
Abstract
Proven capacity to enable both valid diagnostic decisions and effective management decisions should be required before health care innovations are adopted in routine practice. Various care models, although distinct in capacity for information acquisition and status of effectiveness and efficiency assessment, are marketed as telemedicine. Ability to meet criteria of effective and efficient decision making depends heavily on both the type of clinical problem at hand and the diagnostic and communication tools included in the telemedicine model. As an example of a problem-type-specific, connected care model supported by a well-developed evidence base, we review research findings that support widespread implementation of a model for primary care pediatrics. But, as an understanding of disruptive innovations would predict and as our experience has shown, such evidence is not sufficient by itself to ensure adoption and dissemination. Disruptive innovations are “cheaper, simpler, more convenient products and services that start by meeting the needs of less demanding customers.” Such innovations threaten the value of existing services and organizations offering them. Consequently, dominant provider organizations positioned to develop telemedicine, but with important revenue streams threatened by telemedicine, anticipate negative financial impact. Accordingly, these organizations typically obstruct the adoption of disruptive innovations, or are at least slow to adopt them. Organizations funding health services research, investigators, provider organizations, individual providers, and payers, all share responsibility for developing the evidence base supporting connected care. For models supported by a solid evidence base, the challenge extends to ensuring widespread availability of this useful service.
Introduction
Merrill and Doarn extend a challenge for “vetting of telemedicine practices in terms of overall impact on health, human resource conservation, costs and perceptions.” 1 Evidence of effectiveness, efficiency and acceptability should be the basis for any innovation in clinical practice. Before this challenge can be met, 2 fundamental questions must be addressed. (1) What do we mean by telemedicine? (2) What type of clinical challenges do we plan to address? We consider these issues in this article. In addition, we contend that vetting effectiveness and efficiency is not sufficient to ensure improvement in population health or decrease direct or indirect costs.
Care Model Potential Depends on Capacity for Information Acquisition
In addressing the challenge, we accept the ideal of medicine as an evidence-based endeavor. Type of problem addressed determines information required to enable accurate diagnosis and effective management. Capacity for examining the middle ear, for example, is essential for evaluation of a large proportion of illness episodes in young children. A telemedicine model without capacity for cerumen removal and tympanic membrane imaging cannot serve effectively. In contrast, for evaluation and management of common behavior issues such as attention-deficit/hyperactivity disorder, a model including only video and audio suffices. Once type of clinical problem is established, requirements for clinical information (e.g., history, physical examination, laboratory work) can be identified.
Our experience serving families and childcare and school personnel challenged by childhood illness includes over 13,000 telemedicine visits over 13 years. 2 Based on this experience and the logic of evidence-based decision making, it seems useful to characterize clinical problems as falling along a range of complexity in information required for effective care. 3 As illustrated in Figure 1, if one is to base decision making on solid evidence, capacity for information acquisition must meet the level of information quality and detail required by the patient's problem.
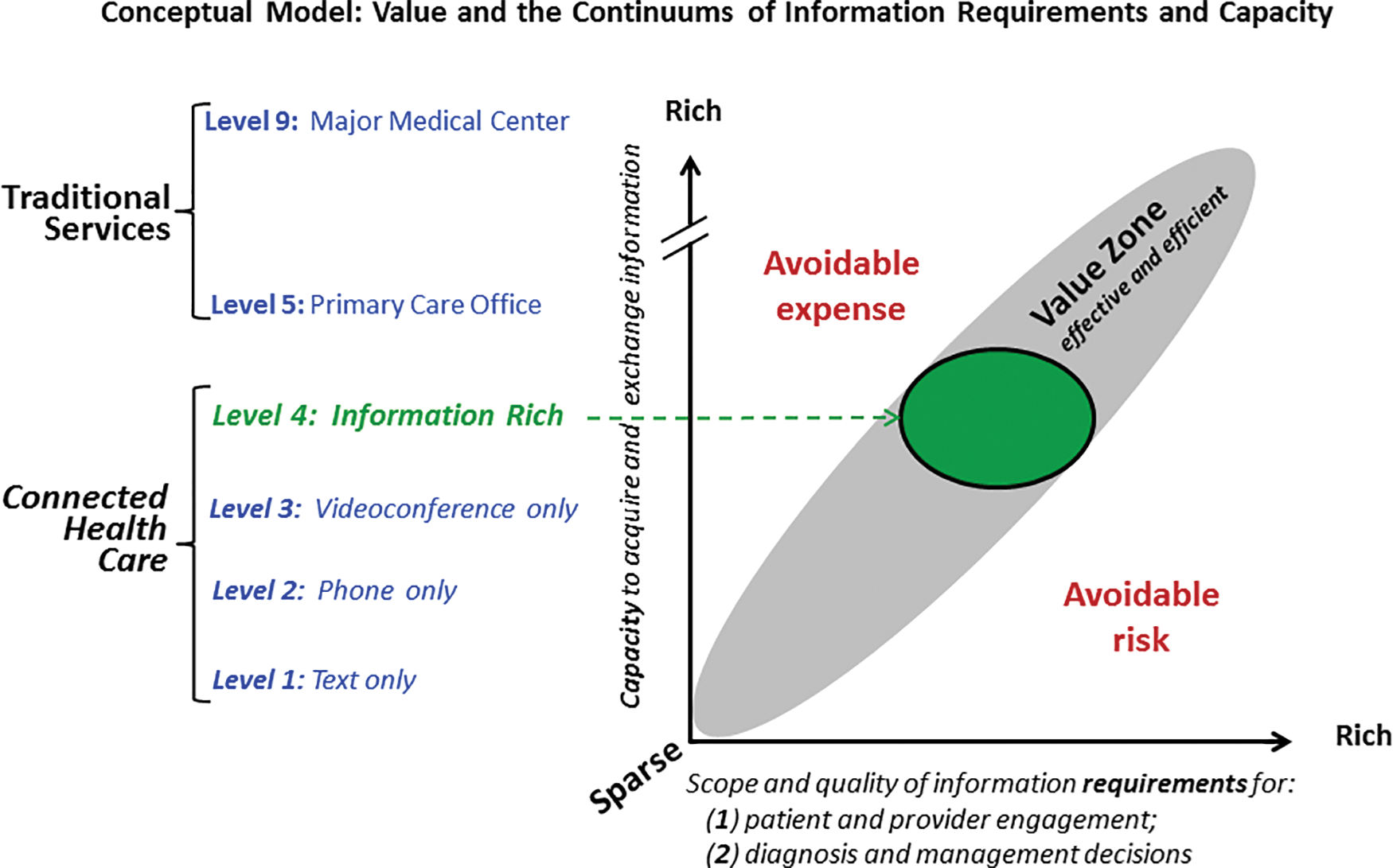
In this conceptual model, value is achieved when resources (currency, time, travel) allocated to the problem are sufficient, but do not exceed, those required to optimize outcome. When resources expended fall above that level, unnecessary and avoidable cost accrues. When resources expended fall below that level, unnecessary and avoidable risk is taken. The farther performance strays from the value zone, the greater the avoidable expense (if above it) or the greater the avoidable risk (if below it). If addressing a problem with rich information requirements for diagnosis and management (e.g., a febrile infant who actually has pyelonephritis) with technology of limited capacity (e.g., phone only), service falls out of the value zone and all stakeholders (child, family, provider, payer, community) incur substantial risk. The Value Zone is represented as an oval rather than a straight line to avoid the implication that the relationship between requirements and capacity is perfectly linear. Color image available online.
In addressing our challenge, it is important to recognize that information required for accurate diagnostic decisions and effective/efficient management decision making varies dramatically with the type of problem. In caring for a young child with fever, for example, fixed images, video, and audio clips may be important, respectively, for pharynx, tympanic membrane mobility, and lung evaluation. For a child with behavioral problems, real-time video interaction—among primary care provider, behavioral therapist, parent, child, and/or teacher—may be sufficient.
We wholeheartedly agree that evidence for effectiveness and efficiency should precede adoption of health care innovations. Evidence reviewed below meets these criteria for a well-defined, broad range of common problems encountered in pediatric primary care. This evidence base exemplifies the type of evaluation required before a clearly defined telemedicine model can be embraced as offering care at least equivalent to in-person care from patient and community perspectives.
Validation
We use the label, Health-e-Access (HeA), to distinguish the model we designed for care of children with illness symptoms. Evidence supports usefulness to all stakeholders through evaluation visits in 74 different access sites, 2 including childcare, school, child development centers, and neighborhood family service agencies. Among inner city childcare centers with telemedicine, absence due to illness dropped to 63%. 4 Among over 14,000 telemedicine visits from these sites, 97% were completed, that is, 3% are referred to a higher level of care. 3 Acceptance of HeA by parents, providers, and insurance organizations was confirmed by high levels of parent satisfaction with telemedicine, 5,6 participation in HeA by over 70 different providers from 10 primary care practices, 3 telemedicine access in all Rochester City Schools since September 2010, and reimbursement by all local payers at office visit rates. Continuity within medical home for visits by children with a participating practice averaged 83%. 3
Children with childcare or elementary school access made 22% fewer emergency department (ED) visits than closely matched counterparts. 4 The finding of ED visit reduction was based on observations during the first 5 years of HeA operation; accordingly, it probably underestimates the potential HeA impact because the years when reduction was observed included substantial periods when providers and parents were learning to use HeA and before evening telemedicine access was offered. Based on subsequent analysis for children with severe disabilities who attended a child development center, ED visits dropped 50% after telemedicine access became available. 7 Parents estimated ED visits avoided would have taken 4.5 h on average. 6
Evidence also suggests that telemedicine extends equity in access to impoverished, urban families. 8 Before HeA availability in childcare or school for an urban intervention group, suburban controls made 80% more acute illness visits overall. With HeA availability, this difference subsequently disappeared. For an urban control group, however, the urban–suburban disparity in access remained.
Potential for HeA to replace illness visits at less convenient and more costly access sites is substantial. Study in pediatric practice found that 85% of illness visits could be completed using the HeA model. 9 This percentage was based on judgments of experienced pediatricians seeing children in the traditional manner in a primary care practice. Potential to expand HeA broadly beyond its original focus on acute childhood illness is supported by evaluation of Rochester initiatives focused on school-based chronic care (especially asthma 10 ), dental screening, 11,12 and older adults in senior living communities. 13,14 Evaluation of a similar model in Sacramento, California demonstrated savings in time, travel, and environmental pollution. 15 A similar model is also used actively in North Carolina. 16
In sum, this model addresses incentives for all stakeholders in care of ill children—patients and families, providers, provider organizations, and payers. For patients and families, HeA equals or exceeds the convenience of alternatives such as urgent care centers or the ED. In addition, HeA enables care within the trusted primary care medical home (PCMH). HeA empowers PCMH providers on call to deliver office-equivalent care at any time without leaving their own home. HeA enables provider organizations to offer ready access within the PCMH through low-cost infrastructure, avoiding revenue loss to care sites (e.g., the ED, urgent care) outside the medical home. As provider organizations increasingly assume the responsibilities of accountable care organizations with various form of capitated financing (e.g., per-member per-month, bundled payment), they will be increasingly incentivized to adopt effective, low-cost acute care alternatives such as HeA. For payers within fee-for-service financing, HeA reduces expensive resource use, such as the ED, for nonemergency problems.
Vision
The HeA goal is to enable health care when and where you need it by providers you know and trust.
Community-wide access and medical home integration, core attributes congruent with this goal, enhance effectiveness and efficiency substantially. Integration within the PCMH promotes trust among patients and caretakers. Trust is especially salient when introducing families to an unfamiliar approach to care of loved ones. Continuity of care within the medical home leverages established relationships with providers, promotes medical record completeness, creates opportunities to offer preventive services (e.g., immunizations), reduces unnecessary testing, increases patient and provider satisfaction, and promotes efficient problem follow-up. With the internet enabling secure communication, clinical information (e.g., high-resolution images, video clips, stethoscope sounds) can be shared either synchronously (real-time interactive videoconferencing) or asynchronously (store-and-forward) across any distance.
One cannot gain the benefits of the medical home integration without community-wide access. Efficiency considerations require service in central locations conveniently accessible to many children, regardless of practice affiliation. Optimal access (when and where you need it) requires access at places such as childcare, school, and neighborhood pharmacies. Efficiency also requires that infrastructure—both technology and personnel—serve the entire community regardless of the patient's provider organization or payer affiliation.
Community wideness, electronic medical record interoperability patient-to-primary care provider design, and internet use, all contribute to potential network effects, defined in economics as the consequence that one additional user has on the value of a product to other users. 17 As with related communication technologies such as social networks, the usefulness of the HeA Telemedicine Model can be expected to conform to Metcalfe's law, holding that system value is proportional to the square of the number of users. 14 Network effects are small with a modest user base but become powerful once a critical mass of users is achieved. Consider the increase in value of your cellphone as the number of phone users grows beyond two.
The Challenge Inherent to Disruptive Innovations
It is appealing to think that research establishing effectiveness and efficiency from patient and community perspectives is sufficient to ensure widespread adoption of useful innovations. But that is not how things work for innovations that are also disruptive. Disruptive innovation, as defined by Christensen et al. 18 –20 are “cheaper, simpler, more convenient products and services that start by meeting the needs of less demanding customers.” With these attributes, innovations threaten the value of existing services and established companies. Consequently, established organizations with sufficient control over a particular type of product—sufficient control to substantially shape the terms on which individuals access it—obstruct its adoption. When less expensive, portable, low-intensity X-ray machines were invented, for example, suppliers and users of conventional large-scale X-ray equipment wanted nothing to do with them. Suppliers as well as hospitals and radiologists already had invested much in manufacture, purchase, and maintenance of conventional equipment. Similarly, physician groups resolutely resisted the introduction of nurse practitioners and physician assistants as professional colleagues, despite demonstration of competence both in management of a large proportion clinical encounters, and in accurately identifying problems possibly beyond their expertise and obtaining physician consultation regarding such problems.
Telemedicine in Primary Care Is a Disruptive Innovation
Large health care provider organizations allocate substantial resources to keeping services available that are capable of addressing dire emergencies. Such emergencies are not frequent enough to fully occupy these resources, so much time of ED personnel is spent on nonemergent problems. The vast majority of nonemergent problems could readily be addressed by a well-designed telemedicine model, that is, “cheaper, simpler, more convenient” services. Research findings on HeA demonstrate these efficiency attributes as well as clinical effectiveness.
Yet, in a health system in which fee-for-service reimbursement dominates funding, major provider organizations would jeopardize their financial status by large-scale adoption of primary care telemedicine. These organizations have a strong financial interest in keeping things busy in the ED, rather than siphoning off visits to telemedicine models designed for common acute problems, where visits are commonly reimbursed at about one-tenth the ED payment.
Organizations with sufficient influence to drive health services innovation have demonstrated little interest in adopting telemedicine for everyday primary care. In seeking to explain this lack of interest, one might start by asking what generally drives the adoption and dissemination of valuable innovations that disrupt important revenue streams, not just in health care, but in
While contemplating that question, the following aphorism came to mind; “When herding cats, move their food.” As long as fee-for-service financing continues to dominate health care, a strong financial incentive remains for large medical centers to maximize ED visits. The Accountable Care Act (ACA) attempts to “move the food” of these organizations. In moving health care funding away from fee-for-service reimbursement and toward capitation (fixed payment per covered life), the ACA attempts to shift provider organization incentives away from volume of highly paid services and toward quality of care. 21 Given that quality of care is more difficult to measure than number of visits, this objective represents a steep challenge in some types of medical practice. For problems dominating primary care practice, however, it should be noted that readily acquired metrics of patient convenience and satisfaction are meaningful and actionable. Most of acute problems seen in primary care are self-limited and readily addressed through telemedicine. Given what we know about herding cats, it would appear promising to establish insurance plans in which management of problems common in primary care were covered through capitation.
Large medical centers generally dominate the organization and delivery of health services in urban communities. With care for common acute problems covered under capitation, dominant organizations would achieve no financial advantage in caring for nonemergency problems in the ED. Rather, they would benefit by providing service “under the cap” in the manner least costly for them. The HeA model offers a powerful tool toward achieving that objective when combined with telephone triage.
Phone triage systems, available in many communities and based on well-validated phone management algorithms 22,23 currently help providers, patients, and parents decide what problems require emergency services, warrant office-based care, or can safely be managed at home. Among those warranting in-person but nonemergency care, our experience has shown that the vast majority can be well managed with an information-rich telemedicine model, as discussed.
Evidence for Effectiveness and Efficiency Is Not Sufficient to Ensure Adoption
Quite reasonably, Merrill and Doarn challenge us to provide evidence of telemedicine's effectiveness and efficiency. Effective care requires valid diagnostic decisions (i.e., high sensitivity and specificity) and implementation of useful interventions. To be more efficient, care must not only be effective; it must also cost less than alternative modes of delivery. In evaluation of efficiency, we advocate taking a societal perspective; considerations of value should include not only dollars expended, but also time lost from work and school, transportation costs, and distraction from other responsibilities due to anxiety.
Such an evidence base can only be provided through systematic accrual of evidence encompassing a broad range of applications. This takes time and treasure as well as rigorously designed and executed studies. Reliability and validity depend on precisely what information is required to address a particular clinical challenges effectively. Effectiveness includes accurate diagnosis and useful intervention. Information for meeting these requirements is determined by the type of problem. Type of problem in this context is based on similarity in information that must be acquired with physical examination tools or history. For an infant presenting with fever and irritability as problem type, distinguishing among common causes, such as upper respiratory tract infection, otitis media with effusion, acute otitis media, nonspecific viral syndrome, and possible serious bacterial infection (e.g., meningitis, sepsis, pneumonia) require all the components of the HeA Model described above. In contrast, effective care for teens with problems in school performance rests almost exclusively on history obtained from school personnel, parents, and the patient. Such history enables differentiation among depression, oppositional-defiant disorder, learning disabilities, and attention-deficit/hyperactivity disorder.
Conclusion
In summary, adoption of telemedicine should require compelling evidence that valid diagnostic and appropriate management decisions can be made. Decisions on use and on insurance coverage should require such evidence to be specific to the type of problem. Guidelines based on the judgment of expert clinician panels can be used to codify problem types as well as type of telemedicine model required to meet standards of accurate diagnosis and effective management. Such evidence-based guidelines are not sufficient, however, to ensure widespread adoption of telemedicine. This will not occur without financing mechanisms that encourage dominant provider organizations to do so. Our challenge, no less important than developing a solid evidence base, includes advocacy for financing that enables access through telemedicine.
Footnotes
Disclosure Statement
No competing financial interests exist.