
Abstract
Background:
Telephone-administered cognitive-behavioral psychotherapy (T-CBT) can effectively treat patients with depressive symptoms.
Introduction:
We investigated whether adding letters (via postal mail) to T-CBT reduces depressive symptoms and increases response and remission. Additionally, we assessed whether T-CBT reduced all patients' symptoms in the first depression-specific T-CBT sample in German healthcare.
Materials and Methods:
Primary care patients were randomized to T-CBT with versus without letters. All received 1 face-to-face and 8–12 telephone-administered sessions. An intention-to-treat sample was analyzed. Between-groups differences in symptom change and the total sample's symptom change were computed using linear mixed models with group as fixed effect, referring general practice as random effect and several covariates. Differences in response and remission were assessed using logistic regressions.
Results:
Fifty-nine patients were referred to T-CBT and randomized. Twenty-six patients actually participated in T-CBT with letters and 21 without letters. The groups did not differ significantly regarding symptom change (Patient Health Questionnaire [PHQ-9]) from baseline to end: T-CBT without letters showed 1.05 points greater reduction (95% confidence interval: −4.72 to 2.62; p = 0.56; Cohen's d = −0.12) (adjusted mean change). The groups did not differ significantly regarding symptom change from baseline to 6-month follow-up nor odds of response or remission. The total sample's PHQ-9 showed significant adjusted mean reduction from baseline to end of T-CBT and to 6-month follow-up.
Discussion:
Additional letters did not lead to greater symptom reduction. Overall results for the first German T-CBT intervention for depression appear promising but require further assessment using a control condition.
Conclusions:
Additional letters do not appear to enhance the effectiveness of T-CBT.
Introduction
Depression is one of the most common and debilitating mental disorders. 1 A large proportion of depressed patients do not receive adequate treatment due to barriers on individual, care provider, or system level. 2,3 Low-intensity psychotherapeutic interventions, for example, bibliotherapy, 4 online treatment, 5 or telephone-administered psychotherapy 6 can help overcome barriers. Meta-analyses demonstrate that telephone-administered psychotherapy reduces depressive symptoms significantly compared to control conditions. 6,7 A large randomized controlled trial (RCT) found telephone-administered cognitive-behavioral psychotherapy (T-CBT) to be equally effective as face-to-face CBT. 8
Process characteristics in T-CBT have seldom been examined. Given that T-CBT is usually delivered as a structured short-term intervention with limited therapist contact, its effectiveness may be enhanced by additional letters. Reviews found text-based messages to significantly improve health behavior, for example, exercising. 9,10 Frequent and tailored messages involving some therapist contact were most effective. 9 Messages delivered via cell phone are becoming potentially valuable adjuncts to face-to-face CBT, for example, as homework reminders that enhance adherence. 11 In the original U.S. version of our T-CBT intervention 12 tailored letters containing personal feedback, encouragement, and reminders about tasks were mailed to patients after each T-CBT-session. 13 To our knowledge, no RCT has investigated whether such letters actually provide added benefit to T-CBT.
This study aimed to compare the effectiveness of T-CBT with versus without letters. This was the first assessment of T-CBT within a German sample of primary care patients with depression. The following research questions were addressed: Does T-CBT with letters lead to stronger symptom reduction from beginning (T0) to end of T-CBT (T1) than T-CBT without letters? (primary question) Does T-CBT with letters lead to stronger symptom reduction from T0 to 6-month follow-up (T2) than without? Does T-CBT with letters lead to greater response (from T0 to T1 and T2) and remission (at T1 and T2) of depressive symptoms than without? Does the T-CBT intervention significantly reduce depressive symptoms for the entire sample from T0 to T1 and T2?
Materials and Methods
Study Design and Setting
This was an RCT with parallel groups and no blinding, in which depressed primary care patients were assessed in a prospective multiple time point study from T0 to T2. It was conducted in Hamburg, Germany and registered with ClinicalTrials.gov, number NCT01770990. It was approved by the Ethics Committee of the Hamburg Chamber of Physicians and conducted according to the principles of the Declaration of Helsinki (2013 version).
This T-CBT study analyzed a subgroup of patients from the intervention group of the larger Hamburg stepped and collaborative care study “psychenet–Health Network Depression,” a cluster-randomized controlled intervention trial of a consecutive sample of depressed patients from primary care. 14,15
Participants and Recruitment
Inclusion criteria for the larger study were age >18, Patient Health Questionnaire (PHQ-9) ≥5, written informed consent, and German language knowledge. 15 Patients were assessed for eligibility for T-CBT by their general practitioner (GP), who could offer a referral to patients with an ICD-10 diagnosis of mild or moderate depression currently not receiving psychotherapy. Patients with more severe depression were also permitted to participate in certain situations, for example, if their mobility was limited.
Randomization
Patients were randomized to equal parts (1:1) into two parallel groups receiving T-CBT with or without letters. Randomization was performed by an independent statistician via computer program. Although assessment of eligibility was performed by the referring GPs, the diagnostic assessment by the psychotherapists afterward showed that some misallocations had taken place and several patients needed to be excluded from T-CBT after randomization and referred into more intensive treatments due to suicidality, post-traumatic stress disorders, or too severe depressive symptoms.
Intervention
The T-CBT-program is the translated and adapted German version 16 of “Finding a balance,” 12,13 comprising 1 initial face-to-face session and 8–12 weekly or bi-weekly ∼30-min T-CBT-sessions. The manualized treatment was performed by licensed CBT-psychotherapists with special training and supervision. Face-to-face, therapists performed diagnostics, introduced the program, and elaborated emergency care plans. An extensive patient workbook including homework was used between sessions. The program focused on psycho-education, behavioral activation, cognitive restructuring, and relapse prevention. 16
The Patient Health Questionnaire depression module PHQ-917 monitored depression severity at T0, T1, and at the fourth and eighth T-CBT-sessions. If the PHQ-9-score was <5 at the eighth session, 2 booster sessions were offered. If it remained ≥5 points when terminating T-CBT, referral into more intensive treatment was facilitated. In T-CBT with letters, patients received tailored one-page letters from the therapist by mail after each T-CBT-session, including a summary of the topics discussed in the previous session, a reminder of current homework, and motivational messages.
Outcome Assessment
Depressive symptoms were assessed using the PHQ-9. 17 Patient-rated therapeutic alliance quality was assessed with the “collaboration or bonding” subscale of the Helping Alliance Questionnaire (HAQ). 18,19 Data on simultaneous antidepressant treatment were extracted from care providers' forms and/or patient questionnaires from the larger study. Data on utilization of higher-intensity treatments after T-CBT were extracted from patient questionnaires for T-CBT at T2 or, if missing, care providers' forms and patient questionnaires from the larger study.
Statistical Analyses
All analyses used the intention-to-treat (ITT) population. Missing values were imputed via last-observation carried forward. Dropout was defined as completing <8 T-CBT-sessions. We statistically compared groups regarding sociodemographic and treatment characteristics using linear mixed models and logistic regressions.
Research question 1: A linear mixed model was calculated with group as fixed effect and referring GP practice as random effect, controlling for baseline PHQ-9, baseline HAQ, duration of T-CBT, and antidepressant treatment.
Research question 2: A linear mixed model was calculated with group as fixed effect and GP practice as random effect, controlling for baseline PHQ-9, baseline HAQ, duration of T-CBT, antidepressant treatment, and utilization of higher-intensity treatments after T-CBT.
Research question 3: Response was defined as PHQ-9-change of ≥50% from T0 to T1 or T2, respectively. Remission was defined as PHQ-9-score <5 at T1 or T2. Logistic regressions assessed between-groups differences.
Research question 4: A linear mixed model was computed with time as fixed effect and GP practice as random effect, controlling for baseline HAQ, duration of T-CBT, antidepressant treatment, and further treatments.
For all analyses, a significance level of p = 0.05 was determined and SPSS 21 was used.
Results
Patient Inclusion
Fifty-nine (n = 59) patients participated in the face-to-face session (Fig. 1). Of these, 31 patients were randomized to T-CBT with letters and 28 to T-CBT without.
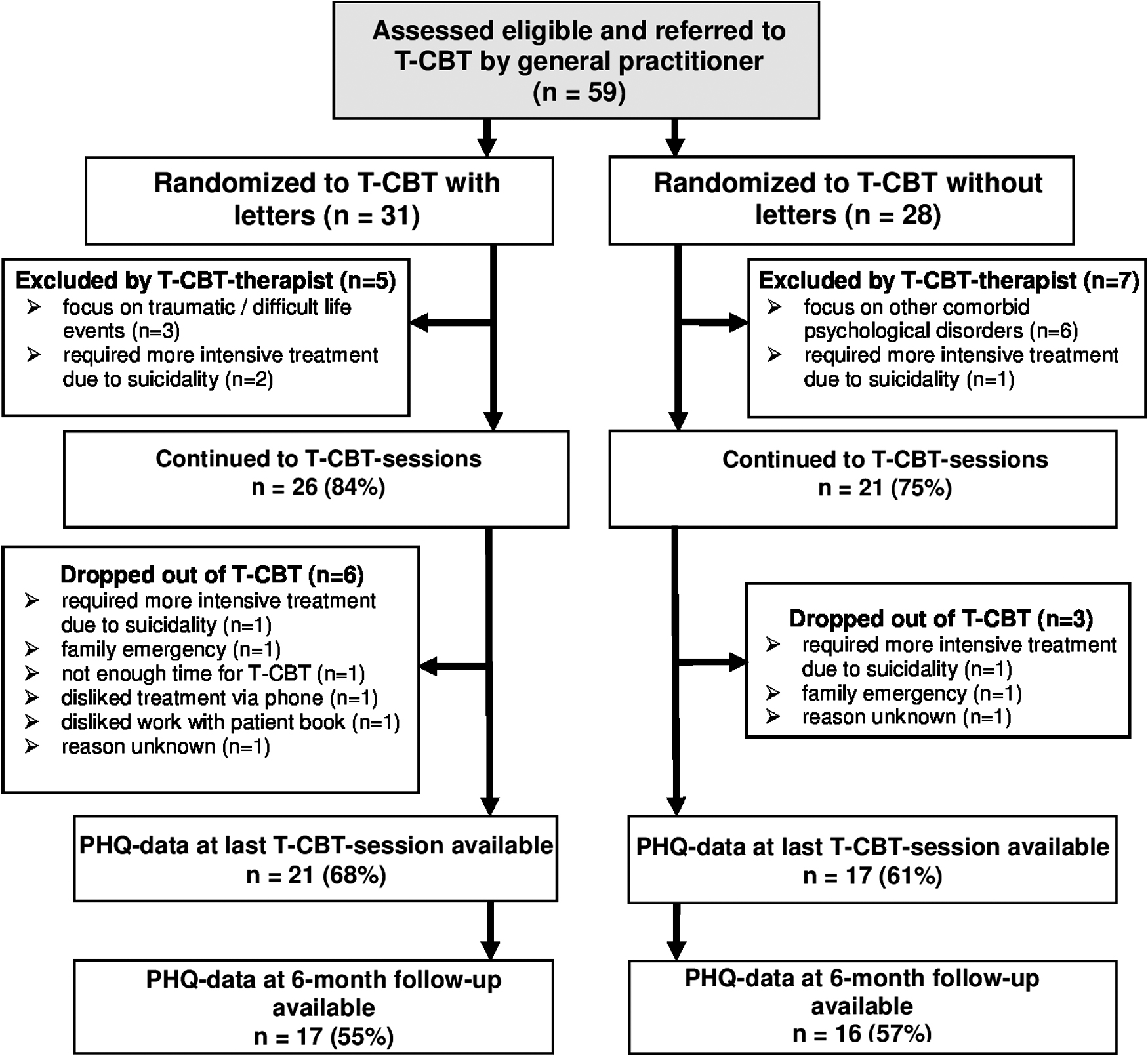
Patient flow from assessment of eligibility to 6-month follow-up.
In T-CBT with letters, five patients (16%) were excluded by the psychotherapist. Thus, 26 (84%) could continue with T-CBT. Of these, one dropped out before receiving any T-CBT-sessions and five (19%) dropped out before completing eight sessions (sessions completed until dropout: mean = 2.5 sessions; standard deviation [SD] = 2.2 sessions).
In T-CBT without letters, seven patients (25%) were excluded by the psychotherapist. Thus, 21 patients (75%) continued. Of these, three (14%) dropped out before completing the eighth T-CBT-session (sessions completed until dropout: mean = 5.3 sessions; SD = 1.5 sessions). The proportion of patients with missing PHQ-9 data was comparable between groups.
Sample and Treatment Characteristics
The groups did not differ significantly regarding baseline patient characteristics or treatment aspects (Table 1). Both showed a mild to moderate mean baseline depression severity and a very positive baseline therapeutic alliance quality (HAQ of ∼30 of 36 possible points).
Sample and Treatment Characteristics of Patients in Telephone-Administered Cognitive-Behavioral Psychotherapy with and without Letters (Intention-to-Treat; n = 47) and Assessment of Between-Groups Differences
Total nos. may vary due to missing values on some variables.
CI, confidence interval; HAQ, Helping Alliance Questionnaire; ITT, intention-to-treat; PHQ-9, Patient Health Questionnaire; OR, odds ratio; SD, standard deviation; T-CBT, telephone-administered cognitive-behavioral psychotherapy.
Research question 1 (primary outcome): Adjusted PHQ-9 mean reduction from T0 to T1 was not significantly higher in T-CBT with letters (Table 2). T-CBT without letters showed 1.05 points greater reduction, but this difference was not significant (95% confidence interval [CI]: −4.72 to 2.62; p = 0.56; Cohen's d = −0.12). An intra-cluster correlation of 0.052 was found, meaning that 5.2% of variation can be attributed to referring GP practices.
Research question 2: Adjusted PHQ-9 mean reduction from T0 to T2 was not significantly higher in T-CBT with letters (Table 2). Patients in T-CBT without letters showed 0.19 points greater reduction, a difference that was not significant (95% CI: −2.39 to 2.01; p = 0.86; Cohen's d = −0.03).
Research question 3: The odds of response did not differ significantly between groups from T0 to T1 (odds ratio [OR]: 0.92; 95% CI: 0.26–3.32; p = 0.90) nor from T0 to T2 (OR: 0.74; 95% CI: 0.21–2.58; p = 0.63) (Table 2). In the total ITT-sample, 27.7% of patients responded at T1 and 29.8% at T2.
The odds of remission did not differ significantly between groups from T0 to T1 (OR: 1.89; 95% CI: 0.48–7.44; p = 0.36) nor from T0 to T2 (OR: 1.28; 95% CI: 0.31–5.28; p = 0.74). In the total ITT-sample, 25.5% remitted at T1 and 21.3% at T2.
Research question 4: For the total sample, PHQ-9 showed a significant adjusted mean reduction of 1.95 points (95% CI: −3.39 to −0.52; p = 0.01; Cohen's d = 0.25) from T0 to T1 and of 3.26 points (95% CI: −3.39 to −0.52; p ≤ 0.001; Cohen's d = 0.42) from T0 to T2 (Table 3).
Discussion
This study investigated whether adding letters to T-CBT reduces depressive symptoms and increases response and remission in depressed patients. Both groups showed comparable sociodemographic and treatment characteristics. No significant differences regarding change in depression severity, remission, or response were found. These null results are not in line with a meta-analysis demonstrating the effectiveness of written messages. 9 However, most results were obtained within low-intensity interventions mainly using online tools and little or no counselor interaction. Possibly, our T-CBT program was already motivating and comprehensive enough not to require additional components. It is also possible that the delivery format used was not optimal. Systematic reviews 9,11 mainly included findings on messages delivered by email, text message, or telephone—perhaps our messages could achieve better results if delivered through one of these modalities.
Difference in Change in Patient Health Questionnaire Scores, and Response and Remission on Patient Health Questionnaire (from Beginning to End of Telephone-Administered Cognitive-Behavioral Psychotherapy (T-CBT) and from Beginning to 6-Month Follow-up (Intention-to-Treat; n = 47).
CI, confidence interval; LOCF, last observation carried forward; PHQ-9, Patient Health Questionnaire; SD, standard deviation; T-CBT, telephone-administered cognitive-behavioral psychotherapy.
Change in PHQ-9 Scores from T0 to T1 and to T2, and from T1 to T2 for the Total Sample (Intention-to-Treat; n = 47)
CI, confidence interval; PHQ-9, Patient Health Questionnaire; SD, standard deviation; T-CBT, telephone-administered cognitive-behavioral psychotherapy.
We found significant symptom severity reduction for the total T-CBT sample. These results appear robust, controlling for cluster effects and therapeutic alliance, duration, antidepressant medication, and further treatment utilization, none of which were significantly related to outcome. Thus, the T-CBT intervention as a whole showed promising results in a first depression-specific German sample. However, this should be interpreted with caution due to small sample and effect sizes and lack of untreated control group. The remission rate of 25.5% in our total sample at T1 was comparable with a large T-CBT study 8 (27%), as was our remission rate of 21.3% at T2 (19%). Our response rate of 27.2% at T1 was notably lower than theirs 8 (44%), perhaps because our patients received lower doses (1 face-to-face and ≤12 30-min sessions) than theirs, who received 18 45-min sessions.
Our study took place within a stepped and collaborative care model, a setting reflected by the relatively high proportion of T-CBT-patients using further, more intensive treatments after terminating T-CBT. While somewhat more than half of the patients did not require further treatment, this intervention may not have been sufficient for a relevant proportion of patients. Case examples from our study 16 reflect these different pathways. A greater amount or duration of sessions might also enhance our program's effectiveness.
Conclusion
This study did not demonstrate any benefit of adding letters to T-CBT. However, it showed promising first results for depression-specific German-language T-CBT, requiring replication in larger RCTs.
Footnotes
Acknowledgments
The study was funded within the larger project psychenet–The Hamburg Network for Mental Health. psychenet is a project network funded by the German Federal Ministry of Education and Research (grant no. 01KQ1002B) in the region of Hamburg that consists of more than 80 scientific and medical institutions, counseling centers, the Senate and the Chamber of Commerce of the Free and Hanseatic City of Hamburg, companies, as well as patients' and relatives' associations (2011–2015). The vision of the project is to promote mental health today and in the future, concerning early diagnosis and effective treatment of mental illnesses (
Disclosure Statement
No competing financial interests exist.