
Abstract
Introduction:
Although some correlates of primary care physicians (PCPs) telemedicine adoption have been studied, little is known about whether the intention to use video-consultations (VCs) relates to how PCPs view their power, relative to other stakeholder groups in primary care. The aim of this study was (1) to describe PCPs', patients', and policy makers' (PMs) views of their power and (2) to explore how PCPs views of power are associated with their intention to use VC.
Methods:
A convergent parallel mixed-methods design was used. Interviews were conducted with five focus groups that comprised 42 patients; five focus groups with 52 PCPs; and 24 individual interviews with PMs. A total of 508 patients, 311 PCPs, and 141 PMs completed the questionnaire, assessing intention to use VC and stakeholders' relative power. The qualitative data were analyzed using the thematic method; survey data were analyzed using quantitative methods.
Results:
All stakeholder groups rated PCPs' power as significantly lower, relative to that of patients and managers. PCPs' intention to use telemedicine was found to be significantly related to perceived power gaps between them and patients (r = −0.24, p < 0.001) and between them and managers (r = −0.45, p < 0.001). Themes revealed in the analysis describing how PCPs' low power influences their intention to use VC were as follows: PCPs' low-impact telemedicine-related decisions, increased work overload, “big brother” control, and Health Maintenance Organization demands for telemedicine mandatory usage.
Conclusions:
To successfully adopt VC, efforts should be made to increase PCPs' relative power, by strengthening their involvement in decision-making procedures and by increasing PCPs' control over their work environment.
Introduction
Video-consultation (VC) is a telemedicine technology, provided by asynchronous (store-and-forward) or synchronous (real-time) digital interaction that uses both image and voice, to conduct medical consultation between the patient and caregiver. 1,2 VC integration in routine primary health care has the potential to increase clinics' accessibility, 3 –5 improve clinical outcomes, 6 –9 decrease hospitalizations and emergency visits, 10 –12 increase satisfaction with the provided services, 13 improve patient waiting time and experience, 14 and help reduce expenses and save time. 15 –17
Despite evidence in the literature regarding these benefits, VC adoption and usage rates have remained below expectations and the actual use of VC as a routine health service is poor. 18 –20 Physicians' and in this case, primary care physicians' (PCPs) willingness to use telemedicine technologies is one of the main factors influencing implementation success. As physicians' willingness appears to be relatively low, it becomes a barrier to the implementation of routine VC use. 21 –23 A recently published approach to telemedicine integration included 18 critical success factors. 24 In all of these factors, and especially during the first stages when readiness and leadership need to be created and the needs of key stakeholders must be identified, PCP attitudes and motivation to use telemedicine play a significant role. During these stages, PCPs who are usually still nonusers of the technology tend to be passive and lack proactive involvement. 25 –27 In addition, their perceptions about the new technology usually move from neutrality or nonresponsiveness to resistance to the use of telemedicine in everyday practice. 24,28
The following aspects were raised in the literature as having importance to PCPs in regard to VC implementation: identifying and using VC with appropriate patients; strategic planning; and integration of VC into work schedules, preventing possible job overload, funding, and other organizational issues. 28 –31 These findings encouraged us to look at PCPs' ability to influence these organizational issues, their power to set an agenda in relation to these subjects, to promote their agenda in the organization so that their preferences would be reflected in VC implementation plans. Therefore, PCPs' power relatively to other VC implementation stakeholders may be a factor in their intentions to adopt VC and we find this subject worthy of further exploration.
Key Stakeholders in Context of Telemedicine in Primary Care and their Power
Telemedicine in the public health sector is adopted in a complex organizational structure where various stakeholders' networks may influence the implementation. Hence, stakeholders' theory 25,32 –35 can provide a useful lens to investigate VC implementation phenomena. In the current research context, when VC is implemented in primary care for PCP-patient consultations, stakeholders can be defined as “individuals and groups who can affect or be affected by VC implementation in primary care.” 32,35 Using the Interpretive Stakeholder Analysis Methodology, 25 we defined three key groups of stakeholders involved in this VC implementation—patients, PCPs, and policy makers (PMs). Each one of these groups has different needs, interests, and preferences; accordingly, each group wants to reflect all of its needs in the VC implementation processes through the power it has. Stakeholders' power was defined by several theoreticians as “the probability that an actor in a social relationship will be in a position to carry out his own will despite resistance, regardless of the basis on which the probability rests.” 36 –40
The perceived power of one stakeholder group with regard to other stakeholder groups can be related to participation in organizational projects. 35,40 –42 For example, the stakeholder group that perceives its power as low, relative to other stakeholder groups within the system, may resist the implementation regardless of the nature of the technology itself, because it feels powerless to present and promote its needs and preferences in the implementation negotiations with other stakeholders.
To further examine this issue in the primary care system in Israel, we asked the following research questions: (1) What is the power of PCPs, compared with that of other key stakeholder groups—patients and PMs, and (2) is the relative power of PCPs related to their intention to use telemedicine?
The study aims to examine the research questions in the context of primary care in Israel. The Israeli health system is based on the national health law in which all citizens are entitled to receive health care services delivered by four Health Maintenance Organizations (HMOs) operating throughout the country. Primary care provides a strong infrastructure for the entire health system. More than 90% of patients have a personal family physician, 64% said they preferred their PCP to be their first health care contact person, and 49% reported turning to their PCP for every aspect of health care. 43 –45 As in other countries, in Israel, VC implementation is found in various strategic national and organizational programs. A sustainable digital infrastructure makes Israel well-prepared for VC adoption 46 : most patients have internet access and interact with PCPs via e-mail and HMO applications for prescriptions, referrals, and even medical issues. All of Israel's health care interactions are supported by a comprehensive electronic medical records system. Still, all study participants were nonusers of VC, as VCs are not yet being implemented for usage on a regular basis in any of the Israeli HMOs.
Methods
Using a mixed-methods approach, 47 we compared and integrated the quantitative data with the PCPs and other stakeholders' perspectives from the qualitative data, thus expanding the understanding of the topic under study. We followed recent guidelines for mixed-methods studies 47 –49 for designing and conducting, and The Good Reporting of Mixed Methods Studies template, which identifies the aspects of appropriate transparent reporting, 50 for reporting the study. The research team was multidisciplinary, including two senior PCPs and PMs (M.G., K.K.), as well as three behavioral science researchers (H.G., A.D.Z., I.C.). The team was diverse in terms of the methodological expertise of qualitative and quantitative methods, to adhere to the standards of each component. 50
Study Design
A convergent parallel design was used: data were collected through qualitative and quantitative methods concurrently and independently during the same time frame, in which separate qualitative and quantitative analyses were conducted, and data sets were merged in the discussion and interpretation stages. 50 Equal emphasis was given to qualitative and quantitative strands. This approach was chosen to allow more comprehensive understanding and to achieve triangulation and greater validity on stakeholders' power balances and its role in PCPs' intention to use VC. Figure 1 presents the study design. Data integration was done at the interpretation and reporting level. 51
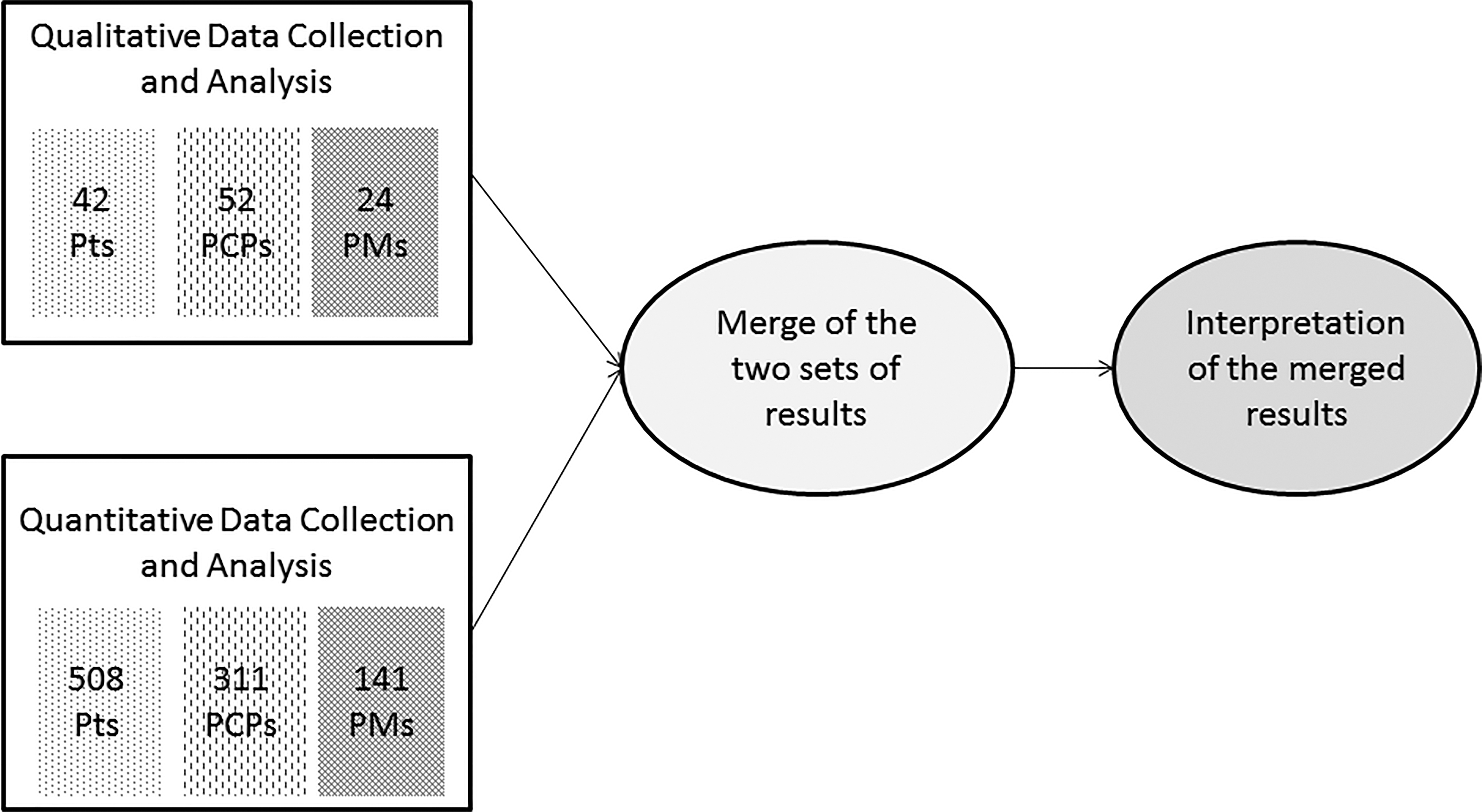
Convergent parallel study design among three stakeholder groups. Based on Creswell and Plano Clark's diagram. 47 Pts, patients, PMs, policy makers, PCPs, primary care physicians.
Data Collections, Samples, and Procedures
Qualitative data were collected through five focus groups that comprised 52 PCPs, five focus groups with a total of 42 patients, and 24 individual semistructured interviews with PMs. Convenience sampling was used for patients and PCPs, and purposeful sampling was used for PMs. Table 1 displays participants' characteristics. Patients' focus groups were conducted by a research institute, specializing in data collection among patients, that contacted patients by mail and invited them to participate in interviews. PCPs were approached face-to-face and recruited to the focus groups during their continuing medical education (CME) trainings. The PM group included national-level executive managers responsible for decision-making regarding primary care in Israel. The PMs were contacted directly, or via their secretaries, and were asked to participate in interviews. Experienced moderators conducted the interviews in Hebrew, which were audio-recorded and later transcribed verbatim.
Stakeholder's Characteristics in the Qualitative Component
Language and living status pertain to patients only.
C, Clalit; HMO, Health Maintenance Organization; L, Leumit; Ma, Maccabi; Me, Meuhedet; MH, Ministry of Health; MTO, more than one HMO; PCPs, primary care physicians; PMs, policy makers; PU, professional union.
The quantitative data were collected through a survey, completed by 508 patients, 314 PCPs, and 141 PMs. A sample of patients, ages >20 years, were contacted via e-mail with a link to the web-based questionnaire. Paper-based questionnaires were used with PCPs and PMs. PCPs were approached during their CME activities and PMs were recruited via a personal approach or at periodic executive managers' meetings in their HMOs. Table 1 presents qualitative stage participants' characteristics and Table 2 presents quantitative stage participants' characteristics.
Stakeholder's Characteristics in the Quantitative Component
ALTOR, Clalit Health Maintenance Organization name for patient-physician correspondence system; FTF, face to face; HMO, Health Maintenance Organization; NIS, New Israeli Shekel; PCP, primary care physician.
Research Tools
The qualitative phase interview guides included six to seven open questions about the integration of telemedicine, in general, and VC, in particular; power dynamics influencing primary care; required resources; drivers and barriers to the adoption of VC technologies; and the respondents' sociodemographic information. The interview's semistructured nature enabled an in-depth investigation of subjects according to the development of the particular interview conversation, and the unique perspective of each participant.
The quantitative survey included a relative power rating tool, intention to use telemedicine items, relevant sociodemographics for each stakeholder group, and more items that are beyond the scope of this study. The relative power tool was adopted from a previous study 35 and explored relative power by asking participants to rate their power relative to other stakeholder groups in primary care. The intention to use VC variable was used in the PCP survey and included three items, which were also adopted from relevant prior research. 52 Although validated by prior research, the variable was examined to ensure content validity and reliability within the targeted context for PCPs during pilot, because validity may not be persistent across different technology-user groups. 53 The intention to use variable had Cronbach's α value of 0.95, indicating a good reliability level. 54 Wording choices were solicited, and minor modifications were made in the survey following pilot. The full version of the survey can be found in the Appendix.
Data Analysis
Qualitative data analysis was performed inductively, 55 using a thematic analysis method. The researchers read the interview transcripts repeatedly, listened to the recordings, documented their first impressions, and prepared an initial analysis, noting keywords and phrases that potentially represented relevant themes. Themes that emerged from the initial analysis were examined for each participant's narrative, seeking connections, similarities, and differences, deleting redundant themes and categorizing themes and subthemes. Interactive coding trees were built separately for the three stakeholder groups. The quantitative data were analyzed using SPSS software: three repeated-measures tests (one for each stakeholder group) with a comparison of the main effects, using Bonferroni adjustment, were performed to identify holistic power gaps. Stepwise regression was used to predict PCPs' intention to use telemedicine according to their perceived power and their sociodemographic characteristics.
Results
Research Question 1: How is PCPs ' Power Rated, Relatively to that of Other Key Stakeholder Groups—Patients and PMs ?
The qualitative research
Four main themes and seven subthemes emerged from the qualitative data gathered in relation to the PCPs: (1) PCPs' power relatively to managers; (2) PCPs' power relatively to the patients; (3) PCP status; and (4) PCPs' ability to change the system. PCPs in all focus groups stated that, compared with the managers in HMOs, they are “powerless and lack control over basic elements” related to their “immediate working environment,” such as schedules and patients' workflow, autonomy on tasks, and time allocation decisions made during the workday. Data revealed that “the manager's pressure to perform many bureaucratic duties” contributed to PCPs' low sense of power. PCPs also mentioned shifts in the power balance, relative to the patients, because the “patients have undergone ‘some kind of change; today they have a completely different, stronger position.’” Data from patients' focus groups showed that patients also recognize the powerless position of their PCPs, relative to HMO managers: “The doctors have studied for many years, they understand, they have professional considerations…the people who tell them what to do are the ones who have been promoted to managerial positions—and they are not doctors …” In the personal interviews, few PMs, mainly those who were originally family practitioners, mentioned PCPs' powerless position. A theme that was unique to PM data was “the need for PCPs to develop strong leadership, take a more proactive attitude, define their own needs, and push to be involved in decision-making processes” as ways to increase their own power and “have a say” within the system. Table 3 presents the themes, subthemes, and citations of all stakeholders in relation to PCPs' relative power.
Stakeholders' Quotations Contributing to Themes on Role of Primary Care Physicians' Relative Power
The quantitative research
Table 4 presents the scores of patients, PCPs, and PMs rating their own and other stakeholder groups' relative power. Not only PCPs but also patients and PMs, rated PCPs' power as the lowest of all stakeholder groups. PCPs viewed managers and PMs, followed by the patients, as having more power than PCPs. Patients viewed PMs' power relative to that of PCPs as the highest, followed by their own power. PMs viewed patients' power relative to PCPs as the highest, followed by their own power. Self-employed PCPs rated their power (M = 3.08, standard deviation [SD] = 1.11) higher than that of PCPs who are employed by an HMO (M = 2.50, SD = 1.07), t(255) = 4.15, p < 0.001. A negative correlation was found between power rating and age, meaning that younger PCPs rated their power higher (r = 0.16, p < 0.01).
Relative Stakeholders' Power
F(2, 301) = 285.18, p < 0.001. Bonferroni: PCPs-PTs: p < 0.001; PCPs-PMs: p < 0.001; PTs-PMs: P < 0.001.
F(2, 506) = 339.98, p < 0.001. Bonferroni: PCPs-PTs: p < 0.001; PCPs-PMs: P < 0.001; PTs-PMs: p < 0.001.
F(2, 135) = 39.29, p < 0.001. Bonferroni: PCPs-PTs: p < 0.001; PCP-PMs: p < 0.001; PTs-PMs: non significant (p = 0.80).
PCPs, primary care physicians; PTs, patients; PMs, policy makers.
Comparison and Integration
Findings from both PCPs' and patients' data sets present a similar picture, indicating PCPs' low power relative to the two other groups of key stakeholders examined in the study. In the PMs' quantitative data set, they rated PCPs as the lowest-strength group, which is consistent with PCPs' and patients' ratings. In contrast, in the in-depth interviews, PMs somewhat avoided relating to PCPs' power within the health care system, but chose to relate to PCPs' status, PCPs' involvement in decision-making, and the need for PCPs' leadership development.
Research Question 2: Is The Relative Power of PCPs Related to their Intention to Use VC?
The qualitative research
Four main themes emerged from the PCPs' qualitative data describing how PCPs' low sense of power influences their intention to use VC: (1) We cannot impact decision-making; (2) “Big brother”; (3) Mandatory usage demands; and (4) Work overload. PCPs' quotations, supporting these themes, are presented in Table 5.
Primary Care Physicians' Quotations on Role of Low Relative Power in Their Intention to Use Video-Consultation
PCP, primary care physician; VC, video-consultation.
The quantitative analysis
A stepwise regression for the prediction of PCPs' intention to use VC was conducted (Table 6). The following sociodemographic variables were entered in Step 1: PCP age, specialty, graduation country, employment type, number of patients, use of social media, and use of internet shops, Skype, or other video application usage. In Step 2, the perceived PCPs' power was entered. The model explained the overall 26.0% of the variance in the predicted variable [F(4, 192) = 16.90, p < 0.001]. The regression showed perceived power to be the best predictor of the PCPs' intention to use VC (β = 0.32, p < 0.001), followed by employment type (β = 0.21, p < 0.01), with self-employed practitioners having higher intentions to use telemedicine. Graduation country also proved to be a significant predictor (β = −0.13, p < 0.05), with practitioners who graduated medical school in Israel having a higher intention level to use telemedicine compared with those who graduated in Eastern Europe and the former Soviet Union. In addition, a t test analysis also showed a positive correlation between previous usage of video call applications (such as Skype) and the intention to use VC (r = 0.18, p < 0.01).
Stepwise Regression Predicting Intention to Use Telemedicine by Perceived Power and Sociodemographic Background
Comparison of Integration
The qualitative findings of the second research question are congruent with the quantitative finding, presenting a significant connection between PCPs' low sense of relative power and intention to use VC. PCPs' previous experiences of telemedicine implementation in HMOs, which were characterized by mandatory usage demand, and lack of ability to influence decisions and implementation plans influenced they motivation to use VC. They expressed concerns about additional work overload, and the fact that the VC issue will give HMO-employed PMs and managers yet another convenient tool with which to control them.
Discussion
This study presents a broad picture of the relative power of PCPs, drawing a line between the power felt by PCPs and their intention to use VC. PCPs' relative power is mapped and validated from several angles and points of view, as expressed by the three critical stakeholders—the PCPs themselves, the patients, and the PMs. The study presents an unequivocal picture of PCPs' low power relative to the managers and the patients. This picture supports findings in the literature about shifts in primary care balance of power, resulting from reforms, the generally turbulent primary care environment, and the long-term trend of gradual power shifting from the medical profession to the management. 35,56 –64 To the best of our knowledge, the study shows for the first time an empirical link between the relative power of PCPs and their intention to use VC: PCPs' low perception of their relative power reduces their intention to use VC. Our explanation for this phenomenon is that as a result of PCPs' relatively low power experiences, they doubt their own ability to impact telemedicine implementation decision-making and express their needs and interests in the negotiations around VC implementation plans.
Apparently, the link between PCPs' perceptions about their own power and their intention to use telemedicine is not only unique to the VC integration case but also relevant to other types of telemedicine implementations. PCPs' diurnal work has become more intense, closely monitored, and routinized, while their power continues to diminish. 55 Thus, telemedicine implementation becomes a focal point in which power gaps are expressed in the different stakeholders.
To successfully adopt VC and, in particular, to ensure that primary care remains a strong sustainable platform for telemedicine implementation, in general, efforts should be made to increase PCPs' relative power. This can be achieved not only by involving PCPs in the implementation processes but also by building a system in which PCPs lead these processes. This is an important factor, as an effective significant medical leadership seems to be crucial for e-health effectiveness. 65 PCP leadership can make a significant contribution to implementation success factors, 24 both in the stages of more strategic nature, such as mapping the needs of all stakeholders, and in stages of more operational nature, such as the establishment of good procurement processes, construction of workflows, PCP-patient communication through VC trainings, and more.
The study has several limitations. The first limitation is the fact that the study was conducted within the framework of the Israeli primary care model, including about 50% of PCPs who are HMO employed and the others work in semiprivate clinics on a contract with one of the four HMOs. That could limit the generalizability of the study, although in general, the Israeli health system, based on the national health law, which insures health services for all, resembles health systems in other countries. The second limitation refers to the patient population. Since the survey was conducted via web-panel, elderly patients who do not have a computer did not have an opportunity to respond to the survey; therefore, they are not represented in this study.
Conclusions
We found a negative impact of low PCPs' relative power on their intention to participate in telemedicine implementation. Hence, effective and timely VC implementation requires careful attention to PCP power and ways to increase it.
Footnotes
Acknowledgments
The authors thank all the study participants: PCPs, patients, and PMs. All authors contributed to the study design and to the data collection. I.C., H.K., A.D.Z., and H.G. conducted the analysis, interpreted the results, and reviewed the article. This study was part of a larger study, titled: “Family Medicine—Quo Vadis?” This aimed to examine the desirable directions for family medicine development over the next 10 years, in accordance with the changing work environment and telemedicine. Funding: The qualitative stage in the present study and the patients' quantitative survey comprise part of a larger study entitled “Family Medicine—Quo Vadis?” This was funded by The Israel National Institute for Health Policy Research, grant no. 2020947. Its publication is not contingent on the sponsor's approval. No funding was received for the PCPs' and PMs' surveys.
Ethical Approval
The study was approved by the Institutional Review Boards (IRB) of the University of Haifa and the Technion. All participants in personal and group interviews signed an informed consent form of participation.
Disclosure Statement
No competing financial interests exist.
Appendix
Note: The interview guides were created in Hebrew and translated to English for the purposes of the article.