
Abstract
Background:
The low participation rate in cardiac rehabilitation programs is the major reason for rehospitalization, morbidity, and mortality. Home-based cardiac rehabilitation by technological means is an essential component of a “patient-centered” approach, which is capable of enhancing the participation rate in rehabilitation programs.
Introduction:
The aim of this research was to examine attitudes, perceptions, and behavioral intentions toward remote digital cardiac rehabilitation (RDCR) with respect to factors such as age, education, smoking, exercise habits, technological illiteracy, and mobile phone behavior.
Materials and Methods:
This was a cross-sectional study of 200 adult patients discharged from a hospital after an acute coronary syndrome, cardiac surgery, or percutaneous coronary intervention. All patients answered an anonymous Technology Usage Questionnaire, which examined the relationship between their willingness to participate in the RDCR program and various parameters. The surveys were distributed and completed between July 2017 and November 2017 at the Sheba Medical Center in Israel.
Results:
Overall, 83% of all participants were interested in participating in the RDCR program. Those with heart failure had a greater interest in the program (100%; p < 0.05), whereas patients after coronary bypass surgery had a lesser interest (71.1%; p < 0.05). The level of attitude toward healthy lifestyle was found to be a significant predictor of willingness to participate in RDCR (odds ratio 2.26; p = 0.01). Sociodemographic characteristics, lifestyle, habits, technological knowledge, age, and gender were not found as significant predictors of interest in RDCR.
Conclusions:
The RDCR program was acceptable to most cardiac patients, including the elderly population, and could be a potential solution for patients who avoid traditional rehabilitation programs in medical centers.
Introduction
Among patients who experience cardiac events, rehabilitation by physical activity is an essential treatment component to improve risk factors, reduce the risk of event recurrence and death, rehabilitate normal functioning, and improve quality of life. Nevertheless, less than a third of patients take advantage of their right to participate in rehabilitation program within the framework of hospitals, mainly due to incompatibility of the offered program with the patient's needs. 1 Traditional rehabilitation programs are typically far from the patient's residence, are offered on fixed days and hours, contain the same activities for everyone, and are done in groups, which can all be barriers to participation in traditional rehabilitation programs.
Despite the effectiveness and safety of rehabilitation programs, the participation of elderly patients (defined as >65 years old) is significantly lower than younger patients, even though elderly patients could greatly benefit from such programs. 2 –4 Moreover, in recent years, increasing numbers of Israel's elderly patients choose to remain in their homes and communities, assisted by the Long-Term Care Insurance Law and community health services. 5 This trend requires health and welfare services to seek alternatives for the traditional medical service. Such an alternative is the patient-centered approach (PCA), which focuses on the patient's needs and preferences. The goal of a PCA is to foster the independence of patients, including the elderly, and allow them to remain in their familiar surroundings while ensuring an acceptable quality of life. There is also a need to reduce public health expenditure, which is increasing alongside the increase in life expectancy. 5,6
The digital revolution has contributed greatly to home-based cardiac rehabilitation through programs that are accessible through smart phones, the internet, monitoring devices, and other utilities. These programs imply a high level of patient involvement in the treatment process and full cooperation between the patient and the caregiving staff. 7,8 Studies have shown that remote digital cardiac rehabilitation (RDCR) is equivalent to traditional cardiac rehabilitation in terms of achieving functional improvement, managing risk factors (blood pressure, lipid profile, body mass index, and smoking) and patient well-being, with no significant differences in mortality or hospitalizations rates. 2,9 Some studies have shown that the patient dropout rate was lower and the degree of responsiveness and perseverance was higher in home-based rehabilitation groups compared with traditional rehabilitation groups. 10
In recent years, the percentage of elderly individuals using technological tools has significantly increased. This population represents the principle consumers of most of digital health care services. According to the “Accenture consumer survey on patient engagement,” about 38% of people aged 65–74 used digital means to manage their health, compared with 22% of those aged 18–34. Health monitoring application use among older and younger populations increased from 16% and 9% in 2014 to 33% and 21% in 2016, respectively. Most consumers (78%) are using or willing to use technology to track their lifestyle or for medical surveillance. 11 Technology use among the elderly is affected by personal factors, such as attitudes, perceptions, and individual abilities. Environmental factors, such as a supportive environment, access to educational material, successful experiences with hardware and software, and ease and context of use all these play roles as well. Given the appropriate conditions and support, the elderly can benefit from the many health-promoting alternatives that technology offers. 12,13
The effectiveness and success of technologies in promoting health in general, and in the rehabilitation of cardiac patients in particular, depend on patients' attitudes toward the technological means. The aims of this study were to (1) examine attitudes, perceptions, and behavioral intentions of cardiac patients in general, and elderly patients in particular, to RDCR programs through technology tailored to the patient and (2) examine the extent to which promoting factors (education and physical activity habits) and inhibitory factors (technological illiteracy and smoking) affect willingness to participate in an RDCR program. Understanding the role of these factors will help policymakers to develop digital cardiac rehabilitation programs to improve the health and well-being of cardiac patients.
Materials and Methods
We conducted a cross-sectional study with a sample of 200 Hebrew-speaking patients >20 years of age who had recently experienced a cardiac event. Half were in a recuperation hotel immediately after hospitalization (n = 100) and the other half arrived at the rehabilitation center of the Sheba Medical Center, located in Ramat Gan, Israel about a month and a half after being discharged from the hospital (n = 100). There were 197 anonymous self-report questionnaires that were analyzed, as 3 were incorrectly completed and had to be excluded from the study. The study was approved by the ethical committee as required.
Measures
The research instrument employed was the Technology Usage Questionnaire, which was developed by Buys et al. 14 (see Supplementary Appendix 1). It includes 33 questions on the topics of (1) demography; (2) lifestyle (physical activity habits, alcohol consumption, and smoking); (3) reasons for referral to rehabilitation; (4) technological literacy and patterns of use of mobile phones, internet, computer, and monitoring devices; (5) interest to receive health content through mobile phone; and (6) interest to participate in a digital heart rehabilitation program and get telephone support. The questionnaire was translated to Hebrew and validated.
Mobile phone usage index
Expresses the sum of scores earned by answering questions that evaluate mobile phone use, for example, “What functions do you use on your mobile phone—calls/messages/camera” (0 = no, 1 = yes).
Technological literacy index
Expresses the sum of scores earned by answering questions that evaluate the knowledge and use of technologies, for example, “Do you have a mobile phone?,” “Do you have regular access to the Internet?,” “How often do you use the Internet?,” “Are you aware of computer based physical activity games?” What were the responses?
Physical activity
Expresses the frequency of participant's weekly physical activity. (Responses range from 1 = less than once a week to 5 = more than three times per week).
Attitudes toward healthy lifestyle management index
Expresses the mean of scores earned by ranking usefulness of various healthy lifestyle management proposals through mobile phone; for example, How useful would the following advice be?—Exercise ideas/Healthy meals ideas and recipes/How to overcome cigarette cravings/and more. (responses ranged from 1 = not useful at all to 5 = very useful).
Interest in telephone counseling from rehabilitation staff
Measured by responses to the question: “Would you be interested in receiving continuing advice on cardiac rehabilitation support via your mobile phone/smartphone?” (0 = no, 1 = yes).
Interest in RDCR
Measured by responses to the question: “If there were a free cardiac rehabilitation program by these types of communication would you sign up?” (0 = no, 1 = yes).
Demographic characteristics
Age, gender, level of education, employment, and residential area.
Statistical Analysis
Categorical variables were described using prevalence and relative prevalence. Continuous variables were described using group size, mean, standard deviation, minimum value, and maximum value. Differences between two groups of continuous variables were measured using the independent samples t test. Categorical variables were compared using a chi-square test. Ordinal variables were compared with the Mann–Whitney U test. The association between various continuous variables was analyzed using a Pearson correlation.
To explore independent predictors of willingness to participate in the RDCR program, a logistic regression model was constructed. The following covariates were included after a significant univariate association: age, education, Attitudes toward healthy lifestyle management index (ordinal covariate), and mobile phone usage patterns.
The significance level was determined according to a criterion of p < 0.05. Statistical analysis was performed using SPSS version 23 (IBM).
Results
Sample Characteristics
Men comprised 69% of the participants. Ages ranged from 20 to 91 years (mean 65 ± 11). More than half of the population was elderly (54.3%) and 94% owned a mobile phone. There were 88.3% of participants who had a high school education or higher. The most common reasons for hospitalization were coronary percutaneous interventions (54.9%), myocardial infarction (39.5%), and postcoronary artery bypass surgery (21.3%). A total of 58% reported that they engaged in physical activity more than twice a week, and 25.5% less than once a week (Table 1).
Baseline Characteristics of Patients
ICD, implantable cardioverter defibrillator; RDCR, remote digital cardiac rehabilitation; SE, standard error.
No significant differences were found between the two recruited groups (hotel/rehabilitation).
AGE, MOBILE PHONE USAGE PATTERNS, AND TECHNOLOGICAL LITERACY
Among elderly participants, mobile phones were predominantly used for calls (98%), messaging (69.4%), camera (69.4%), and video (57.1%). A significant negative correlation was found between age and technological literacy; the older the participants were, the less they knew about and used technology (r = −0.285, p < 0.01). The average Technological Literacy Index revealed a significant difference between the older and younger participants (10.42 and 12.51, respectively; p < 0.05) There was a significant difference between the young (84.1%) and elderly (59.2%) in daily internet use (p < 0.01). However, about 75% of the elderly reported that they used the internet at least three times a week. Findings indicated that only 5.2% of the elderly were familiar with exercise computer games compared with 23.2% of younger participants (p < 0.01). Only 11.7% of all participants [68.4% young compared with 31.6% elderly (p < 0.05)] used physical activity tracking devices (such as FitBit step trackers). Most participants (about 80%) in both age groups did not use heart rate monitors, with no difference between the groups.
Promoting and Inhibiting Factors to Rdcr
Total of 83% of all participants declared interest in an RDCR program. The type of cardiac disease condition was not associated with positive response, except in two cases: (1) patients after coronary bypass surgery were less likely to respond positively (71.1%), as opposed to 85.9% of patients who did not undergo surgery (p < 0.05) and (2) 100% of the patients with heart failure were interested in the program, compared with 80.8% of patients without a heart failure diagnosis (p < 0.05). There was no significant difference between young and elderly, between men and women, nor between the “hotel” and “rehabilitation” groups. No correlation was found between the promoting factors (physical activity habits and education) and the inhibiting factors (age, smoking, and technological literacy) and interest in the RDCR program. A comparison of lifestyles between older and younger participants showed that older patients were much more active—44.1% reported that they performed physical activity three times a week or more, compared with 28.7% of young patients; in addition, 53.8% of younger patients were physically active once a week or less, compared with 33.3% of the elderly population (p < 0.05). Smoking prevalence was greater among the young group as compared with the elderly (88.9% versus 11.1%, respectively; p < 0.001). No significant differences were found between men and women in education, technological literacy, or physical activity habits. Men smoked more than women (borderline significance: p = 0.056).
There was no significant difference in technological literacy among those who expressed an interest in the RDCR program and those who did not. Different age groups expressed a similar interest in participating in the RDCR program: 81% of those aged 20–40, 83.6% of those aged 60–80, and 66.7% of those aged 80–100. Our regression analysis did not show a significant association between baseline characteristics and declared interest in the RDCR program. However, significant differences were found among the age groups regarding proposals related to the healthy lifestyle management through mobile phone, such as virtual physical activity, goal setting, and medication taking. A higher percentage of patients aged 20–40 expressed an interest in these proposals (p < 0.05) compared with patients aged 40–80 and 80–100 (Fig. 1).
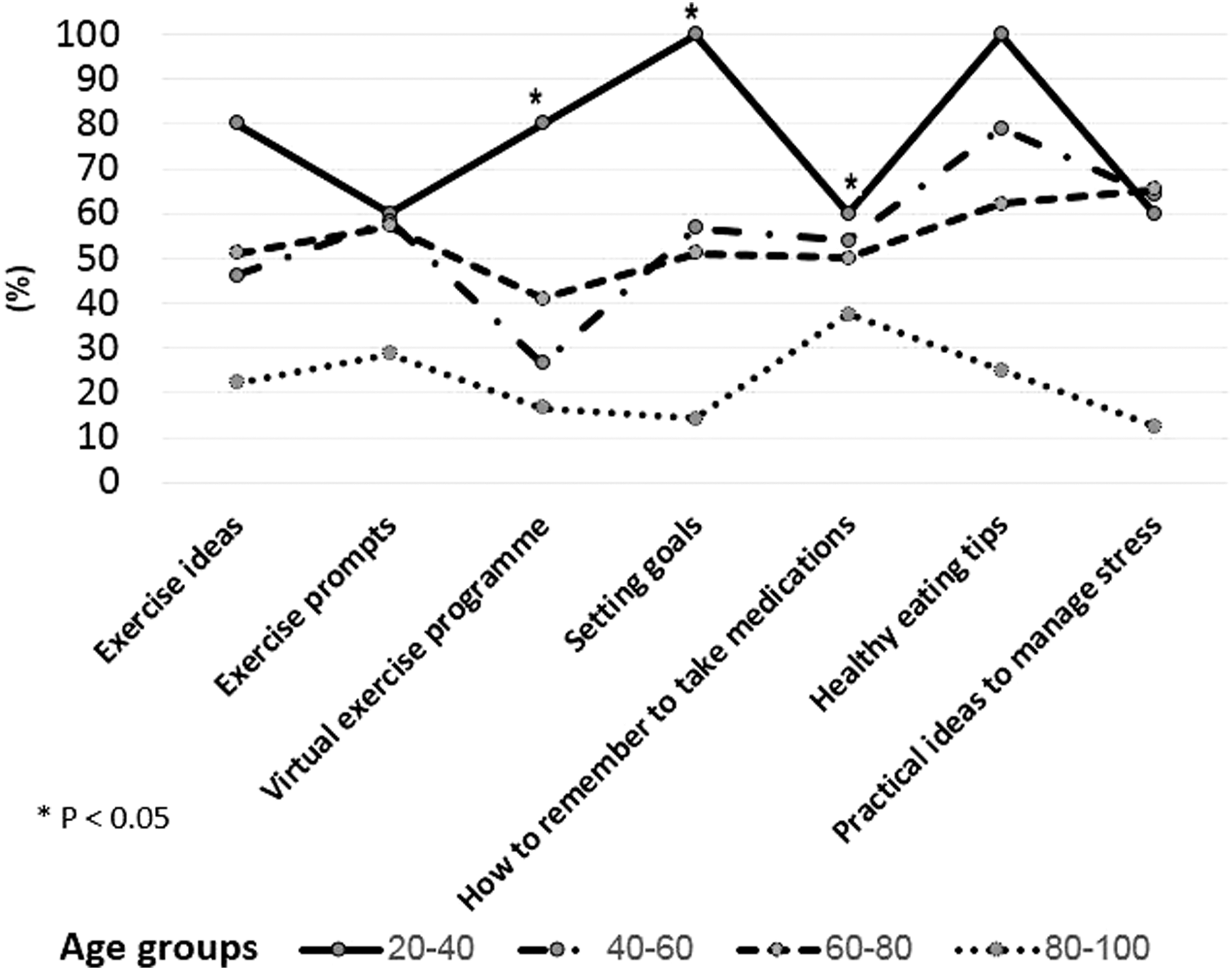
Relation between age and attitudes toward healthy lifestyle management. The figure shows that younger patients expressed more interest in healthy lifestyle proposals.
Age and Responsiveness to Digital Rehabilitation Proposals
Responsiveness to various rehabilitation options indicated that 77.2% of all participants expressed an interest in supportive counseling from rehabilitation staff through mobile phone (Fig. 2). Most participants responded that their preferred communication channel for receiving supportive counseling was through text messaging (86%). Second most popular options were e-mail and video clips (40% each).
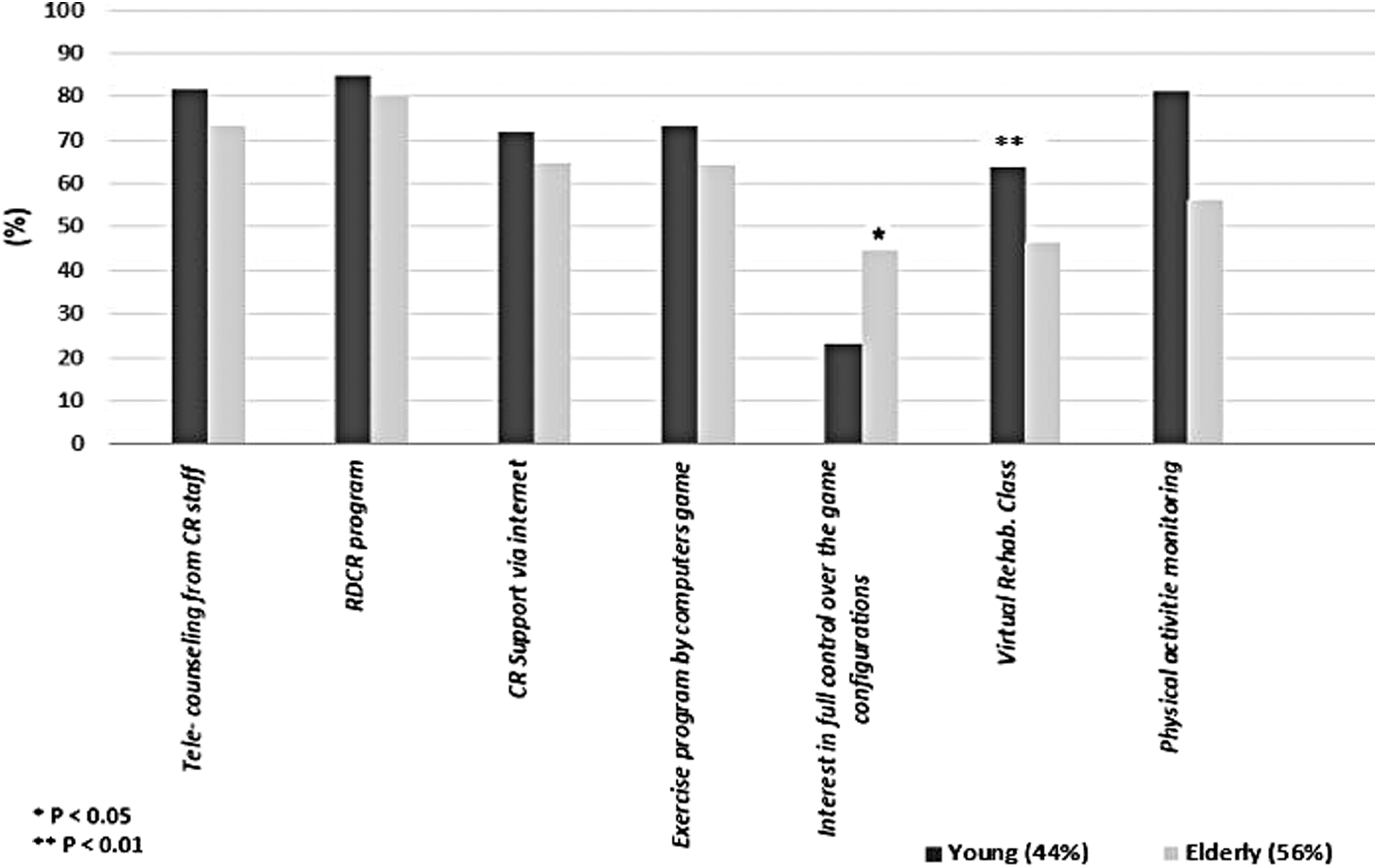
Acceptance rates of digital health intervention options stratified by age.
Half of those who agreed to participate in the RDCR program (41.5% [half of 83%]) wanted to receive up to two text messages a week, and 20% (16.6% [20% of 83%]) were interested in daily text messages. No significant differences were found on any of these parameters between age groups or between men and women. A total of 68.1% of all participants wanted to receive continuing cardiac rehabilitation support through the internet. Almost 60% of the participants wanted to try a virtual rehabilitation class.
In response to the question “How much interaction with such a game platform would you tolerate?” about 44.8% of the elderly indicated that they would be interested in full control over the computer game configuration, compared with 51.7% of younger participants who preferred only a few clicks to begin training (p < 0.05). About 68.1% of all participants expressed a desire to monitor their heart rate during exercise with a significant difference between the young (81.3%) and old (56.3%), and between men (72.5%) and women (54.8%) (p < 0.01) (Fig. 2). The average index of Attitudes toward healthy lifestyle management (Fig. 3) among younger participants was significantly higher (3.86) than that of the elderly (3.34) (p < 0.05).
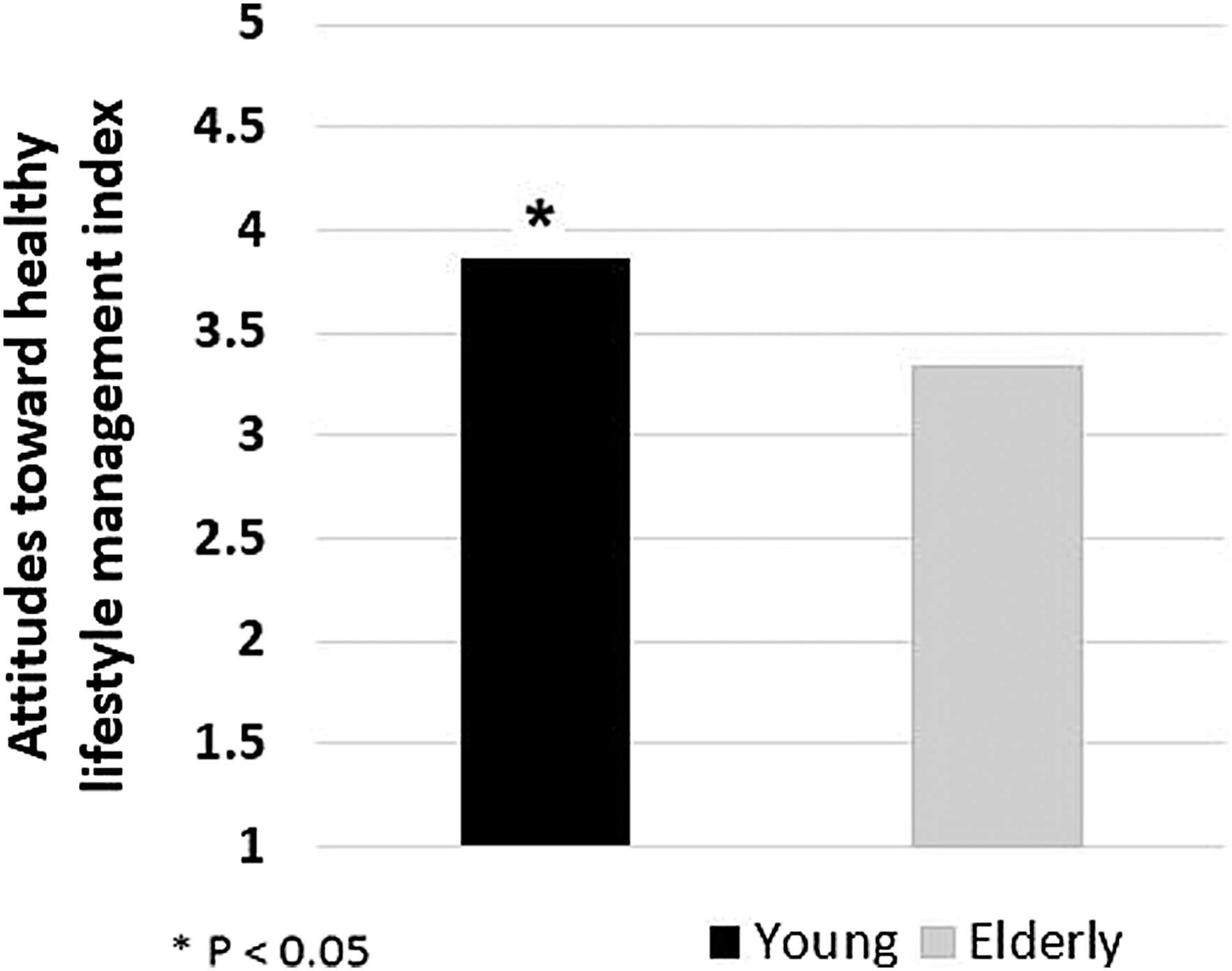
Attitudes toward healthy lifestyle management through mobile phone.
Attitudes Toward Health Counseling Through Mobile Phone
The mean rank of Attitudes toward healthy lifestyle management index among patients who were interested in the RDCR program was significantly higher compared with those who were not interested in the program: 80.99 (n = 125) versus 48.04 (n = 25), respectively (p = 0.001).
In addition, the mean rank of the same index was significantly higher among patients who were interested in telephone counseling by rehabilitation staff compared with those who were not: 82.88, n = 124 versus 61.53, n = 32, respectively; p < 0.05 (Fig. 4).
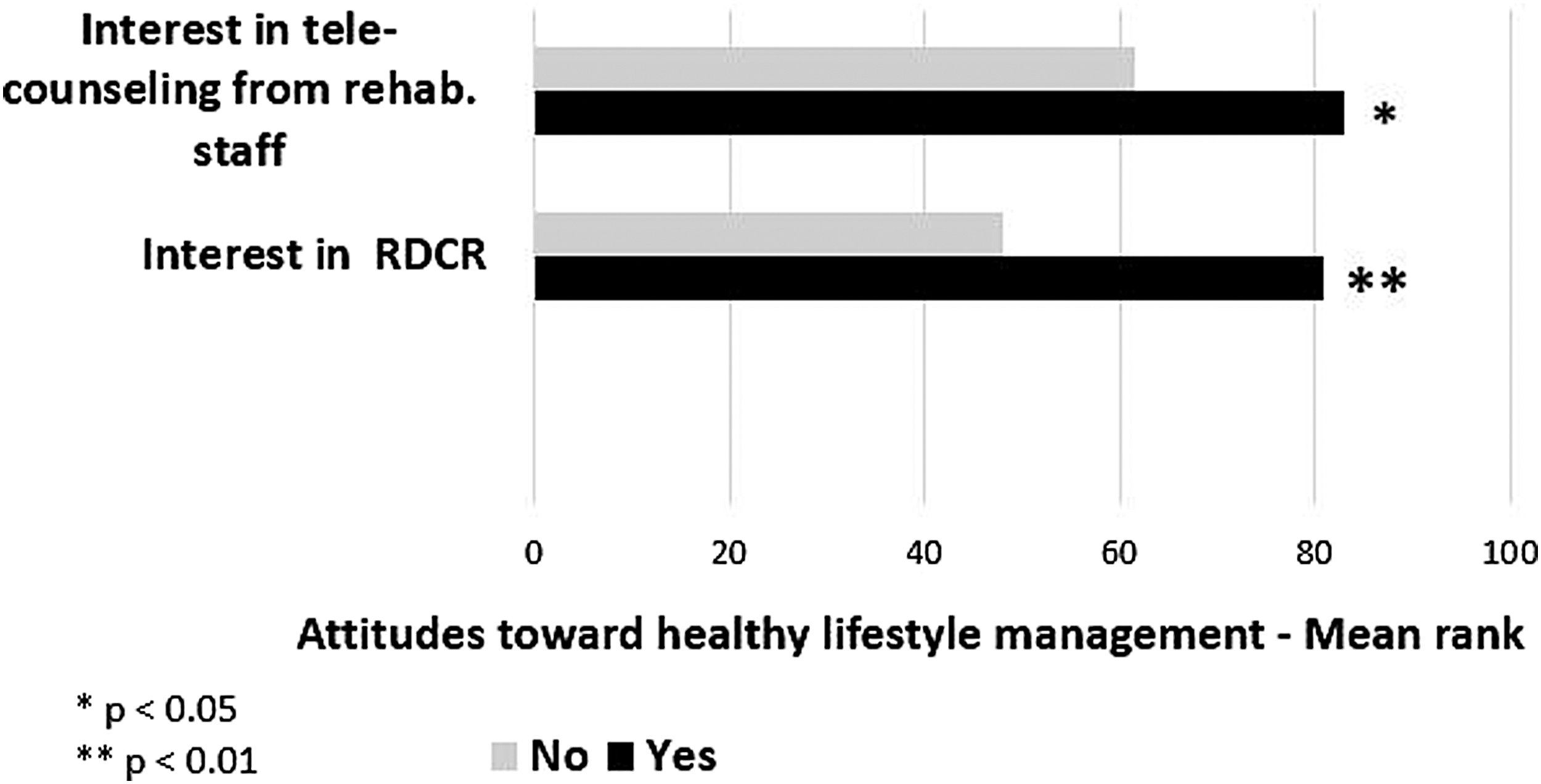
Relation between interest in the RDCR program and attitudes toward healthy lifestyle management. RDCR, remote digital cardiac rehabilitation.
We performed a logistic regression analysis for the responses to the question “If there was a free cardiac rehabilitation program by these types of communication would you sign up?” with the following variables: age, education, mobile phone usage patterns, Technological literacy index, and Attitudes toward healthy lifestyle management index. The only significant predictor of a positive response (meaning that participants would sign up for RDCR) was a higher attitude toward healthy lifestyle index, with odds ratio = 2.26 (p = 0.01) (Fig. 4). Most patients indicated that suggestions for healthy nutrition (66.4%), physical activity guidelines (59.6%), and coping with stress (56%) were “useful” or “very useful.”
Discussion
We conclude that cardiac patients in Israel, regardless of gender, age, lifestyle, education, technological literacy, or medical diagnosis, had a positive attitude toward the RDCR program with use of advanced digital technologies and are willing to participate in such programs if made widely available. Moreover, patients were open to various rehabilitation programs that used various digital means. This finding is consistent with the existing research. 15
Some explanations for the positive attitude may be due to the increasing use of technology as an accepted social norm in Israel, 16 the increasing use of digital devices in health care, and the expected benefits of the program; RDCR acting as a program that resolved various barriers that had prevented participation in traditional rehabilitation programs. 4
Digital communication suggests numerous communication channels, which makes it accessible to most cardiac patients of all ages. In our study, patients >65 years of age used mobile phones extensively for making phone calls, watching videos, and using the internet. This conclusion is consistent with OECD data, showing that in Europe, between 91% and 50% of the population aged 16–74 uses the internet on a daily basis. 17 Our data also showed that technological literacy declined with age. This finding is consistent with previous studies, which found that older people tend to use technologies less because of an objective decline in functioning, decreased social involvement, fear of learning new technology, and lack of practice and successful experiences that reinforce self-confidence and continued use. 13,18 –21 In addition, this study indicated that elderly people are less likely than young to use the internet, computer games, and digital devices to monitor physical activity. Hence, insufficient technological literacy and lack of previous experience with the technologies listed earlier may be a limitation for cardiac patients, especially the older ones, to participate in the RDCR program.
Patients who were interested in the RDCR program also had a greater interest in healthy lifestyle management through mobile phone. Text messages have been found to be a very efficient communication channel in health information of chronic patients. 22 –24 We also found that most patients preferred text messages as a communication medium for rehabilitation. Participants <65 years of age expressed more interest than the elderly population in healthy lifestyle management applications. As studies show, the elderly population is concerned about their ability to deal with the required technology, which may explain our findings. 21,23,24 Nevertheless, according Ines Frederix, 25 >70% of elderly population use technological means for health information searching. Therefore, we assumed that healthy lifestyles promotion by technological means may also increase responsiveness to cardiac rehabilitation. Studies show that most cardiac patients do not get sufficient health education and have poor health literacy. We found that cardiac patients expressed interest in subjects such as nutrition, physical activity, and mental well-being, which is in line with other studies. 15 Integration of these topics into health applications will encourage the usage of the applications and gain the awareness of living healthy lifestyle.
Digital means address patients' growing demand to be active actors in the treatment process, to receive complete information from the therapists, to monitor physiological processes in their bodies, and to manage their health. 11,15 In the cardiac rehabilitation domain, digital means are enablers of home rehabilitation programs and provide a solution for many patients who refrain from traditional rehabilitation. 7 By adopting the conclusions of this study and expanding the use of technological means, the health system would be able to promote health services for the general population and the chronically ill patient. RDCR programs are the future of the cardiorehabilitation domain. Such programs implement a “patient-centered” approach that allows treatment personalization and makes the patient an active actor in the treatment process. Development of such programs should consider the technological limitations of the elderly population and focus on convenient, easy to use, and attractive applications for patients of any age. RDCR programs shall also include health promotion content to balance the risk factors. Further studies are needed to examine various methods of digital rehabilitation and their adaptation to the needs of the patient.
Limitations of the Study
The study had several limitations. First, the study was undertaken at only one medical center in the center of the country, which excluded participation of patients who did not live near rehabilitation centers. Second, for reasons of convenience, data were collected at the hospital's hotel and rehabilitation center, which only some of discharged patients attended (30–50%) despite it being free of charge. In addition, the sociodemographic characteristics of the sample, residential location, level of education, and socioeconomic level may not adequately reflect Israel's entire cardiac patient population. Finally, the study is based on a self-report survey, which can also lead to bias.
Footnotes
Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Appendix 1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.