
Abstract
Background:
When implementing e-health solutions, effective integration into a clinic's existing processes is essential to facilitate adoption and sustained usage.
Introduction:
This article examines the effectiveness of adoption/utilization of an electronic consultation (eConsult) service by primary care providers (PCPs) using a “delegate model,” through which referral clerks manage requests on behalf of PCPs, thereby reducing PCPs' administrative burden.
Materials and Methods:
We conducted a retrospective cross-sectional study of all eConsults submitted between May 1, 2013, and December 31, 2017, by the Bruyère Academic Family Health Team (FHT), after the clinic implemented the service using a delegate model. We assessed system utilization, including monthly volume of submitted eConsults, requested specialties, and impact on PCP referral behavior based on the mandatory closeout surveys. We also conducted a subanalysis to compare the volumes of eConsults per provider between the FHT and all other providers.
Results:
The Bruyère Academic FHT submitted 3,233 eConsult cases. Volume increased 3.5 fold, from 285 in the first year to 1,016 in the last year. Active Bruyère Academic FHT providers (those who submitted ≥3 cases in 6 months) submitted a median of 25 eConsults (interquartile range [IQR]: 14.75–35.25) versus 14 (IQR 8–24) for all other active users. In 36% of cases, a referral was originally contemplated but avoided based on specialist advice. In 5% of cases, the referral was not originally contemplated but deemed appropriate by the PCP based on specialist advice.
Discussion:
Our findings show high levels of eConsult use in the clinic utilizing a delegate model, which persisted throughout the study period and was reported to significantly reduce the backlog of traditional referrals at the clinic.
Conclusions:
The integration of eConsult capability into existing clinic operations was successful in that it allowed the PCPs to request eConsult using a familiar process, avoiding the challenges associated with adopting a new and unfamiliar technology.
Introduction
There is an urgent need to transform the delivery of specialist care for Canadians. The results of the Commonwealth Fund survey in 2016 ranked Canada last among 11 countries surveyed on wait times for specialist care, with 56% of Canadians waiting more than 4 weeks to see a specialist compared with the international average of 36%. 1 Digital health solutions, such as electronic consultation (eConsult), an asynchronous communication tool that facilitates virtual conversation between primary care providers (PCPs) and specialists about the patient, are a promising approach to improve timely access to specialist advice. Through eConsult, PCPs are able to manage some conditions with remote support by the specialist, often without the patient themselves needing a face-to-face specialist appointment.
Accumulating evidence indicates that eConsult and other technologies that encourage knowledge sharing in new and efficient ways optimize care coordination and efficiency. For example, eConsult services have been shown to reduce wait times, improve access to specialist advice, and increase PCP and specialist satisfaction with the primary care/specialty care interface. 2 –5 Although eConsult services allow PCPs to retain a central role in more patients' care, some PCPs have expressed concerns over broadened clinical responsibilities and frustrations with the increased administrative workload and interface issues. 6 These concerns have been linked to the issue of physician burnout, which is being increasingly recognized as a systemic health care problem with adverse impact on physician health and patient care. 7,8 Since provider experience has been shown to have a substantial impact on adoption of new technology innovations and overall quality of care, a careful consideration of increased workload and burnout challenges is necessary to inform decisions on how best to implement an eConsult service.
The Bruyère Academic Family Health Team (FHT), a clinic operating in Ottawa, Canada, has implemented a novel approach to address this issue. The FHT had previously developed a well-functioning process to streamline traditional referrals, in which the PCP entered the pertinent information into a template form with the patient's electronic medical record (EMR). A referral clerk would then act as a delegate, drawing out the information and submitting the referral request. On implementing eConsult, the FHT adapted this process by having PCPs complete eConsult templates within the EMR, from which the referral clerk would copy the information and enter it into eConsult's web-based form for submission. The delegate model provided a low-cost method of integrating eConsult into the clinic's existing workflow for referrals with minimal disruption for providers. In this study, we examine the effectiveness of this structure by assessing eConsult's use and outcomes at the clinic.
Materials and Methods
Design
We conducted a retrospective, cross-sectional study of all eConsult cases submitted by the Bruyère Academic FHT between May 1, 2013, and December 31, 2017.
The Champlain Base™ eConsult Service
The Champlain BASE (Building Access to Specialists through e-Consultation) eConsult program is a web-based service that allows PCPs to submit nonurgent patient-specific clinical questions to specialists from 114 specialty groups. Since its creation in 2010, the eConsult service has completed more than 47,000 cases and enrolled more than 1,400 PCPs. Additional patient information, such as medical history, medication lists, and laboratory and imaging results, can be added to the eConsult if needed. Specialists respond within 1 week and can provide PCPs with recommendations, request additional information, or recommend a face-to-face referral. After the specialist responds, ongoing communication between PCPs and specialists is possible until the PCP closes the eConsult. PCPs typically incorporate the relevant eConsult information into their patient's chart, communicate relevant outcomes to the patient, and implement any recommendations. PCPs receive a response in an average of 2 days, and two-thirds of cases are resolved without the patient ever needing a face-to-face specialist visit. 2 The service has been evaluated in Eastern Ontario and presently operates as a fully funded service through the Ontario Ministry of Health and Long-Term Care, with province-wide expansion underway.
Setting
The study was conducted by the Bruyère Academic FHT, located in Ottawa, Canada. In Ontario, FHTs were created to expand access to comprehensive family health care services as community-centered primary care organizations whose programs and services are geared to the population groups they serve. They include an interprofessional team of family physicians, nurse practitioners, registered nurses, social workers, dietitians, pharmacists, and other professionals who work together to provide primary health care for their community. Each team is set up based on local health and community needs.
The Bruyère Academic FHT is located within the Élisabeth Bruyère Hospital. It is a primary care practice divided into two practice sites that provide care for 17,000 patients. The eConsult service was implemented within the team, starting in 2013.
Participants
All PCPs in the Bruyère Academic FHT who submitted eConsult cases during the study period were included in the study.
Intervention: Processing Econsult Referral Requests Using a Delegate Model
The Champlain BASE eConsult service operates on a secure online platform accessed through an internet browser. Typically, in an EMR-using clinic, completion of an eConsult requires PCPs to log into the service using a separate username and password, transfer patient data from the EMR into the online submission form, and then send the eConsult. Once they receive a reply, PCPs need to log back into the platform, copy the response, and paste it into the EMR. The Bruyère FHT decided to make this process less cumbersome by having PCPs create eConsult requests in the same manner as their routine referrals, using a form in their EMR. From this form, a referral clerk—acting as a delegate—draws and sends all outbound eConsult requests. The form contains all elements required by the eConsult service.
To request an eConsult, PCP accesses the form directly in the EMR, enters pertinent notes and questions for the specialist, selects any relevant patient data to be included from the patient's chart in the EMR, annotates them to be sent to eConsult service, and uses the EMR internal messaging feature to notify the clinic's referral clerks in the same manner as when requesting a routine referral (Fig. 1). On receiving a message, a referral clerk logs onto the eConsult server and uploads all of the relevant data into the system. Once the specialist replies, the referral clerk retrieves the information, uploads it to the EMR, and notifies the PCP using the EMR internal messaging feature. The PCP can perform follow-up actions (e.g., replying to the specialist if desired, responding to the mandatory closeout survey) in the EMR template, which the referral clerk replicates in the online platform. This process allows PCPs to request eConsults in a familiar environment, thereby avoiding the time-consuming process of learning a new application (e.g., remembering their username/password, completing the 30-min one-on-one orientation call, and familiarizing themselves with a new layout). Meanwhile, referral clerks gain expertise in the platform through frequent use, allowing them to manage cases even more quickly and efficiently. Information entered in the template is captured automatically by the patient's health record, eliminating the need to manually transfer records.

Diagram demonstrating the eConsult workflow used by delegates at the Bruyère Academic Family Health Team. eConsult, electronic consultation.
Data Analysis and Variables
We analyzed utilization data from all eConsult cases completed by the PCPs from the Bruyère Academic FHT between May 1, 2013, and December 31, 2017. System utilization data included monthly volumes of submitted eConsults, number of eConsults submitted per PCP, requested specialty groups, the specialist's response time, and time it took before PCPs closed the case.
To further measure the impact of integrating the eConsult service into the clinic workflow on eConsult utilization, we conducted a subanalysis to compare the volumes of eConsults per provider between the Bruyère Academic FHT versus all other providers using the service. For the purpose of the subanalysis, we chose a time period from January 1, 2015, to December 31, 2015, since at that time, the Bruyère Academic FHT was the only clinic using such workflow integration. An active user was defined as a provider who submitted a minimum of three eConsults in a 6-month period (January 1–June 30, 2015). Since eConsult volumes per provider did not follow a normal distribution, the counts of eConsults per PCP were reported using medians and interquartile ranges (IQR) and a Mann–Whitney U-test was used to compare the groups.
For the cases submitted in the final year of the study, between January 1 and December 31, 2017, we analyzed the impact on PCP referral behavior based on responses to the mandatory closeout survey. This let us to examine (1) whether using eConsult resulted in PCPs choosing a new course of action for treatment, and (2) whether a face-to-face consultation was originally contemplated and/or ultimately recommended. The results from Bruyère Academic FHT were compared with the overall results obtained from the service in the Champlain Local Health Integration Network. Ethics approval for this study was granted by the Ontario Health Science Network and Bruyère Research Ethics Boards.
Results
A total of 30 PCPs (26 family physicians and 4 nurse practitioners) from the Bruyère Academic FHT submitted 3,233 eConsult cases between May 1, 2013, and December 31, 2017, accounting for 10% of all cases submitted during the study period. PCPs consisted of mostly family physicians versus nurse practitioners (87.5% and 12.5% respectively), and just over half (56%) were female. Patients who received an eConsult were mostly adults between 18 and 64 years of age (59%), followed by seniors older than 65 years (26%), and children and youth younger than 18 years (15%). Fifty-nine percent were females.
The monthly volume of cases submitted by PCPs steadily increased each month, from 285 in the first 12 months of the study period to 1,016 in the last 12 months, a 3.5-fold increase (Fig. 2). During this time period, the median number of eConsult cases submitted by a PCP grew from 6 to 31. The most frequently accessed specialties were dermatology (23%), orthopedics (7%), neurology (5%), cardiology (5%), and obstetrics/gynecology (5%).
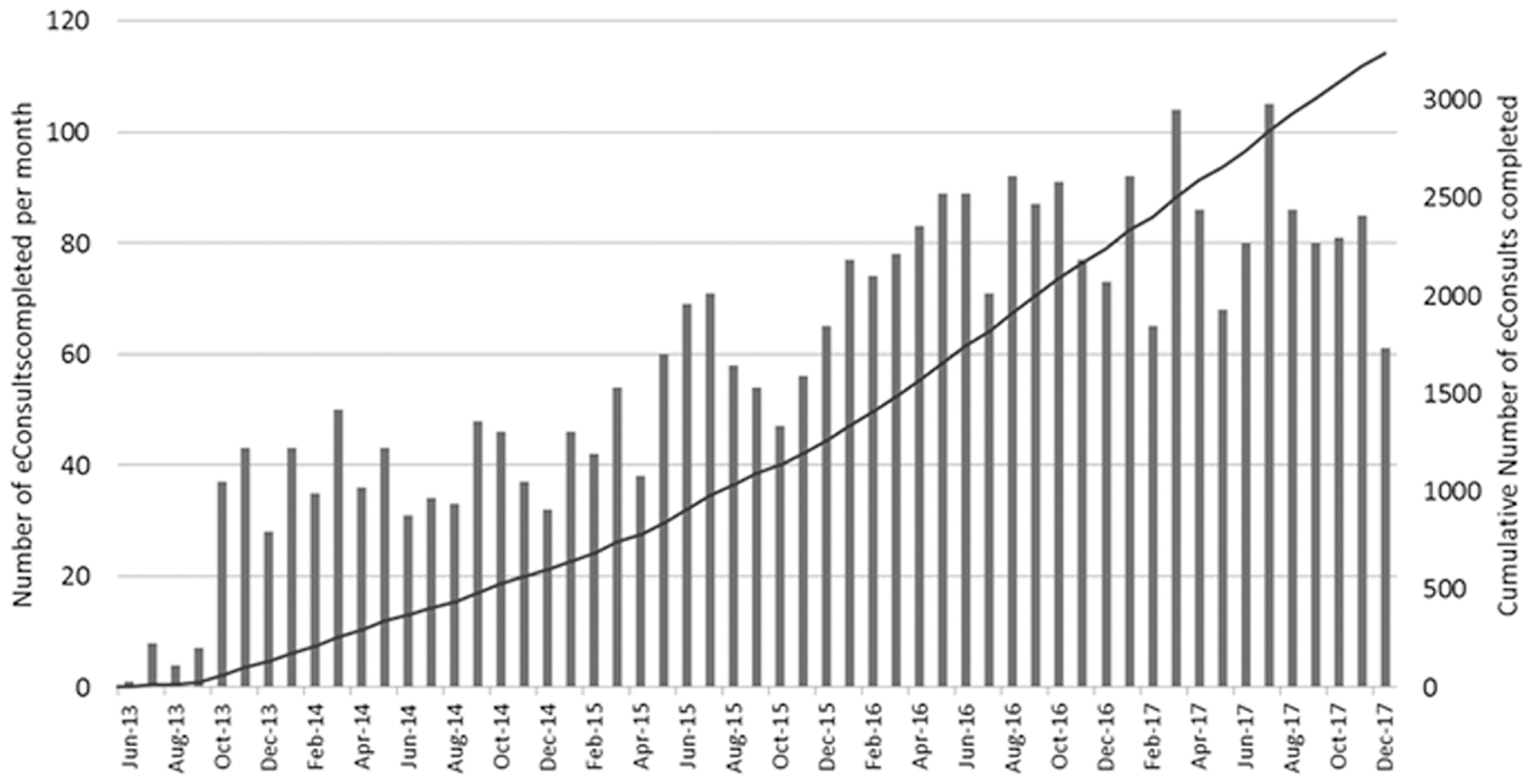
eConsult case volumes over time—number of cases completed per month and cumulative total.
Specialists responded in a median of 0.9 days, with 75% of eConsults answered within 3.8 days. The PCP closed the eConsult (meaning received, read response, and answered closeout survey) in a median of 6 days, with 75% fully completed within 10.1 days.
The subanalysis conducted on all active users of eConsult service between January 1, 2015 and December 31, 2015, who were defined as those who submitted a minimum of three eConsults in a 6-month period, revealed that the Bruyère Academic FHT providers (n = 24) submitted a median of 25 eConsults (IQR: 14.75–35.25) and all other active users (n = 239) submitted a median of 14 eConsults (IQR: 8–24), a significant difference as confirmed by the Mann–Whitney U-test.
PCPs received advice on a new or additional course of action in 58% of cases and confirmed their original course of action in 36% of cases. In only 2% of the cases, PCPs indicated that the response was not useful (the remaining 4% of responses were “none of the above”). In 36% of cases, a referral was originally contemplated but avoided based on specialist advice. In 5% of cases, the referral was not originally contemplated but was deemed as necessary based on the specialist's advice.
Discussion
The Bruyère Academic FHT's method of incorporating eConsult into its existing clinic workflow for traditional referrals via a delegate model was successful, yielding high utilization rates. The volume of eConsults sent from the clinic increased 3.5-fold over the study period. Nearly 3,300 of the clinic's patients received care facilitated by the service, 66% of whom (∼2,150 patients) were treated without needing a face-to-face specialist referral. Active users from the Bruyère Academic FHT submitted significantly higher volumes of eConsults than other providers. The utilization results observed in this study are comparable with the overall results generated by the Champlain BASE eConsult service, which completed more than 33,000 eConsults during the study period, with a median response time of 2 days, and only 28% of cases requiring a face-to-face specialist referral. 9 eConsult's effectiveness at reducing wait times, high levels of patient and provider satisfaction, and cost effectiveness have been described in previous studies. 10 –13
In alignment with other research showing a close link between technological interventions and professional burnout among physicians, 6,14 our study supports the idea that, to successfully foster adoption of innovative technological solutions without causing frustration, professional burnout, and increased administrative burden, systems must identify and eliminate low-value tasks. This can be done by, for example, streamlining work and delegation to nonclinical staff to free PCP time and energy for new, higher value activities. This is exactly what the Bruyère Academic FHT has done to increase adoption of eConsult use by their PCPs. This type of approach can be tailored to meet the various workflow processes utilized by the clinics to manage referral requests and therefore can take on a different appearance.
The growing adoption of eConsult is an example of a disruptive innovation, where utilization of an innovative product is driven by its ability to address previously unmet needs. 15 Such innovations typically align and blend with a pre-existing technology infrastructure. In the case of eConsult, certain vendors are already known to integrate eConsults and templates directly into the existing infrastructure of electronic health records (EHR)/EMRs, 16 whereas others are partnering with eConsult platform providers to enable such integration. 17 There are, however, several barriers to having eConsult embedded in an EMR, most notably a reliance on vendors, delays in product development, and often prohibitive costs. In addition, although some eConsult systems are integrated into EMRs, at present these are limited to settings where the PCPs and specialists share a common EMR, which is not typical in most jurisdictions. Finally, as already emphasized, there is a need to better understand which EMR features contribute to stress and burnout to help predict unintended consequences and offer opportunities to optimize EMR features that complement and enhance physician work life. 6,14
Alternatives to EMR/EHR integration have not been studied, hence, our study is very unique in that it demonstrates (1) a different solution to the issue of integration and (2) positive deviance as an approach to support health care transformation that focuses on identifying innovative practices to achieving the desired outcomes (e.g., in this case improving the much needed access to specialty care) and using those practices to guide transformative change. The premise of this approach is that solutions to common problems mostly exist within clinical communities, which have tacit knowledge that can be generalized and tend to be more readily accepted and feasible within existing resources, thus increasing the likelihood of success and, potentially, expansion. 18 The Bruyère Academic FHT demonstrated positive deviance for improving access to specialist expertise by using a delegate model to harmonize eConsult requests within their existing, well-established workflow for processing referrals, without the need for awaiting vendors to facilitate technical integration into the clinic EMR, which also adds cost and complexity. As a result, eConsults from the Bruyère Academic FHT accounted for 10% of all eConsult cases submitted during the study period by providers from 484 clinics. The clinic reported that access to the eConsult service has reduced a backlog of conventional referrals by helping direct difficult referrals to the appropriate specialist.
Health care today is delivered in complex uncertain settings, with time-pressured and resource-constrained providers who are often in a state of inertia and hesitant to adopt new practices. 19 Studying positive deviance offers a greater understanding of practices that can bring on positive change and allow organizations to achieve top performance. Spreading the success stories involving the behaviors, processes, and systems contributing to better care is of key importance from a policy perspective. In fact, perhaps it is time to move research to action and make it obligatory for regulatory bodies to use positive deviance to improve the quality of our health care.
Our study has limitations that need to be acknowledged. It is a single-clinic study of a motivated group of providers, where there was a well-functioning process in place to allow providers to obtain conventional referral consultations, and thus, the results may not be generalizable.
Conclusions
Harmonizing eConsult requests within the existing referral workflow processes at the Bruyère Academic FHT enabled rapid uptake of a new, innovative service. Active engagement of PCPs and the clerical team enabled the clinic to implement eConsult in a locally adapted manner. Our findings show a very high level of eConsult use, which persisted throughout the study period. This approach was successful in that it allowed the PCPs to request eConsult using a familiar process, avoiding the challenges associated with adopting a new and unfamiliar technology.
Footnotes
Acknowledgments
The authors thank the primary care providers and clinic staff at the Bruyère Academic Family Health Team for supporting and using the service, and Justin Joschko for his assistance in editing the article and preparing it for publication. Funding for this project was provided by the Canadian Institutes of Health Research. The authors affirm their independence from the funders. The funders played no part in the study design, collection, analysis, or interpretation of the data, in the writing of the report, or in the decision to submit the article for publication.
Disclosure Statement
No competing financial interests exist.