
Abstract
Background:
Women with breast cancer (BC) commonly experience physical and psychosocial symptoms after surgery. Web- and smartphone-based support can significantly improve women's symptoms and quality of life. Social care applications (apps) are widely used in China, but there are few studies on their effectiveness BC support. This study aimed to examine the effects of nurse-led support on the social care app WeChat® (Tencent Holdings Limited, Shenzhen, China) in BC patients after surgery.
Methods:
A quasi-experimental study was conducted between June 2015 and August 2015. Sixty patients with BC (30 in the intervention group, 30 in the control group) were enrolled. Subjects in the intervention group participated in a WeChat-based support program (WSP) led by nurses, while subjects in the control group received a follow-up by telephone. Subjects in both groups were evaluated at the time of discharge and at 1, 3, and 6 months of follow-up. Physical well-being status, psychology status, and social support were evaluated.
Results:
There were no differences between intervention and control patients at baseline. Physical well-being (p < 0.001), anxiety (p < 0.001), depression (p < 0.001), and support from outside of family (p = 0.037) were significantly better in the intervention group than in the control group after 6 months. The intervention group showed that physical well-being (p = 0.036), anxiety (p < 0.001), and depression (p < 0.001) were significantly different from baseline to 6 months of follow-up.
Conclusion:
WSP assisted with nurse-led support and had physical, psychological, and social benefits for patients after surgery for BC.
Introduction
Breast cancer (BC) is one of the most commonly diagnosed cancers in women worldwide. 1 Although the incidence of BC in China is lower than in Western countries, it has increased rapidly, with >1.6 million new cases diagnosed each year, representing 17.1% of female cancers. 2 BC patients experience both physical and psychosocial symptoms during treatment and recovery, such as complications after various treatments, risk of cancer recurrence, fatigue, sexual disorders, functional limitations, negative mood, and feelings of social isolation. 3 –5 A Chinese study found that 88% of BC patients reported at least one of these symptoms, whereas 51% had unmet needs including lack of information and of long-term physical, psychological, and social support during the post-treatment period. 6
With the rapid expansion of smartphone ownership across the world, numerous smartphone applications (apps) have been developed for many chronic diseases such as diabetes, 7 chronic obstructive pulmonary disease, 8 and heart failure 9 to deliver personalized health information and health data monitoring. Social networking tools, such as Facebook, have also been used for health communication, promoting healthy behaviors, and providing social support in cancer patients follow-up. 10 –13 Although Facebook is unavailable in mainland China, a similar social networking app called WeChat® (Tencent Holdings Limited, Shenzhen, China) (or Weixin in Chinese; launched by Tencent Co. in 2011) is becoming one of the most popular mobile social media platforms. It offers free instant messaging, transmits real-time messages, video calls, group chat, pictures on the WeChat activity timeline (Moments), photo and update sharing with contacts, and status updates with illustrations. There is potential for WeChat-based health interventions to impact populations and deliver follow-up health care to patients after discharge with high adherence rates and high satisfaction. 14 Nevertheless, few studies have evaluated the potential of this kind of social networking tool as an intervention delivery channel for Chinese BC patients.
In this study, we conducted a pilot study to compare WeChat-based follow-up with telephone follow-up of BC patients after surgery. The aims of the study were to (1) determine the effects of the WeChat-based follow-up intervention on health status, physiological distress, and social support and (2) preliminarily investigate the feasibility of using WeChat as an assistant and method for nurses to provide on-going follow-up support.
Subjects and Methods
Study Design and Sample Characteristics
This was a quasi-experimental study. BC patients who underwent surgery were recruited at the Shanghai Tenth People's Hospital. Between August 2015 and October 2015, patients were recruited into the control group. Between November 2015 and December 2015, patients were recruited into the intervention group. The inclusion criteria were (1) ≥18 years of age, (2) diagnosed with BC within the past 6 months, (3) underwent BC surgery for the first time, (4) local Shanghai resident, (5) ability to read and write, and (6) owns a smartphone with an active WeChat account. The exclusion criteria were (1) undergoing second surgery for progressive disease or recurrent BC; (2) with other primary cancer; (3) with psychiatric history; (4) life expectancy <6 months; or (5) with severe comorbidities, including pulmonary diseases, cardiovascular diseases, heart failure, renal diseases, or severe orthopedic conditions. This study was approved by the Ethics Committee of Shanghai Tenth People's Hospital. All participants signed informed consent forms before data collection.
Procedures
The patients in the intervention group were taught how to use WeChat and relative functions of the app. After being enrolled in this study, they received a WeChat-based support program (WSP) led by nurses. Each nurse was responsible for up to 10 patients and was informed about the patients' treatment plan and future rehabilitation regimen in advance. All the nurses involved in the intervention arm were the same as those who supported the control group, and they received an extra week of training before the intervention.
Intervention
In the intervention group, nurses released educational messages related to (1) dealing with potential symptoms, (2) management strategies on adverse events, (3) management strategies on distress and negative mood, (4) physical exercise and activities, and (5) diet. All the educational messages were the same as the content in the health-care guidance manual provided by the hospital to the control group and had been edited before the intervention started. Messages were designed as a hyperlink sent to the specific patients who were receiving certain treatment at each stage. The patient could click the message link, which came up with detailed context, pictures, and videos created by the hospital.
All patients could consult the nurses through text, voice messages, and video call, as well as use the group chat function through WeChat. The nurses could reply in the same way. Nurses assessed patients' needs and complaints dynamically according to the communication, adjusted the information they provided, and dealt with problems. Nurses used skills such as comforting, explanation, and encouragement to guide the patients to voluntarily express their symptoms and mental stress.
The patients were encouraged to ask questions, share their experiences, and express worries and concerns of treatment and recovery in the group chat. Nurses also shared successful examples of those who had adjusted well after treatment of cancer. The patients in the peer group could talk to others with similar experiences and symptoms through group WeChat.
WeChat Movement is an affiliated function, which records the number of steps a user takes. The users can check their own daily steps and those of their friends who also use WeChat Movement. The patients were asked to report their physical exercise improvement to the nurse through WeChat every week. The patients received personalized text or voice messages for appointments, adjuvant therapy plans, updated rehabilitation programs, or evaluation.
The patients in the control group received a health-care guidance manual after treatment and educational information, which was the same as the information provided to the intervention group, on the day before their discharge. Patients received follow-up by telephone at 1, 3, and 6 months after discharge. Nurses called them to address their physical and psychosocial needs, symptom assessment, medication compliance, and adverse events of adjuvant treatment. The patients could call back for consultation or support at any time during the workweek.
Measures
The Hospital Anxiety and Depression Scale (HADS) is a self-reported questionnaire that measures anxiety and depression for patients with physical illness during the past week. It contains two 7-item subscales, which measure anxiety and depression, 15 respectively. Each item is rated on a 4-point Likert response scale ranging from 0 (not a problem) to 3 (severe problem). Higher scores represent higher degree of anxiety and depression. The validated Chinese version of HADS (C-HADS) showed good internal consistency and acceptable concurrent validity in Chinese Mandarin-speaking cancer patients, with the Cronbach's α ≥ 0.820. 16
The Multidimensional Scale of Perceived Social Support (MSPSS) assesses perceived social support. 17 The Chinese version of MSPSS (C-MSPSS) consists of 12 items with 2 subscales that detect perceived support from family, and support from outside the family (friends and significant others). Responses were on a 7-point Likert scale ranging from 1 (very strongly disagree) to 7 (very strongly agree) that was used for scoring each item. The total scores ranged from 12 to 84, with higher scores indicating higher perceived social support. Cronbach's α of the C-MSPSS was 0.92. 18
Medical Outcome Study of the Quality Of Life Inventory (MOSQOL-72) assesses the physical aspects of BC patients' quality of life (QOL). 19 The MOSQOL-72 includes 72 items with 4 subscales. Considering the focus of the current analysis, we used the physical well-being subscale of MOSQOL-72, including sleep/rest and energy (5 items), pain and physical discomfort (4 items), eating ability (3 items), and capability of daily living (11 items). The scale was validated in the Chinese BC population, and showed acceptable reliability, validity, and sensitivity. 19 This scale ranged from 0 to 100 with increasing scores indicating better functioning.
Data Collection and Follow-Up
Demographic and clinical data were collected during face-to-face interviews and through medical records before discharge, including age, education level, marital status, working conditions, time since cancer diagnosis, tumor-node-metastasis (TNM) stage at diagnosis, and treatment. Patients in the intervention group were required to complete the instruments by WeChat, whereas patients in the control group completed the instruments delivered by e-mail or post. Data collection was carried out at baseline and at 1, 3, and 6 months after discharge.
Statistical Analysis
All data analyses were performed using SPSS 22.0 (IBM Corp.). Continuous variables are expressed as mean ± standard deviation (SD) and were compared using independent t-test between groups. Categorical variables are expressed as frequency (percentage) and were compared using the chi-square test between groups. The repeated-measure analysis of variance (ANOVA) and post hoc least significant difference (LSD) test were used to compare intragroup differences at different time points. p < 0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics of the Patients
A total of 85 patients were recruited in the study, 46 in the control group and 39 in the intervention group. Seven patients in the control group and nine patients in the intervention group were excluded due to loss to follow-up. Thirty patients in the control group completed 6 months of assessment, whereas nine patients were lost to follow-up. All 30 patients in the intervention group completed the entire assessment with high adherence (Fig. 1). The mean age of the patients was 56.6 years (SD = 7.9) in the control group and 55.1 years (SD = 8.8) in the intervention group. There were no statistically significant differences between the two groups in terms of the demographic and clinical characteristics (Table 1).
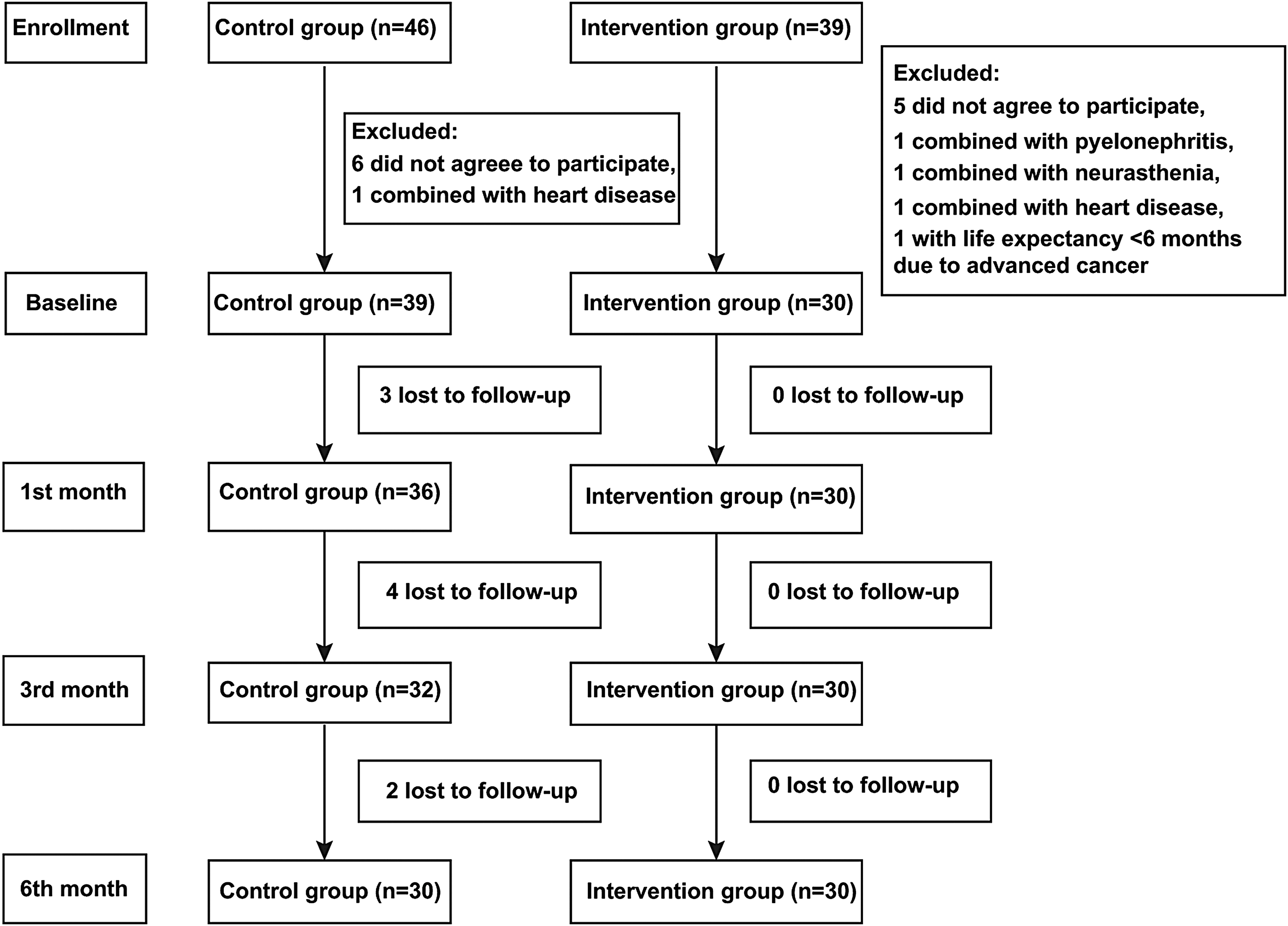
Study flowchart.
Demographic and Clinical Characteristics
SD, standard deviation; TNM, tumor-node-metastasis.
Physical Well-Being Status
The total physical well-being subscale (p = 0.762) and the sleep/rest and energy (p = 0.811), pain and discomfort (p = 0.406), eating ability (p = 0.796), and capability of daily living (p = 0.988) did not differ significantly between the two groups at baseline. There were statistically significant differences between the two groups in total physical well-being (p < 0.01), eating ability (p = 0.044), and capability of daily living (p < 0.01) at the 6-month time point (Table 2).
Differences of Physical Well-Being, the Chinese Version of the Hospital Anxiety and Depression Scale and the Chinese Version of the Multidimensional Scale of Perceived Social Support During Four Time Points Between Two Groups
p < 0.05 versus the intervention group; ** p < 0.01 versus the intervention group.
C-HADS, the Chinese Version of the Hospital Anxiety and Depression Scale; C-MSPSS, the Chinese Version of the Multidimensional Scale of Perceived Social Support.
Repeated-measure ANOVA showed for the total score of physical well-being subscale MOSQOL-72 that there was a significant difference (p = 0.036) in the intervention group and no significant difference (p = 0.967) in the control group. LSD correction in the intervention group revealed that there was a significant difference between baseline and 6-month follow-up (p < 0.05) in the total scores of physical well-being subscale of MOSQOL-72. For sleep/rest and energy, repeated measure ANOVA in each group showed a significant difference (p = 0.042) in the intervention group and a significant difference (p = 0.031) in the control group. The intervention group showed a significant difference from 3-month follow-up in the subscale of sleep/rest and energy, whereas the control group showed a significant difference at 6-month follow-up. For pain and discomfort, repeated measure ANOVA in each group showed a significant difference (p = 0.042) in the intervention group and a significant difference (p = 0.017) in the control group. The intervention group showed a significant difference from 3-month follow-up, whereas the control group showed a significant difference from 1-month follow-up. For eating ability, repeated measure ANOVA showed no significant difference (p > 0.05) in the intervention group and a significant difference (p = 0.033) in the control group. LSD correction in the control group revealed that a significant difference was found only between baseline and 1-month follow-up (p < 0.05). There were no significant differences in the intervention group or control group in the capability of daily living at 6-month follow-up (Tables 3 and 4).
Intragroup Comparison of Physical Well-Being, the Chinese Version of the Hospital Anxiety and Depression Scale and the Chinese Version of the Multidimensional Scale of Perceived Social Support Between Different Time Points in the Intervention Group
The p values are the results of the measurement of the main body effect (measurement time) in the repeated ANOVA. No intragroup comparison (-) was conducted if variance analysis is not significant. Posthoc LSD test was conducted if the variance analysis is significant.
p < 0.05 versus baseline; # p < 0.05 versus post 1 month; & p < 0.05 versus post 3-month.
ANOVA, analysis of variance; C-HADS, the Chinese Version of the Hospital Anxiety and Depression Scale; C-MSPSS, the Chinese Version of the Multidimensional Scale of Perceived Social Support; LSD, least significant difference.
Intragroup Comparison of Physical Well-Being, the Chinese Version of the Hospital Anxiety and Depression Scale and the Chinese Version of the Multidimensional Scale of Perceived Social Support Between Different Time Points in the Control Group
The p values are the results of the measurement of the main body effect (measurement time) in the repeated ANOVA. No intragroup comparison (-) was conducted if variance analysis is not significant. Post hoc LSD test was conducted if the variance analysis is significant.
p < 0.05 versus baseline; # p < 0.05 versus post 1 month; & p < 0.05 versus post 3 month.
C-HADS, the Chinese Version of the Hospital Anxiety and Depression Scale; C-MSPSS, the Chinese Version of the Multidimensional Scale of Perceived Social Support.
Perceived Social Support
The mean scores of total C-MSPSS (p = 0.832) and the subscales of support from family (p = 0.966) and support from outside of family (p = 0.803) did not differ significantly between the two groups at baseline. There were no statistically significant differences between the two groups in total C-MSPSS (p = 0.209) and support from family (p = 0.578) at the end of 6-month follow-up. Nevertheless, the subjects in the two groups showed statistically significant differences in the support from outside of family (p = 0.037) (Table 2).
Repeated measure ANOVA showed no significant differences (p > 0.05) in the total C-MSPSS and the subscale of support from family in the intervention group or control group. For anxiety and depression, LSD correction showed significant differences between baseline and 6-month follow-up (p < 0.05) ( Tables 3 and 4 ).
Anxiety and Depression Scales
The mean scores of total C-HADS (p = 0.617) and the subscale of anxiety (p = 0.641) and depression (p = 0.836) did not differ significantly between the two groups at baseline. There was a statistically significant difference between the two groups in total C-HADS (p < 0.01), anxiety (p < 0.01), and depression (p < 0.01) at the end of the 6-month follow-up (Table 2).
Repeated measure ANOVA showed significant differences (p < 0.05) both in the intervention and in the control groups in the C-HADS, anxiety, and depression. Repeated measure ANOVA in each group showed a significant difference (p < 0.01) in the intervention group and significant difference in the controlled group (p < 0.01) for both subscales of anxiety and depression. LSD correction showed a significant difference between baseline and 6-month follow-up (p < 0.05) in the intervention group ( Tables 3 and 4 ).
Discussion
This study suggests that WeChat-based messages for education and reminders can improve physical health. Previous findings have also demonstrated that intervention messages persuade people to increase their physical activity 20 and change dietary behavior. 21 Compared with a manual, the WSP support was able to be a more situation-specific intervention. Text messaging during follow-up was supposed to enhance health service provision, encourage better disease self-management practices, and deliver personalized and changing health promotion needs. 22 We also used an add-on function by WeChat to show the daily number of steps walked and compared the number of steps of users with number of steps of their friends. Aerobic physical exercises improve fatigue and QOL in BC patients. 23 In contrast with other kinds of aerobic exercises such as resistance exercise, which should be implemented supervised by professionals in rehabilitation settings, walking and jogging seemed more accessible and safer for BC patients in the community and at home. 23
Compared with a previous study of BC patients after surgery, the level of anxiety of patients in this study was similar at baseline, but the level of depression was slightly higher. 24 For most BC patients, anxiety and depression often persist throughout the entire treatment course, especially during chemotherapy. 25 The levels of depression and anxiety are affected by support from psychologists and the presence of a person to share their concerns. 26 Another study also proved that the level of anxiety and depression significantly dropped with psychological therapy in the form of a workshop at the 3rd and 6th month, respectively. 24 These findings might be explained by anxiety that comes from uncertainty associated with future treatment and the effect of rehabilitation. Providing helpful information and professional support could reduce this emotional distress in BC patients. Lu et al. 27 found that Chinese BC patients who were highly ambivalent over emotional expression had increased risk for depressive symptoms. In this study, the coaches encouraged patients to express their feelings and thoughts by group chat or by talking with their nurse in private, which reduced the embarrassment of face-to-face contact.
Social support is an essential component of comprehensive cancer care. 28 It plays an important role in enhancing patient outcomes. 29 We found patients in both groups showed no significant change in perceived social support from inside of family members. This finding may be explained by Chinese BC patients being unwilling to burden their family in case of role reversal during the illness. 30 Therefore, peer group relationships developed outside of the family network could serve as a supplement platform for BC patients to gain both informational and emotional support. Cheng et al. 30 indicated that social support satisfaction is more critical than support network size in influencing various aspects of patients' QOL through the underlying different types of situation-specific support. Therefore, patients in a small group might be more accessible for resource and personal support. Group leaders should keep a balance between professional and peer support, as well as controlling the sharing, such as encouraging positive moods and ideal behavior, correcting any wrong suggestions and negative moods in group chat. 31
This study integrated several functions of the social networking app into the WSP. Physical, psychological, and social factors are likely to be associated with each other during BC survival. For example, physical symptoms such as sleeping disorder and fatigue are related with both depression and anxiety, whereas physical function, pain, and arm symptoms negatively affect patients with depression. 26 Patients who are supported by social groups are less depressed and anxious, 32 and are more knowledgeable about their illness, treatment, and management of side effects. 29,31
We were able to establish the feasibility of using a social media platform (such as WeChat) to provide information and support to BC patients in this study. All 30 participants in the intervention group completed the 6-month measurements. This high level of adherence was probably due to the fact that nurses were able to keep a long-term relationship with participants through WeChat. The interactive communication targeting physical and psychosocial benefits may have contributed to maximize the level of adherence. There is an opportunity to improve the communication between BC patients and health care professionals by using WeChat. Nurses and other health care providers can directly impact and potentially improve the health of cancer patients during this critical time of survivorship.
There are some limitations in this study, such as its small sample size recruited from one site and nonrandomized control. There was reluctance of spousal partners and other health providers to be involved, and a lack of multidisciplinary team support, who could provide more professional guidance. Moreover, further studies are needed to identify the impact of the relationship between physical, psychological, and social dimensions, and the components of the three dimensions that play key roles or have mediating effects. We also recommend studying the relationship between frequency that subjects used the app and their health outcomes. Finally, future studies should include objective measurements such as urgent care or clinic visits, difference in objective performance such as ability to work or care for family members, physical endurance measured objectively, wound healing or complications, and cost to the health care system. Cost-effectiveness analysis could also be performed in future studies.
Conclusions
This study suggests that a WSP is a feasible and effective way of providing patients who have undergone surgery for BC with continued, individualized, and timely education, facilitates on-going communication between patients and health care providers, and provides peer support from patients with similar treatment experiences. The use of a WSP can improve BC patients' physical status and perceived informational and emotional support from outside of family and decrease their level of anxiety and depression. Oncology nurses should be encouraged to use similar social network apps to support BC patients during follow-up.
Footnotes
Acknowledgments
The authors acknowledge the contributions of the study patients and data analysis assistance by Pro. Tao Zhou in Nanchang University. This study was supported by two projects of National Natural Science Foundations of China (Grant Nos. 71704135 and 71774117).
Disclosure Statement
No competing financial interests exist.