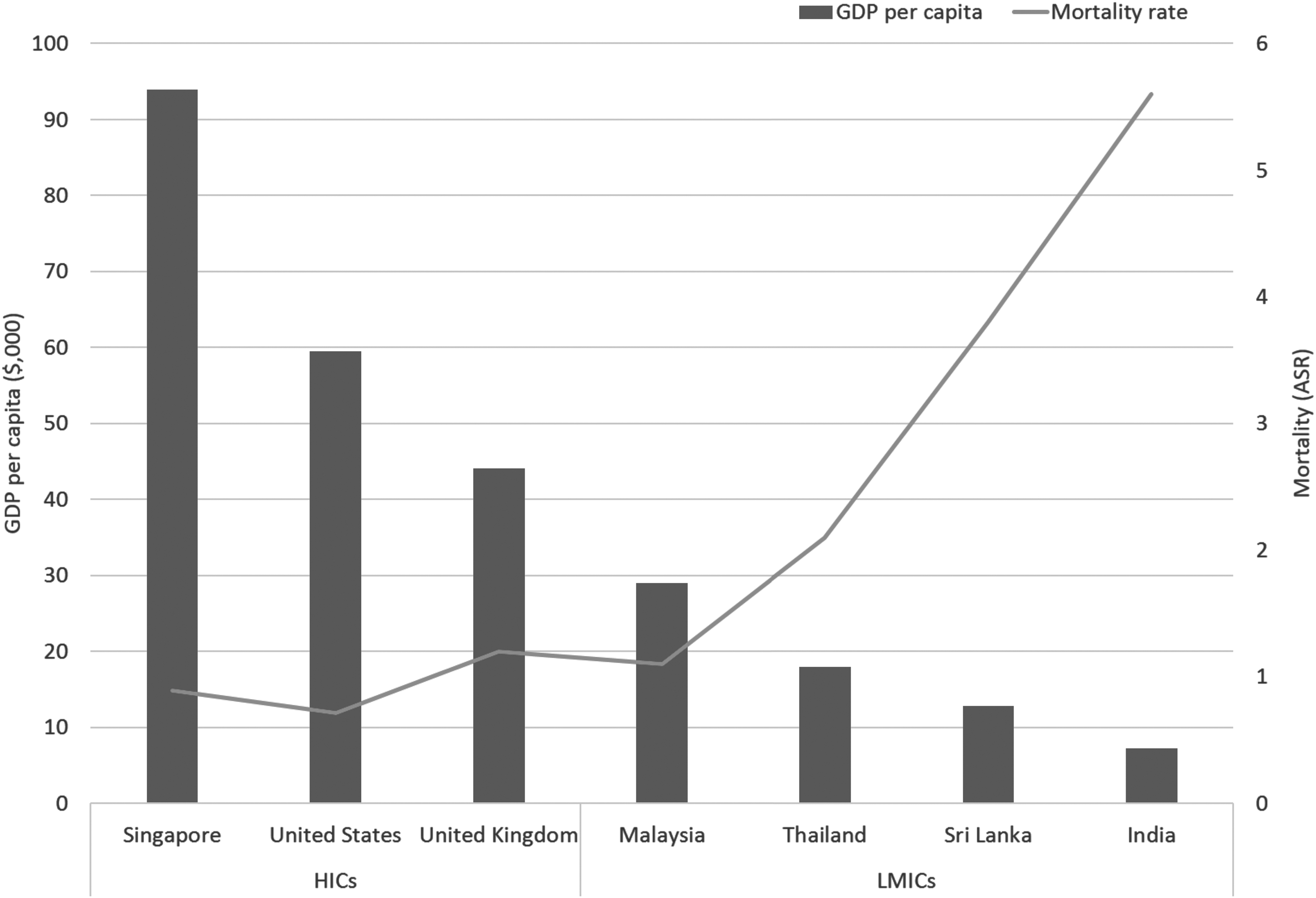
Oral cancer (OC) disproportionately affects low- and middle-income countries (LMICs) particularly those in the South and Southeast Asia (SEA) regions. 1 The age-standardized rate (ASR) for incidence and mortality of OC for SEA regions is 7.6/100,000 and 4.6/100,000, respectively, and icomparatively higher than the world ASR incidence and mortality rate that are 4.0/100,000 and 2.0/100,000, respectively. 2 Notably, low-socioeconomic status is a risk factor for OC 3 and the mortality rate associated with OC is inversely correlated with gross domestic product (GDP) of a country 2,4 (Fig. 1). This could be due to the practice of risk habits including smoking and betel quid chewing where income and education levels have been previously demonstrated to be associated with the lack of awareness of the disease and its risk factors. 3
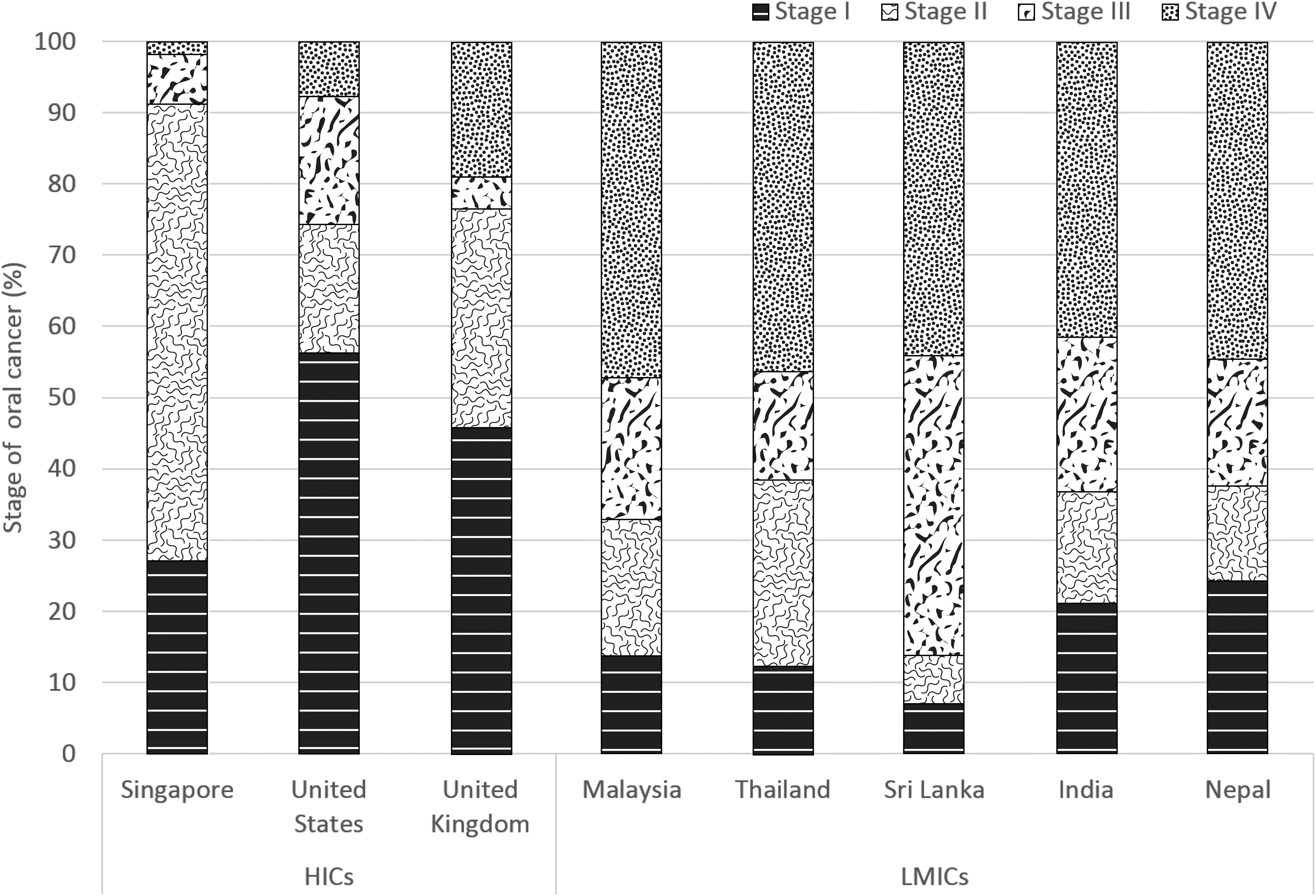
Correspondingly, a majority of OC patients in LMICs are diagnosed at late disease stages 5 –11 (Stages III and IV) where 5-year survival rates are severely compromised 12 –14 compared with those in high-income countries (HICs), where these cancers are diagnosed at earlier stages (Fig. 2). Fortunately, OC is one of the few cancers amenable to early detection without the need for expensive medical equipment. One major advantage is that up to 80% of OCs develop from a precursor lesion, and the oral cavity is amenable to visual examination, affording an opportunity to detect these lesions early for intervention to prevent malignant transformation to cancer. 15 However, challenges in early detection include the lack of expertise in recognizing high-risk lesions and geographical barriers in accessing diagnosis and treatment particularly in remote areas. 16 –20
For example, the ratio of dentists to the Malaysian, Thai, and Cambodian populations is 1:4,775, 1:4,374, and 1:10,667, respectively, compared with standards in developed nations where the ratio is about 1:2,000, whereas the number of oral specialists to the population in these LMICs is less clear. Furthermore, early detection and management of patients are also influenced by the accessibility to clinical management as demonstrated recently in Thailand, where despite the launch of the universal coverage scheme in the country, the survival of OC patients did not improve because of the difficulty of accessing medical care particularly for those patients living in remote areas. 13 Therefore, innovative wide-reaching and cost-effective strategies that enable equitable access to early detection of OC particularly in LMICs where the incidence is at its highest are critical if we were to improve survival of patients with this disease.
One recent innovation in health care that addresses geographical barriers and the limited accessibility to health care professionals is m-health. 19,21,22 m-Health can be defined as the use of mobile technology to provide or support clinical care at a distance to improve individual or population health care. 23,24 Usage of mobile phone itself has been rapidly increasing worldwide and particularly among LMICs. 25,26 The availability of third and fourth generation mobile coverage (3G/4G) in some LMICs are on par with the HICs (Fig. 3). 27 Although the connection speed across most networks in LMICs is lagging compared with HICs, this is not a major barrier to implement m-health in LMICs because the phone can operate as store and forward system where the data can be accessed, downloaded, and uploaded to the cloud in these LMICs even at the lowest speed. 28 –30
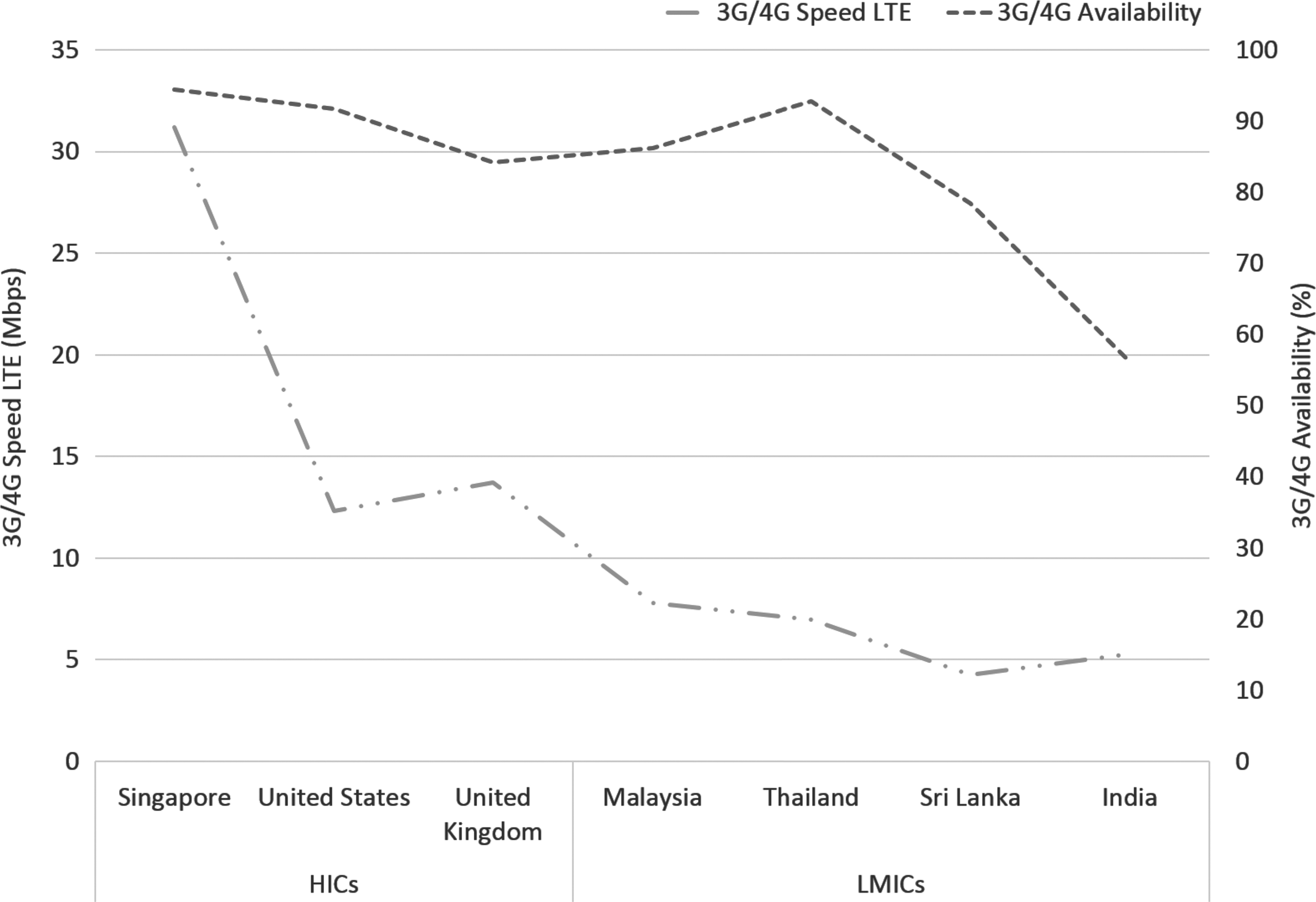
Third and fourth generation wireless mobile coverage (3G/4G) availability and speed in HICs and LMICs. Data source: Reference. 27
Our previous study has demonstrated that a mobile phone can be a sensitive and specific tool in early detection of oral mucosal lesions wherein a sensitivity of >80% for detecting a lesion, an accuracy of 87% for categorizing the type of lesion, and 85% concordance in patient referral between clinical oral examination (COE) and using a mobile phone were reached. 31 These findings suggested that using mobile phone for early detection of OC is feasible and comparable with standard COE. Moreover, discussion and communication between health care professionals involving images of the lesions inside the oral cavity also are found to be important for making a referral decision. 15,19,32,33 Moreover, mobile phone applications (apps) have been used for screening, remote consultation, and treatment planning for OC and cervical cancer. 19,34
In this study we describe the development of a novel app called Mobile Mouth Screening Anywhere (MeMoSA®) for easy documentation of oral lesions, secured communication between health care practitioners, and to improve referral accuracy during screening programs. Furthermore, we describe the testing of the app in a community setting to determine the feasibility of using such a tool in documenting the lesions and to communicate between health care professionals. We discussed the opportunities and challenges in using such an app, including the potential of using m-health to transform health care in low-resource settings.
Methods
Development of MeMoSA
MeMoSA is a store-and-forward mobile phone application (app) built on React Native as a platform for systematic documentation of disease presentation, and communication between health care practitioners (Fig. 4). MeMoSA is used for the collection of data including text and images. MeMoSA can be installed in any Android smartphone, and for this study, a phone with a 13 megapixel (MP) camera was used based on findings from our previous study where images taken with a 13MP camera gave high concordance in referral decisions when comparing with COE. 31 Using the app, the patient's demographic information, risk habit, and any signs that are suspicious of OC were entered manually by the dentists, and images of the mouth were captured systematically using the mobile phone camera operated through the app. The data that are captured using MeMoSA are automatically uploaded to the secured server in Malaysia using cellular data network, and if there is any interruption in internet connectivity, the data will be saved offline by MeMoSA and uploaded automatically to the server when an internet connection is available. Information can also be accessed from a customized design website through a secure login. To ensure information security, all health care practitioners are required to register before use and each will have a unique username and password to log on to the app and website.
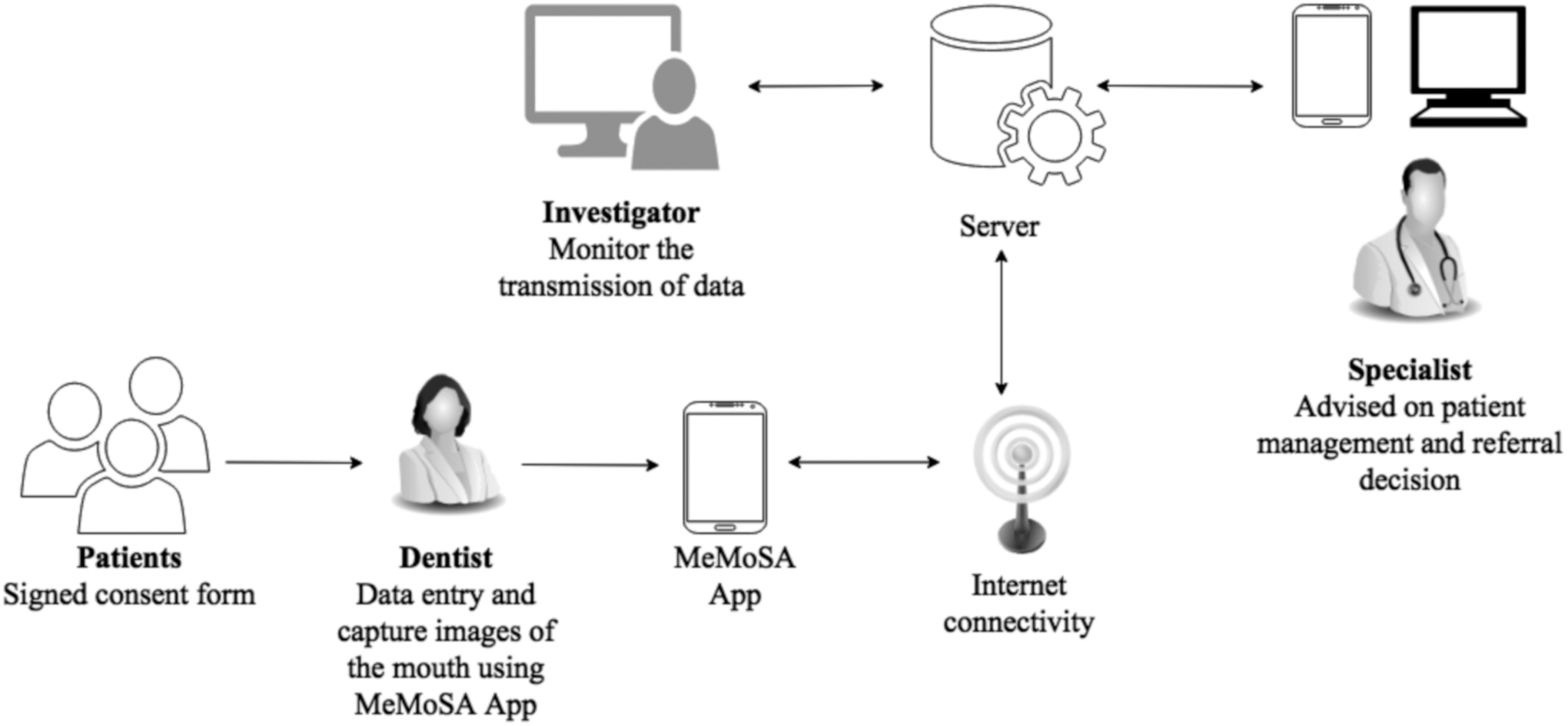
Framework of MeMoSA®. MeMoSA, Mobile Mouth Screening Anywhere.
Feasibility Testing of MeMoSA
To test the feasibility of using MeMoSA in the community, we tested the use of this app in conjunction with a routine screening program conducted by the Ministry of Health (MOH) Malaysia on November 4, 2017. This study was approved by the Medical Research Ethics Committee of the Ministry of Health, Malaysia (MREC; NMRR-15-763-25620). The screening was conducted in a village in Peninsular Malaysia where the nearest tertiary referral center was 42 km away. There is 3G/4G broadband internet coverage in this area. Before the community screening program, training on the use of MeMoSA was conducted. The public was invited to attend the screening through banners, radio advertisement, e-mail, social media, and through word-of-mouth through the village head.
Three oral specialists, 10 dentists, and 6 dental surgery assistants (DSAs) from the MOH Malaysia were involved in the screening program, wherein dentists performed the standard procedure of COE and added the use of MeMoSA to their routine procedures. The community screening program was conducted for a 7-h period (8am–3pm). Those who were interested registered themselves with MOH personnel at the registration counter in the community hall of the village. The criteria for inclusion in our study were consented individuals who are of age >18 years old. Information on risk habits and presence of suspicious signs were recorded and six images of the mouth with specific angles including (1) right buccal mucosa, upper labial/sulcus, and gingiva, (2) left buccal mucosa, upper labial/sulcus, and gingiva, (3) lower labial/sulcus and gingiva, (4) floor and ventral tongue with lateral tongue, (5) palate and upper lingual gingiva, and (6) dorsum/lateral and tonsil and two images focusing on the oral lesions (where present) were captured using MeMoSA. Information on risk habit and the mouth images of all patients who consented were sent by the dentists to the specialists for review. After a notification on the mobile phone, the specialists, who were not conducting the COE, reviewed the cases through a mobile phone and replied to the dentists using the app and indicated whether the patient should be referred for further examination by a specialist. The app allows further communication between the dentist and specialist through its chat function.
The feasibility, perception, and challenges associated with the use of MeMoSA were evaluated by conducting a survey on the dentists and specialists using a set of questionnaires that has been validated previously. 31
Results and Discussion
Seventy-eight individuals registered for the community screening program, of whom 48 met the inclusion criteria. Participants were informed about the study to evaluate MeMoSA during registration and informed consent was obtained. The response rate to participate in the MeMoSA study was 100%, with almost equal distribution between males and females (52.1% and 47.9%, respectively). The largest number of participants were from those who were 30–39 (31.2%) and 40–49 years of age (33.3%) with the mean age of 46 years (range: 25–76 years). Ethnic communities included in this study were Malay (85.4%) and Indian (14.6%). Focusing on the risk habits, 4 of 25 males and 2 of 25 males smoked and drank alcohol, respectively, and these were found exclusively among Malays. Betel quid chewing was observed only among Indian females (2/23) (Table 1). Twelve participants had suspicious signs that could be indicative of OC. Of these, eight participants had white/red patches, two had ulcers and another two had swelling in the neck (Table 2). As expected, the majority of the participants (75.0%) did not have any suspicious signs and symptoms of OC.
Demographic of Participants Who Were Screened
Referral Decision by Specialists
Each case was reviewed thoroughly by the specialists through MeMoSA and all of the images taken using MeMoSA were clear, and none of the images were uninterpretable (total of 288 images reviewed). Having reviewed the cases through the app, only three were recommended for further referral by the specialists. These included a 63-year-old male with bilateral white patches on the left and right buccal mucosa/sulcus and gingiva area indicative of lichen planus, which is an oral potentially malignant disorder recognized by the World Health Organization as one of the high-risk lesions that has a propensity to transform to OC. 35 Notably, this patient did not practice any risk habits and was not aware of the presence of these lesions before being alerted through the screening program. The other two individuals who required referrals were males of age 66 and 41 years old, respectively, with no risk habits. Both had swelling in the neck and already had appointments with the ear, nose, and throat specialist, and were advised to keep to these appointments. This highlights an important point in community screening wherein opportunistic screening is predominantly conducted on individuals with known risk habits, and in this setting, we could very well have missed individuals with high-risk lesions. 19
The other nine participants who did not require further referral had benign lesions including Fordyce spots (n = 2), betel quid stains (n = 2), erythematous spots due to cheek biting and denture (n = 2), racial pigmentation (n = 1), and aphthous ulcers (n = 2; Table 2). Using the image acquisition and communication functions, MeMoSA was able to provide a platform to facilitate the stratification of patients and to streamline referral where only high-risk cases were referred for further consultation. This can ease the need to make unnecessary visits to the hospital and reduce the congestion at the hospital that has been shown to cause longer patient waiting time and delay in diagnosis. More importantly, the availability of the imaging option on MeMoSA enabled the documentation of lesions that otherwise may have been missed by the patients themselves, promoting early detection and intervention. Although dentists are typically trained in recognizing high-risk lesions through COE, they were our primary health care practitioners of choice in the evaluation of MeMoSA so as not to miss any of these lesions if we had used untrained health care practitioners during this evaluation study. Notwithstanding, the identification of high-risk lesions could be difficult and subjected to interpretation that depends on experience, particularly for health care practitioners who do not encounter these lesions routinely, 36,37 underscoring the utility of MeMoSA in early detection of OC, particularly in low-resource settings where trained health care practitioners are not always accessible. At the end of this study, the participant with the suspicious lesion has been referred to the nearest MOH Hospital, according to the tracking system on MeMoSA, he has not attended the follow-up visit and health care professionals have contacted him with reminders to have his lesions checked.
To determine the feasibility and challenges in using the MeMoSA, a questionnaire was distributed to dentists and DSAs after the field testing. The data showed that 16 of 16 (100.0%) participants (dentists and DSAs) agreed that MeMoSA has the potential to improve early detection of oral mucosal lesion however, 3 (18.7%) highlighted the need to be cautious about the possibility of medicolegal issues. 23 The dentists and DSAs were pleased with the imaging function of the app as it provided a visual record of the lesions in the mouth for future comparison and learning. The majority of the dentists and DSAs (75.0%) took ∼20 min to record information on the patient, to ask the questions included in the MeMoSA, and to take six pictures within the mouth. This finding is same as another study where average time spent to capture five images of the mouth for review is also 20 min. 38 Although this may appear to be lengthy compared with COE, MeMoSA allows the visual record of the lesions and overall still saves time compared with unnecessary traveling time and cost incurred by patients to go to the hospital if the lesion does not require a referral.
Nevertheless, it is anticipated that time taken in using MeMoSA will become shorter when the dentists and DSAs become more familiar with the tool. Notably, the dentists and DSAs found that 90% participants were co-operative and did not complain about the use of MeMoSA. Seven participants seemed uncomfortable and this could have been due to a sense of guilt as they practiced risk habits and these were now being documented systematically. All dentists and DSAs stated that they would like to continue using MeMoSA as screening tool beyond the study and 13 of 16 (81.3%) would recommend the app to a colleague as they were motivated by the belief that the MeMoSA is user-friendly and it could assist in detection of oral mucosal lesions by providing a direct link to specialists. This finding is in line with other studies where the user is satisfied with using a mobile phone as a tool for remote screening of oral health through communication with off-site specialists. 19,39
Although MeMoSA is well received by the dentists and specialists as a tool for early detection of OC, intervention depends on the conscious effort of patients to seek treatment when they are referred. With a lack of urgency on the patient's part, early detection and intervention could remain challenging. Therefore, during the use of MeMoSA, educating the patient on the urgency of the referral is also important. A current limitation in the use of MeMoSA is that it is not yet been integrated into the national health care system, therefore, patient tracking could be challenging if the patient seeks treatment at specialist centers other than the appointed hospital. Therefore, early development of m-health should involve stakeholders including the public health care sector to inform on planning, policy development, and the possibility of developing an integrated health care system that can address these gaps to enable seamless implementation of m-health. 40
Conclusions
MeMoSA was able to document lesions within the oral cavity, and individuals with precancerous and benign lesions were identified through consultation within the functions of the app. With the wide-scale implementation of MeMoSA, logistical and access barriers hindering early detection of OC can be addressed, streamlining referral that could promote early intervention and maximize health care resources particularly in a low-resource setting where most OCs are diagnosed.
Footnotes
Acknowledgments
This study was funded by Berjaya Cares Foundation. We are grateful for the support and partnership from Oral Health Programme, MOH Malaysia; Oral Health Department, Selangor State Health Department; District and Land Office of Mukim Bandar/Jugra Kuala Langat; Oral Cancer Research and Co-ordinating Centre, University of Malaya; Dental Faculty, MAHSA University; and other supporters of Cancer Research Malaysia. Cancer Research Malaysia is a nonprofit organization committed to an understanding of cancer prevention, diagnosis, and treatment through a fundamental research program. We would also like to thank the Director General of Health Malaysia for his permission to publish this study.
Disclosure Statement
No competing financial interests exists.