
Abstract
Introduction:
Group therapeutic singing (GTS) may be an effective treatment for voice and respiratory impairments in persons with Parkinson's disease (PD). However, it remains unknown if GTS can be effectively delivered through telemedicine.
Methods:
Participants with PD from rural areas were recruited to complete a prerecorded GTS program, once a week for 8 weeks. Voice and respiratory outcome measures were collected 1 week before and 1 week after intervention.
Results:
Ten participants were enrolled in the study. One participant dropped at week 3. Five participants attended all eight sessions, two participants completed seven sessions, and one participant completed six sessions for 93.75% compliance. Statistical analysis for the data collected from the eight participants enrolled in the study revealed that voice outcome measures improved but did not reach significance. However, respiratory outcome measures significantly improved.
Discussion:
Results suggest that prerecorded GTS is feasible. Moreover, results are in keeping with results from a previous study using the exact same intervention with an in person therapist. Thus, this pilot work suggests that the use of prerecorded GTS may be a viable treatment option for those with limited access to care.
Introduction
Nearly 60–80% of persons with Parkinson's disease (PD) have voice impairments. 1 –3 Moreover, difficulties in breathing and airway protection are the primary factors leading to death in persons with PD. 4,5 Current pharmacological and surgical treatments do not fully address these impairments, and it is estimated that only 3% to 4% of persons with PD undergo speech therapy. 6 –8 This estimate is further minimized for those living in rural areas in which access to care is limited. There remains a need to develop and deliver new ancillary therapies to help improve voice and respiratory impairments in persons with PD, especially those in rural areas.
Telemedicine is a growing area that may address the needs of persons with PD in more rural areas. Research has shown that compared with in person visits, telemedicine provides similar care and reduces travel costs and travel times. 9,10 Telemedicine has mainly been used for the assessment and monitoring of disease progression in persons with PD. There is limited use in providing therapy. However, research has shown that telemedicine is effective for delivery of a cognitive-behavioral treatment for depression in PD, as well as for group therapy and education and support sessions. 11,12 Thus, telemedicine may have the potential to improve the accessibility of group interventions for those with PD living in rural environments.
Previous research has suggested that singing may be an effective treatment for voice and respiratory impairments in persons with PD. 13 –15 Singing is generally considered to be a more sustained form of speech requiring greater vocal control and increased respiratory control and muscle strength. 16 –19 Indeed, previous research from our team has shown that group therapeutic singing (GTS) is an effective treatment strategy to maintain the voice and significantly improve respiratory control in persons with PD. 20 However, it remains unknown if GTS can be effectively delivered through telemedicine, and if this type of delivery would produce similar results to in person GTS. Therefore, the purpose of this study was to determine if an 8-week prerecorded GTS program was feasible and effective for persons with PD living in rural areas. We hypothesized that prerecorded GTS would be feasible. Moreover, we hypothesized that the prerecorded GTS would be effective, producing results similar to our previous study using in person GTS: (1) voice outcome measures would be maintained and (2) respiratory control would significantly improve.
Methods
Recruitment
Participants were recruited from two rural areas in Iowa: Rockwell City (population 1,709 in 2010) and Storm Lake (population 10,600 in 2010). Various recruitment methods were used. A human sciences extension specialist (last author) through the University's Extension and Outreach program serving these regions met with local health care facilities, churches, and PD support group communities to discuss the study and provide fliers. Follow-up calls were completed to remind these contacts of the research study opportunity and encourage them to inform potential participants of the study. Interested participants were provided contact information of the principle investigator (first author) and asked to call or e-mail for more information.
Participants
All participants had a diagnosis of idiopathic PD, were on a stable regimen of antiparkinsonian medications for 30 days, were current nonsmokers, and had no speech therapy within 2 years before the study. Exclusion criteria included significant cognitive impairment (Mini-Mental State Examination score <24), major psychiatric disorder (Beck Depression Inventory score <18), history of head or neck cancer, asthma or Chronic Obstructive Pulmonary Disease, and untreated hypertension. A Unified Parkinson's Disease Rating Scale score was obtained for all participants by a researcher trained in the administration of the test. All participants gave written informed consent, and the study procedures were approved by the Iowa State University Institutional Review Board.
Prerecorded Program
Before recruitment and data collection, an 8-week program was filmed. The first author is a board-certified music therapist and leads weekly GTS sessions for persons with PD. Thus, this group served as the population for the video and the first author lead the recorded sessions. Each session followed the same protocol that was used in our previous study examining the effects of an in person 8-week GTS program. 20 All participants on the videos provided consent to be filmed. Delivery of the program was completed by a human sciences extension specialist (last author) through the University's Extension and Outreach program. The extension specialist met with each group weekly and was responsible for displaying the program and monitoring participation. Both groups met at a local church in their community that was equipped with a screen to project the program, and the extension officer provided the laptop with the electronic version (stored on the University's protected box file) of the program to be projected onto the screen.
Each session included a series of vocal exercises followed by group singing of familiar songs. The intervention specifically targeted breath support, vocal intensity, and fundamental frequency range. A complete description of the intervention has been provided in our earlier work. 20
Data Collection and Analysis
The research team traveled to each group location 1 week before the start of the intervention and 1 week after the intervention to complete pre- and post-assessments. All participants were tested on medication for both assessments, and both assessments were collected at the same time of day for each participant to avoid fluctuations in medication. The same outcome measures were collected for both the pre- and post-assessments using the same equipment and in the same location.
Voice outcome measures included phonation duration, phonation range, and vocal intensity. Three trials of each measure were collected. For phonation duration, the total time each participant sustained the vowel sounds “ah” and “ee” was recorded. For phonation range, the lowest and highest pitch was recorded using a Chromatic Tuner iPad application (Pano Tuner; Jung-gun Lim, version 1.2.10), and the difference between these values was calculated for vocal range. For vocal intensity, the loudest sound produced on a sustained “ah” was measured using a Decibel Meter iPad application (Dominic Watson, version 1.6).
Respiratory outcome measures included maximal inspiratory pressure (MIP) and maximum expiratory pressure (MEP) and were recorded using a portable respiratory pressure meter (CareFusion, San Diego, CA). Three trials that produced values within 5% of each other were obtained for both MIP and MEP. For MIP, breathed in through the tube as forcefully as possible for 2 s. For MEP, participants blew out through the tube as forcefully as possible for 2 s.
The mean and standard error were determined for each outcome measure. To determine the effectiveness of prerecorded GTS, a paired t-test was completed for each voice and respiratory outcome measure. Given that this is a pilot study, the significance was set at α = 0.1. 21 Cohen's d effect sizes were also determined.
Results
Feasibility
Recruitment was first initiated in Rockwell City. There was no PD support group around this region, making recruitment more challenging. Four potential participants made initial contact with the principle investigator, but only two remained interested and were subsequently enrolled in the study. To increase enrollment, recruitment was initiated in the Storm Lake region, as there was a well-established PD support group in the area. Ten participants made initial contact with the principle investigator. Two participants declined the study. Seven participants were enrolled in the study. In total, nine participants were enrolled in the study for an enrollment rate of 57.14%. One participant dropped before completing the study, leaving a completed data set for eight participants. See Figure 1 for the flow diagram of recruitment to enrollment and Table 1 for participant demographics.
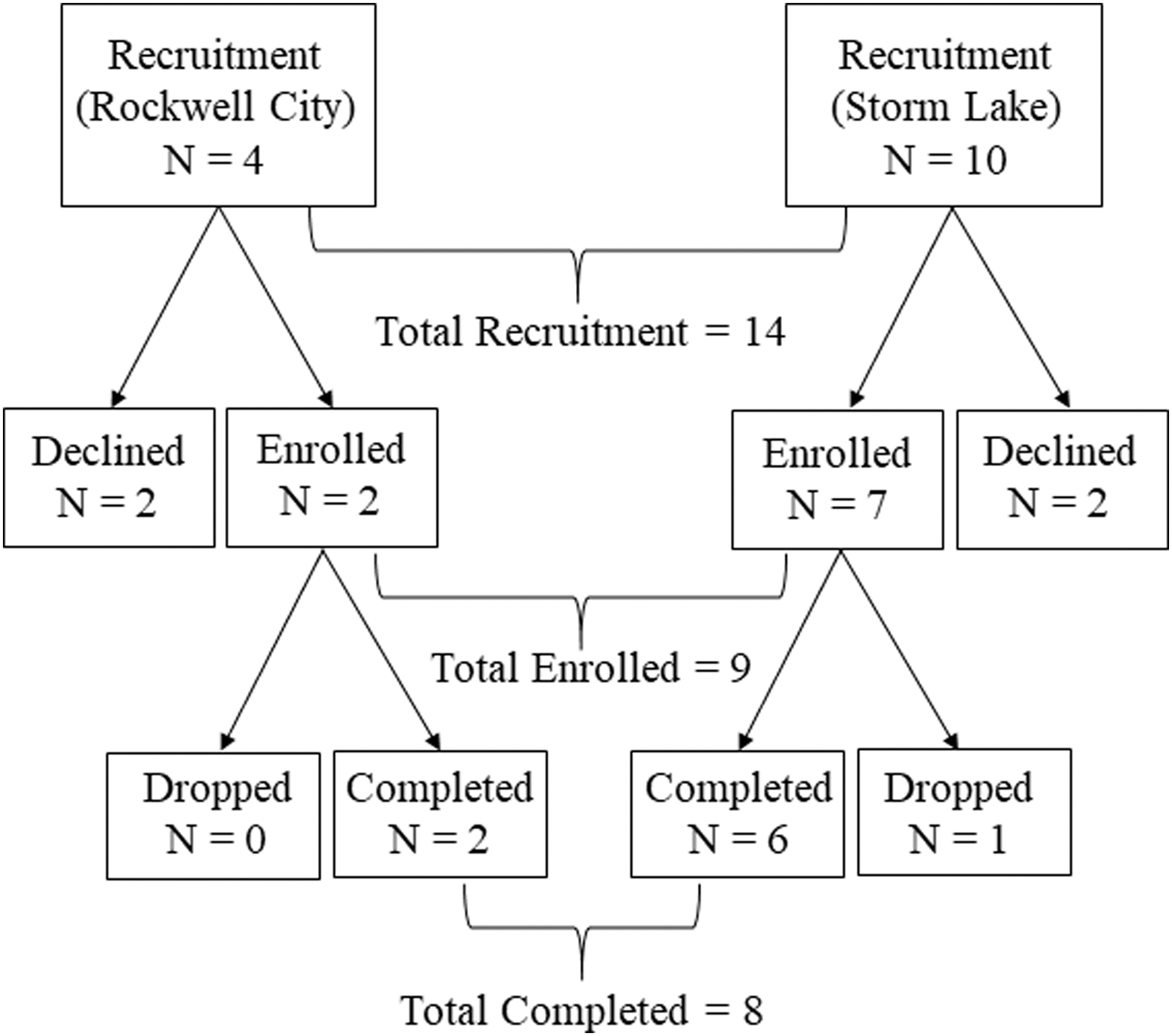
Flow diagram of the participant recruitment, enrollment, and study completion.
Participant Demographics
UPDRS, Unified Parkinson's Disease Rating Scale.
Due to schedule limitations, participants enrolled in the study were allowed 9 weeks to complete 8 weekly sessions. Five participants attended all eight sessions, two participants completed seven sessions, and one participant completed six sessions for 93.75% compliance.
Effectiveness
Results are reported for the eight participants who completed the pre- and post-data collections. Figure 2 shows individual data for each outcome measure. Results revealed no significant differences between the pre- and post-measures of the voice outcome measures. The mean for phonation duration was the only outcome measure that showed any decline, though minimal (d = 0.09). The mean for all other voice outcome measures improved, but not to the level of significance. For respiratory control, the mean for both outcome measures improved from pre- to post-assessment. Both mean MEP [t(7) = −3.70, p = 0.008] and mean MIP [t(7) = −2.18, p = 0.06] reached significance. See Table 2 for descriptive and inferential statistical results.
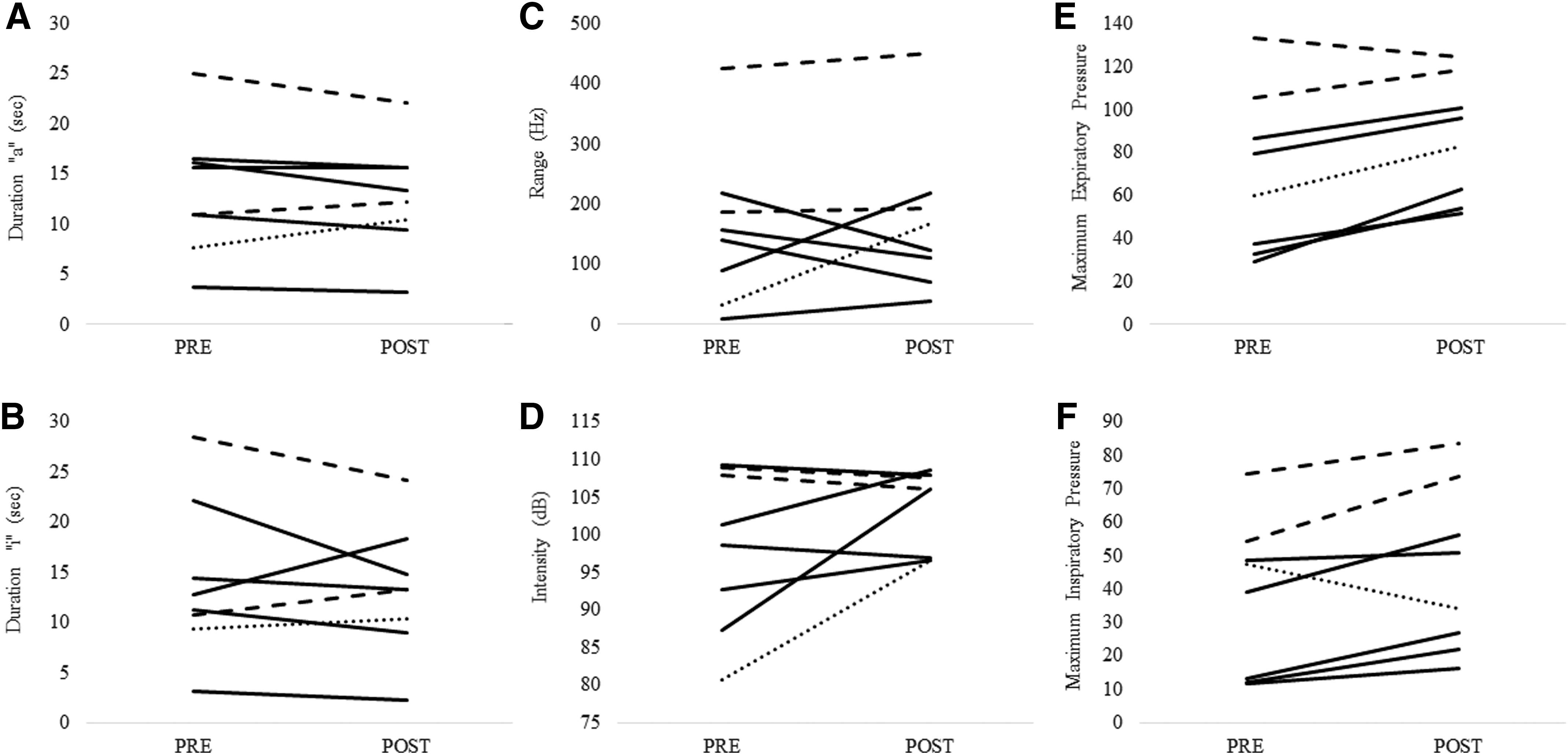
Individual data for each outcome measure are shown. (
Descriptive and Inferential Statistics for all Outcome Measures
All values are shown as mean ± standard error. Asterisk designates a significant difference between the pre- and post-values.
df, degrees of freedom; MIP, maximum inspiratory pressure; MEP, maximum expiratory pressure.
Discussion
To the best of our knowledge, this is the first study to demonstrate the feasibility and effectiveness of a prerecorded GTS program for persons with PD living in a rural environment. The enrollment rate was above 57.14% and compliance was above 93.75%. Our pilot results revealed that there were no significant changes (positive or negative) in the voice outcome measures after the 8-week program. However, both respiratory control measures significantly improved. These results support our hypotheses. This pilot work is promising and suggests that the use of prerecorded GTS may be a viable treatment option for those with limited access to care.
The results of this study are generally in keeping with results from our previous study using the exact same intervention with an in person therapist. 20 Voice outcome measures did not change, but the respiratory outcome measures reached significance. This suggests that the prerecorded GTS program may be as effective as the in person GTS program for improving respiratory control in persons with PD. However, phonation time declined slightly over 8 weeks in this study, whereas phonation time improved in the in person GTS program. 20 An increase in phonation time requires a steady control of the release of air. Even though MEP increased, this did not translate to the controlled release of air in this study. Thus, in person instruction may be more beneficial for translating improvements in air pressure to improvements in air control. However, phonation time did not decline in all participants in the study, and the effect size was small (d = 0.09). Some participants did increase their time while other stayed the same. Thus, the small participant number in this study (n = 8) compared with the in person GTS study (n = 30) may be the largest contributor to different results for phonation time. 20
Results of studies investigating singing in persons with PD have been equivocal. 13 –15,17 Small samples sizes and differences in approach, music therapy versus choral singing, may contribute to these results. Interestingly, this study replicated the exact intervention methods and data collection methods used in a previous music therapy-based program and revealed similar results. 20 This supports the notion that using a music therapy-based approach to therapeutic singing may be a reliable therapy for voice and respiratory impairments in persons with PD. However, the primary challenges with any therapy are access to care and compliance. In particular, access to care and a lack of compliance after speech therapy may further limit treatment of voice and respiratory problems in persons with PD. 22 In this study, there was a 93.75% compliance among all participants, and the prerecorded GTS program provided access to care to those who would not normally be afforded the opportunity for continued therapy. Thus, using a prerecorded GTS program may be a viable option to increase compliance and continue with treatment after speech therapy is discontinued in persons with PD, especially in rural areas where access to care is limited.
Conclusions
This study has established that using a prerecorded GTS program is feasible and effective for persons with PD in rural areas. Future larger efficacy and clinical trials randomizing participants to prerecorded GTS or in person GTS are needed to more fully understand which approach is most beneficial. Nonetheless, GTS is a promising therapeutic approach for persons with PD.
Footnotes
Acknowledgment
This material is based on the work supported by the Iowa State University Extension and Outreach and joint Iowa agricultural extension districts.
Disclosure Statement
The authors declare that there is no conflict of interest.