
Abstract
Introduction:
The Integrated Telemedicine and e-Health program (ITeHP) of Albania, built by the International Virtual e-Hospital Foundation (IVeH), has improved access to high-quality health care, particularly in high demanding specialty disciplines. We aimed to test the hypothesis that the majority of patients in remote and regional hospitals can be managed using telemedicine and will prevent unnecessary transfers.
Methods:
A retrospective analysis of prospectively collected data of patients seen between January 2014 and September 2018 was conducted. Patient demographics, type of teleconsultation modality used, and patient disposition were analyzed. The comparison of continuous data was performed with t-test or Mann-Whitney test. The categorical data were tested with chi-squared test and analysis of variance.
Results:
There were 2,842 patients seen in all the clinical disciplines during the study period. We excluded tele-autism and incomplete data. There were 2,724 records eligible for study. The most frequent consulting clinical programs (82.9%) were teleradiology (39.0%), teleneurotrauma (27.2%), and teletestroke (16.7%). The majority of patients (77.9%) were kept at regional centers and did not require transfer (p < 0.001) to a tertiary center. Of those transferred, 70.3% were male (p < 0.001), of which 81.6% were for transferred due to neurotrauma.
Conclusion:
The telemedicine program in Albania has improved access to specialized care in a number of specialty clinical disciplines, particularly in potentially life-threatening and time-sensitive conditions such as neurotrauma. Almost 80% of patients did not require transfer to tertiary centers and were kept for further treatment at the regional centers.
Background
The Integrated Telemedicine and e-Health program in Albania (ITeHP-Albania) was established by the International Virtual e-Hospital Foundation (IVeH) in a collaborative effort with the U.S. Agency for International Development (USAID)/Albania, the U.S. Army Corps of Engineers, and the government of Albania (Ministry of Health and Social Affairs [MOHSA]), and the University of Arizona. This program was developed based on previous telemedicine models implemented in Kosova and in Cabo Verde. 1 –4
IVeH's comprehensive four-pronged strategy, initiate-build-operate-transfer (IBOT), ensures a step-by-step sustainable approach to rebuild the health care system using telemedicine and advanced technologies. 3,5
The telemedicine program in Albania has been operational from inception in 2010 and has grown into a large telemedicine network (Fig. 1). It serves the entire country with a total of 36 active telemedicine centers and telemedicine clinical portals/units. Out of these, 19 centers provide teleconsultations. The rest of centers include 11 regional hospitals and 3 municipal hospitals that refer the patients. There are three mobile units to complete telemedicine network in Albania. In January 2017, the program was transferred to MOHSA as an integral part of the National Center of Biomedical Engineering (NCBE).
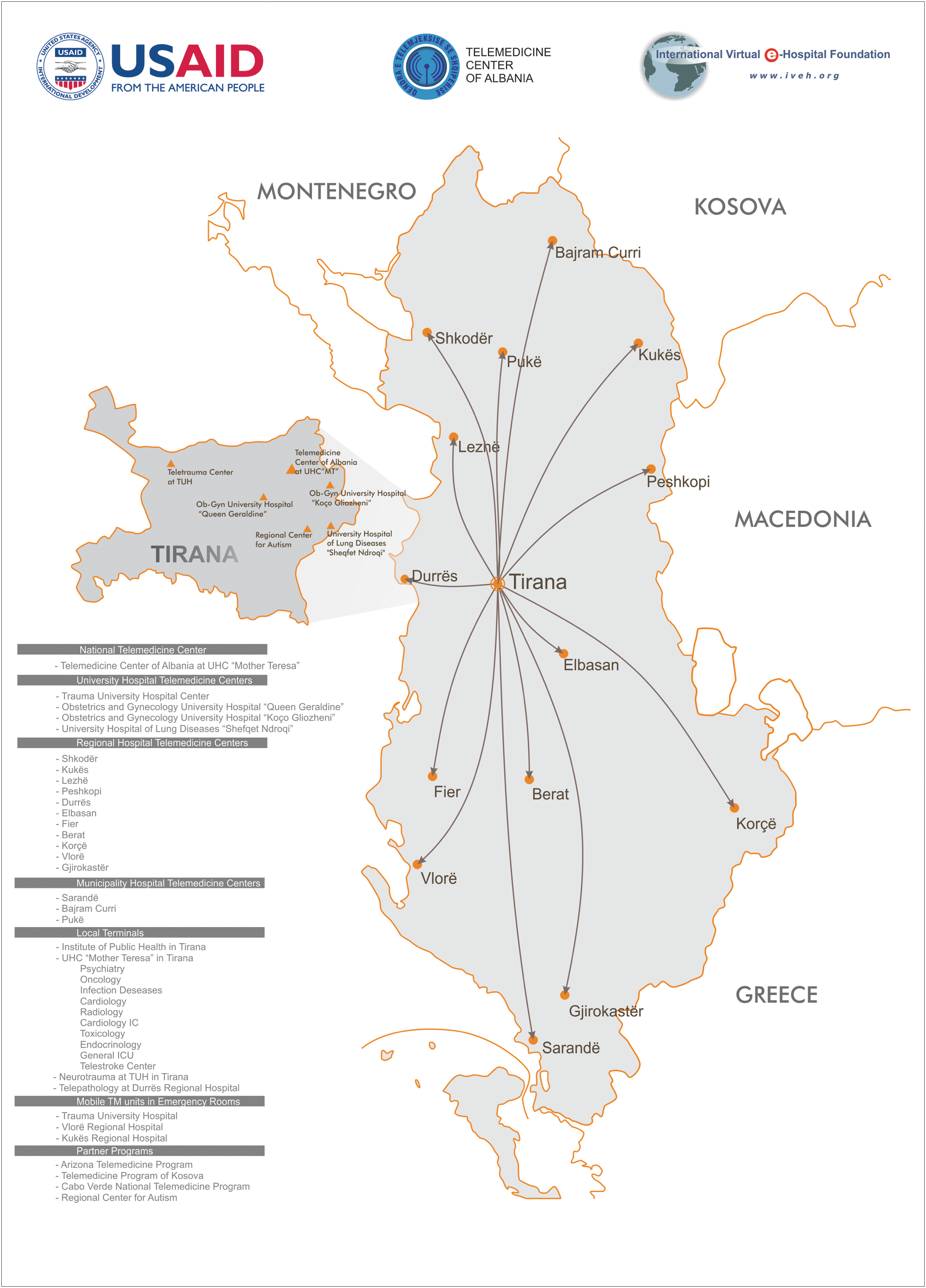
Albanian Telemedicine Network.
The need for telemedicine services and a concomitant increase in access to all clinical disciplines in Albania, particularly in high-risk specialty disciplines, where services are concentrated in the capital city, is obvious. With the fall of communism in the 1990s, the Albanian health care system was divided into public and private health care. While this process in one way has added other services, the public health care system has not made much progress. In 2014, IVeH conducted an analysis of the trauma system of Albania using the American College of Surgeons/Committee on Trauma (ACS/COT) criteria. We found that trauma and emergency medicine systems were in need of major reforms and lacked essential elements to meet the basic requirements of a structured trauma system. 6 In a subsequent study by our group, it was reported that emergency services in Albania were staffed with inadequately trained personnel. In addition, there was a lack of necessary equipment and protocols to support appropriate care. 7 An analysis of 42 public hospitals found major deficiencies in the ability to provide emergency services and a lack of specialized trauma training for both physicians and nurses. Only about half of the emergency room physicians and 20% of the nurses possessed basic life support certification. Between 50% and 71.4% of the facilities showed a combined lack of training and supplies. This was the reason for not offering interventions such as rapid sequence induction, needle thoracotomy, chest tube insertion, and thrombolytic therapy. Furthermore, this study demonstrated some significant differences in the emergency medical care provided between primary, secondary, and tertiary hospitals across Albania. Since that publication by Latifi et al. 7 there have been major efforts in rebuilding emergency services in Albania with a current state-of-the-art coordination center. 8,9 We aimed to test the hypothesis that the majority of patients in remote and regional hospitals can be managed using telemedicine and this will prevent unnecessary and costly transfers.
Methods
A retrospective analysis of prospectively collected data of patients seen between January 2014 and September 2018 was conducted. All the clinical disciplines that used telemedicine were reviewed, except tele-autism, consistent with previous report. 10 Patients with unknown clinical discipline or action taken during telemedicine consultation were excluded. We analyzed the data in three steps. First, we studied all clinical disciplines together. Second, only the neurotrauma program with more detailed information was reviewed. Finally, we analyzed the overall data without teleradiology. The age of patients as a variable was available as continuous data. We categorized the age variable and studied each age category separately to determine the age strata, accounting for statistical differences.
Call-to-response (CTR) time was calculated in minutes, representing the elapsed time from the initial call from the regional hospital or referring physician to response time from the specialist. In this article, telemedicine centers are referred to as centers or consulting centers based on their action in the telemedicine network. In addition, the name of telemedicine center (national, regional hospital, tertiary center, and municipality hospital) or portals/units (specialty-based telemedicine units) based on their location.
We compared the number of transfer versus nontransfer patients based on the modality of teleconsultation: (1) asynchronous, (2) synchronous, or (3) a combination of both modalities. We compared two groups (transfer vs. nontransfer) using chi-squared test for the three most prevalent programs (teleradiology, teleneurotrauma, and telestroke) that comprised 82.9% of the consult requests. In the second step of the analysis, we compared the neurotrauma patients based on their transfer status. In the third step, after excluding radiology, we followed the same procedure to analyze the data. We looked at the data without teleradiology because teleradiology is expected to be performed remotely. The trend of the rate of transferred patients over the years of study was measured with one-way analysis of variance testing and regression analysis. For all the data, we performed overall analysis and subgroup analysis for programs or hospitals individually, whenever applicable. The comparison of continuous data was performed with t-test or Mann-Whitney test. Categorical data were tested with chi-squared test. The analysis was performed with SPSS (Version 24.0; IBM Corp., Armonk, NY).
Results
There were 2,842 patients who were managed using telemedicine program in all clinical disciplines. We excluded 118 patients—90 tele-autism patients, and 28 patients with missing data (unknown clinical discipline and unknown or no action taken during the consult). Ultimately, 2,724 patients remained for analysis. The most frequently consulting clinical disciplines were radiology 39.0%, neurotrauma 27.2%, and stroke 16.7% (Table 1). The difference in transfer status was statistically significant (p < 0.001) for radiology, neurotrauma, stroke, pneumatology, psychiatry, nephrology, and surgery.
Clinical Disciplines
Other: orthopedics 5, cardiology 20, ENT 17, gastroenterology and hepatology 17, toxicology 16, ICU 15, trauma 5, infectious disease 13, hematology 12, urology 12, pediatrics 8, maxillofacial surgery 7, rheumatology 6, thoracic surgery 6, endocrinology 5, vascular surgery 5, oncology 4, ophthalmology 4, allergology 3, gynecology 3, cardiology ICU 2, pediatrics surgery 2, pediatrics ICU 1, pediatric nephrology 1, pediatric radiology 1, plastic surgery and burns 1.
ENT, ear, nose, and throat; ICU, intensive care unit.
Age (as a continuous variable), was significant between nontransfer and transfer patients (p = 0.001.) However, this significance was only in the age group 70–79. While the rate of transfer patients increased from 2014 through 2017, overall there is a smaller size of transferred patients to a tertiary center in each year. The rate of transfer patients decreased in 2018 (Fig. 2). The CTR time was shorter in the transfer patients and the difference was statistically significant (median, 20.8 vs. 113.0 min, p < 0.001) Table 2.
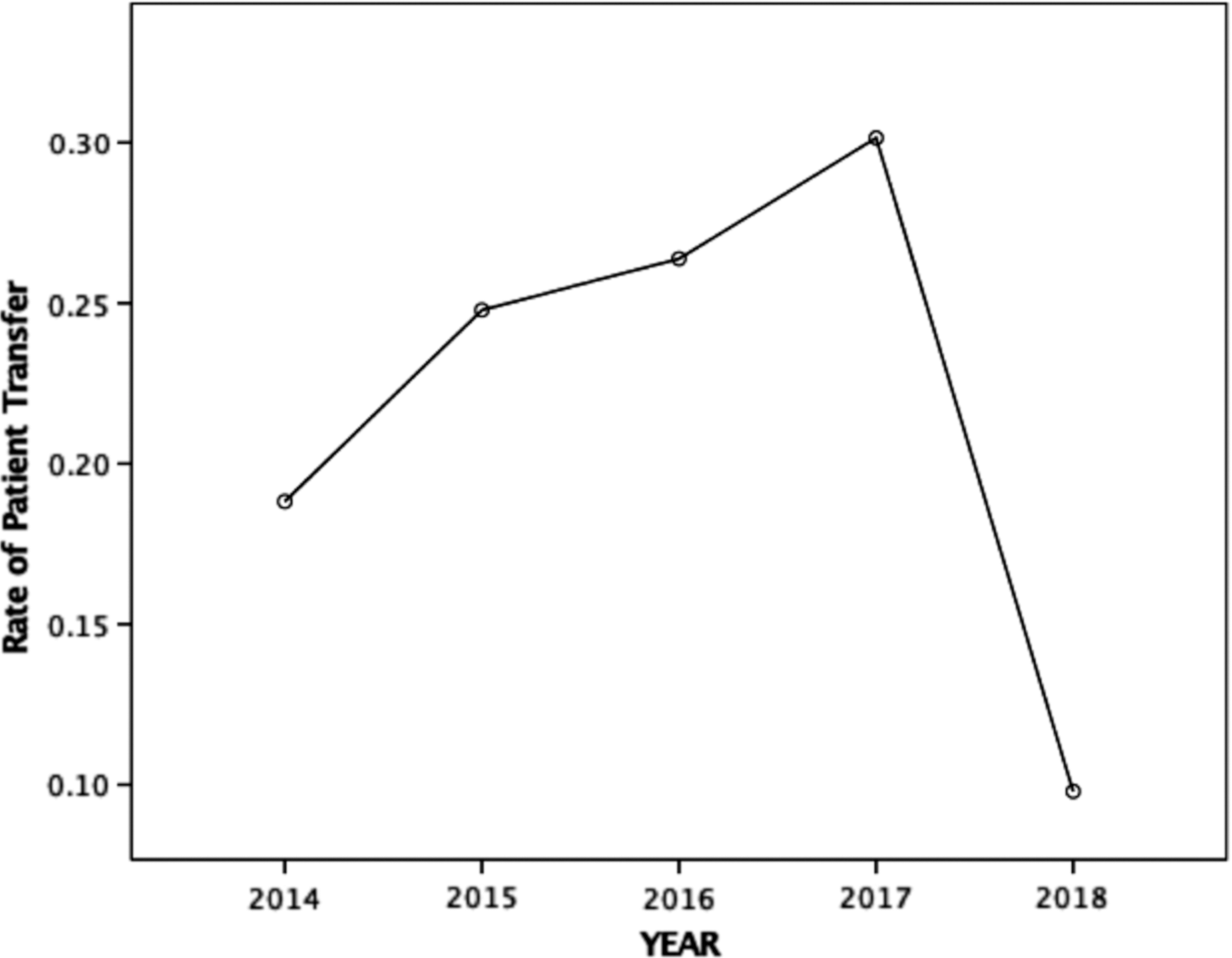
Rate of patient transfer 2014–2018.
Comparison Between Nontransfer and Transfer Groups
The records in 2018 were for 9 months of the year.
Two hundred and eighty-eight (10.6%) of the age values were unknown.
CTR, call to response; IQR, interquartile range; SD, standard deviation.
There were 16 hospitals requesting telemedicine consults from around the country, and the greatest portion of the consults, 45.9%, was from Vlora Regional Hospital (Fig. 1). As the largest tertiary medical center in the country, the Mother Teresa University Hospital Center accepted 54.4% of the consultations (Table 3).
Referring and Consulting Centers
Various specialists consulted in Vienna, requested by patients themselves were performed at different institutions.
Table 4 represents the distribution of the modality of teleconsultation between transfer and nontransfer patients for the three most prevalent clinical disciplines. In each modality, the number of transfer patients was a small portion of the total patients, except for live teleconsultation in neurotrauma, although this difference was not statistically significant (p = 0.198).
Transfer Status per Three Most Common Technology
Overall, transfer neurotrauma patients were slightly older (42.5 vs. 44.8, p = 0.215), but there was no statistical difference. However, the difference was statistically significant in the stratum of patients ≥80 years of age (p = 0.021). Similar to overall clinical disciplines, only a smaller portion of neurotrauma patients were transferred to a tertiary center each year as follows: 23.8% in 2014, 33.3% in 2015, 29.9% in 2016, 37.1 in 2017, and 35.9% in 2018. The two centers that requested most consults for neurotrauma were Vlora Regional Hospital (51.8%) and Korca Regional Hospital (32.9%). All the teleneurotrauma consults (100%) were provided by University Hospital of Trauma.
The transfer rate in Vlora Regional Hospital was 22.7% and in Korca Regional Hospital, it was 46%. Comparison of the transfer and nontransfer patients for these two centers was statistically significant (p < 0.001). The comparison of nontransfer versus transfer patients from Kukes Regional Hospital was associated with a p < 0.05, but for this hospital, the rate of transfer patients was slightly higher (8 vs. 10). The same observation was true for Berat Regional Hospital (2 vs. 6) (Table 5).
Comparison Between Nontransfer and Transfer Groups—Neurotrauma
N/A, not applicable.
We compared the median CTR time for each hospital individually and overall as a group. In general, transfer patients were consulted faster (15.0 vs. 20.0 min, p < 0.001). In Vlora Regional Hospital, the median CTR time was almost the same (19.5 vs. 21.0 min, p = 0.260) between the two groups. In Kukes Regional Hospital and Peshkopi Regional Hospital, the median CTR time was longer for the transfer patients, but it did not reach statistical significance. Median total CTR time was the longest in the Berat Regional Hospital (23.3 min) (Table 6). In the neurotrauma cases, 95% of the consults were provided within 111.0 min, with median of 17.2 (11.9–31.0) minutes. Table 7 illustrates the telemedicine program characteristics, when radiology was excluded. There was no statistical difference in age between transfer and nontransfer patients. Males were almost equally distributed between transfer and nontransfer patients (p = 0.159).
Call to Response between Regional Hospitals—Neurotrauma
In the Berat Regional Hospital the number of nontransferred patients was only two. Therefore, median was not calculated.
Comparison Between Nontransfer and Transfer Groups—Radiology Excluded
CTR, call-to-response; IQR, interquartile range; SD, standard deviation.
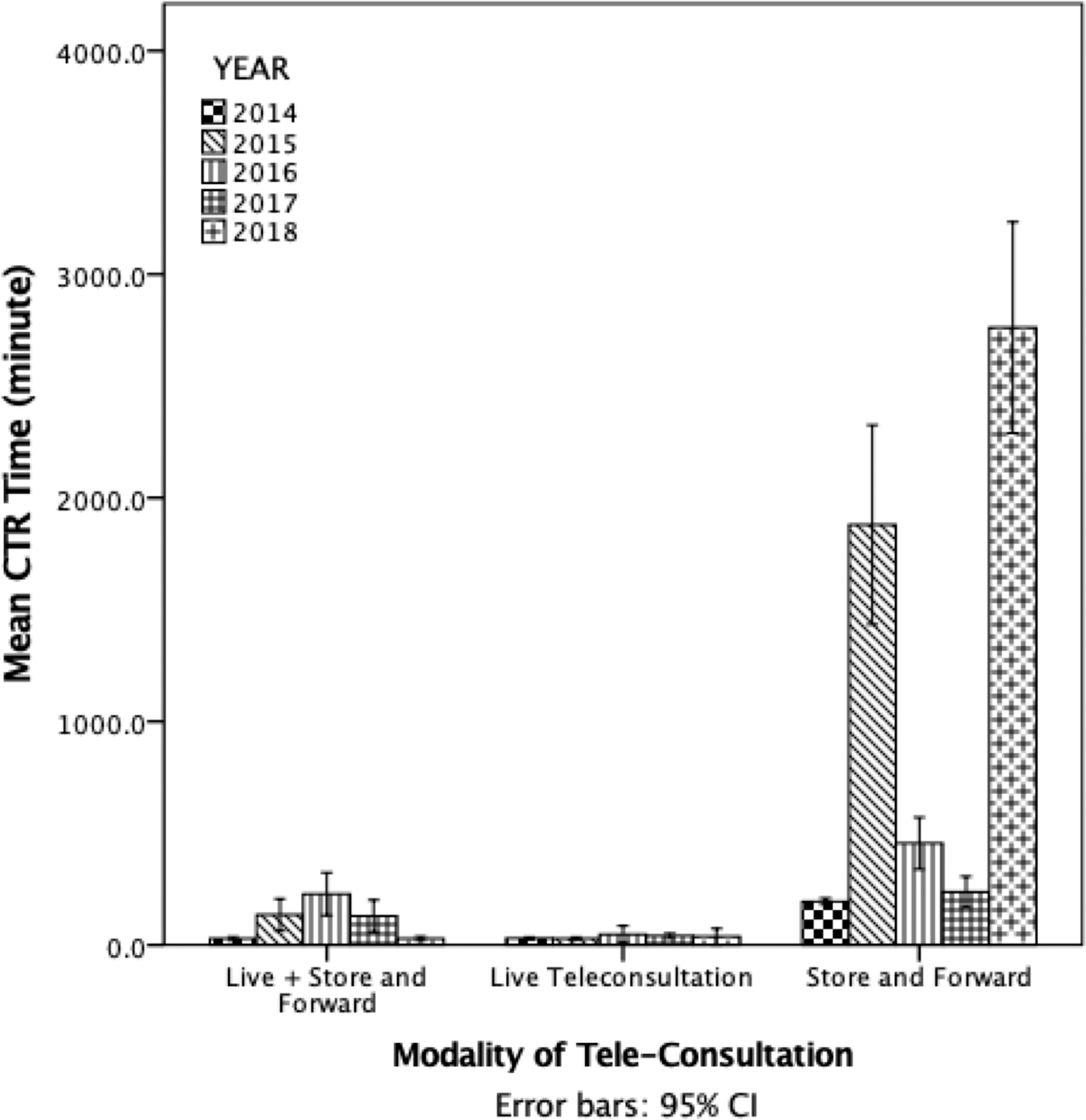
This is unlike overall patients at all the disciplines without excluding radiology (p < 0.05), where we note statistical difference. Korca Regional Hospital and Vlora Regional Hospital were the two most frequent hospitals that requested radiology consult. These two regional hospitals had the highest number of request for telemedicine consults, even without excluding radiology. However, they switched their order in terms of frequency when the data were considered with and without radiology. Most common consultation modality for all clinical disciplines was store-and-forward with the longest mean CTR time in all years (Table 8, Figs. 3 and 4).

Distribution of technology during years-all programs. CI, confidence interval.
Distribution of mean CTR during years-all program. CTR, call-to-response.
Mean Call to Response for Each Year with Comparison to 2014 (Starting Year)
Discussion
We have demonstrated that the majority (77.9%) of patients were kept at the regional centers for management and did not need to be transferred to the national tertiary centers in Tirana. We assumed that nontransferred patients truly did not require transfer based on advisement from the consulting specialists. The results of this analysis are consistent with previous reports by our group. 10 Out of 1,065 patients managed by telemedicine during the 20-month study period, 974 patients did not require transfer. 10 Radiology, neurotrauma, and stroke were the most frequently requested specialties for teleconsultations (82.9%).
The mean response time for both asynchronous and the combined modality (asynchronous and synchronous) was significantly shorter in 2014 than 2015 (p < 0.01), whereas there was no significant difference seen for live teleconsultations only (p = 0.76).
Timing of CTR for teleconsultation is an important aspect of increasing immediate access of patients, particularly for highly specialized care. In this comprehensive review for the years since the initiation of the program, the mean CTR in all years and for each technique is depicted in Table 8 and Figures 3 and 4. In 2018, the CTR for the asynchronous modality was statistically significantly longer than 2014. The CTR for the other two technological modalities was not statistically significant in 2018.
As far as patients' disposition following teleconsultation, only 20% of patients in 2014 and 22.7% of patients in 2015 were transferred to a tertiary hospital. As such, most patients did not need to travel to Tirana from regional hospitals.
In this study, we observed that the low rate of transfer patients continued in 2018 as well (Table 2). When asynchronous technology was used, only 2.7% of patients were transferred to the tertiary hospitals in 2014 and 9.9% in 2015. However, when the synchronous modality was used, 83.1% of patients were sent to the tertiary hospitals in 2014 and 51.7% in 2015. When a combination of modalities was used, 46.5% of patients were transferred to the tertiary hospitals in 2014 and 34.1% in 2015. During 2014 to 2018, 167 out of a total of 602 transferred patients were managed using combination of both modalities. Yet, this was the smallest among the three different modalities used (Table 2).
Teleneurotrauma continues to be the main pillar of access to care for specialized care. 11 In this first study of 146 teleconsultations for neurotrauma, the majority were performed asynchronously (84%), while the combination modality was employed in only 15% of cases. Median time of respond to teleconsultation was 20 min. Sixty-six percent of patients remained at the referring hospital for further observation and did not require transfer to trauma center. Of the patients transferred to the tertiary care, 91% were treated nonoperatively, 85% were discharged to home, 9% were transferred to another hospital, and 6% died in the hospital. 11
This analysis demonstrates a number of very important elements of usability and sustainability of a nation-wide telemedicine program. Just the mere fact that we built a telemedicine network, it does not mean that it will be used by practitioners. The Albania program is a fine example of this. We suggest that, to create and maintain successful telemedicine program, a number of sustainability factors have to be introduced and implemented, which our group and others have reported. 3 –5,12 –20
These include the following: the IBOT strategy, creating the infrastructure, establishing policy and clinical protocols, overall good organization of the program, careful training and development of solid human capacities, continuous support of the program, presence of e-government, appropriate use of country's assets, continuous funding, dedicated or protected time or inclusion and managing time of the physicians to perform telemedicine consults, and finally, almost most importantly, political support from the government leadership. Yet, once the infrastructure is built, the most important factors for continued success of telemedicine programs are established protocols for receiving and delivering consultation in timely manner at tertiary centers, and local physician and hospital leadership champions at the remote sites. In our study, the neurotrauma, stroke, and radiology continue to be main pillars of telemedicine in Albania. The hospitals in Vlora and Korqa continue to use telemedicine to provide care for their communities.
The role of established protocols and local champions has been demonstrated in other projects in the literature. One of the most impressive is the cardiology project in Brazil. 21 In this project between 2012 and 2014 73,751 babies were screened for heart defects and 857 abnormalities were identified. Detection of congenital heart diseases increased from 4.09 to 11.62 per 1,000 live births (p < 0.001). Over 6,000 consultations and echocardiograms were supervised through the internet. Time to diagnosis, transfers, and hospital stays were greatly reduced. Another very successful telemedicine pediatric cardiology program is one in Cabo Verde. Since 2009, children with cardiac anomalies are examined by a local cardiologist, and the cardiac ultrasound images are sent to cardiac surgeons in Portugal, after which these children are evacuated for definitive surgery. This has proven to be an important improvement in the care of these children, who otherwise would not have been able to get care in Cabo Verde, as they do not have pediatric cardiac surgeons. 3,10
Although there are a number of smaller scale telemedicine projects led by western countries and institutions in the developing countries reported, 22 the real contribution to health care system in the developing countries is not clear. Bediang et al. 23 listed a number of factors as key to sustainability of telemedicine and e-Health efforts in Africa, of which most importantly are lack of ownership by stakeholders, lack of interoperability as many of the projects are deployed by multiple organization, and finally, lack of basic infrastructure and training support. Lack of e-government readiness, enabling policies, and the capacity-building process as crucial components has been emphasized. 22
Despite successful implementation of the telemedicine in Albania, there is much more that needs to be done. If one just scans the result of current main clinical disciplines used (Table 1), it becomes obvious that the majority of clinical disciplines do not use telemedicine. If one would summarize the lessons learned over the last few years of the implementation of a nation-wide telemedicine program in Albania, the key to success would be physician and hospital administrator champions. Moreover, clinical discipline protocols for teleconsultation and a buy-in of physician specialist are an absolute must. Finally, updating technologies and maintaining strong administrative support of the program (not a case in Albania for last 2 years) are detrimental. This study has several limitations: While we know that in light of telemedicine program in Albania, patients are transferred less than before, we do not know that they necessarily have a better outcome as well and less transfer may or may not result in improved care clinically; We have no detailed clinical information for transferred and nontransferred patients. This article's focus is accessibility and transfer rate of patients undergoing telemedicine consultation; Although there is only one neurotrauma center, and if any of the patients are not transferred initially, most likely they would have been sent subsequently to the trauma center, we do not have that data; and Finally, we do not have financial data and cost savings to the health system from preventing unnecessary transfers. The future studies should be designed with all these elements. A survey of all other specialties that do not use telemedicine similar to neurotrauma, radiology, and stroke should be done, so may gain a better understanding of the invisible barriers to implementing routine telemedicine.
Summary
We conclude that development and deployment of telemedicine in Albania has been an important step in rebuilding health care services in Albania. Despite challenges in maintaining the human capacities, as well as involving most clinical disciplines, it is proving to be a valuable tool for access to care for many. Moreover, to justify further its existence and cost of building and maintenance, the telemedicine program in Albania has to demonstrate acceptable expansion and coverage. There is still a need to grow and cover more clinical settings, while the necessary infrastructure is consistently getting stronger. Yet, this program has improved the quality of patient care and management, especially in life-threatening and time-sensitive conditions such as neurotrauma or stroke. Avoidance of unnecessary transfer is beneficial for both patients and the Albanian health care system.
Footnotes
Acknowledgments
The authors acknowledge the entire team of the Integrated Telemedicine and e-Health program (ITeHP) of Albania and many people who work hard to make this program a reality and success.
Disclosure Statement
No competing financial interests exist.