
Abstract
Background:
Remote home blood pressure monitoring (RBPM) has been shown as effective in managing hypertension in underserved areas. Effects on urban patients, who are more easily provided with high-quality medical services, are still unclear. We systematically review previously published randomized controlled trials on the effect of RBPM for urban hypertensive patients.
Methods:
We searched electronic databases for studies published in English up to October 2018. Studies comparing the use of RBPM to face-to-face care were included. Outcome measures were changes in office blood pressure (BP) and the rate of BP control.
Results:
We identified 1,433 potential references for screening, of which 27 were eligible for review. Substantial heterogeneity was evident for the investigated variables. A significant standardized mean difference (SMD) was observed for RBPM for systolic BP, but the effect size was small compared to face-to-face care and was clinically irrelevant in avoiding cardiovascular events (0.212, 95% confidence interval 0.148–0.275; p < 0.001). For diastolic BP, the SMD between the two groups was small (0.170, p < 0.001) and the effect of RBPM was irrelevant in preventing cardiovascular events. The effect on the rate of BP control was significantly high for the intervention group (relative risk: 1.136; p = 0.018).
Conclusions:
This review demonstrates that RBPM performed on urban hypertensive patients has limited value and seems not to be superior to ordinary care in avoidance of cardiovascular events. Further studies are needed to provide more reliable information about the effectiveness of RBPM in preventing hypertensive cardiovascular complications.
Introduction
Hypertension is a common cause of morbidity and mortality and a major risk factor for cardiovascular disease. However, not all patients with this chronic medical condition have blood pressure (BP) medically controlled at the recommended level. 1 –3 The standard for BP control for hypertensive patients has recently been strengthened according to the 2017 ACC/AHA guidelines. 4 The standards for remote home blood pressure monitoring (RBPM) have also been reinforced with respect to controlling BP. Accurate measurement and control of BP at a medical institution are sometimes difficult, as high BP may be masked or the white-coat effect overlooked. 5 Self-measurement and remote monitoring of home BP can help overcome these difficulties and provide advantages in the management of hypertension and prediction of complications. 6 –8
In conjunction with RPBM, aiding patients through telemedicine has been suggested as a potential solution for those lacking adequate care. In some randomized controlled trials (RCT) for hypertensive patients, RBPM is reported to be effective with respect to clinical validity, cost, and time. 9 –15 There are also studies that show limited effects of RBPM in urban areas, where access to medical care is satisfactory; it has been reported that these might be due to the abundance of medical resources and well-established face-to-face care system. 16 –19
Yet, there is a lack of both integrated clinical validity and clear scientific evidence of RBPM as a sustainable policy decision in urban regions. RBPM is a health care service in which patients' biologic information is transmitted in environments where distance is crucial. 18,20 It helps making accurate diagnosis and proper treatments of hypertension and also reduces the possible limitations arising from office care of patients in medically underserved areas. 19,21 Thus, this article hypothesizes that in urban environments, where patients reside in relative proximity to the relevant clinical settings, the effects of BP control of RBPM and the impact for avoiding cardiovascular complications of hypertension may not be superior to the usual care (UC).
To test the hypothesis above and to determine the direction for evidence-based practice in urban areas, well-designed RCT need to be selected and synthesized their results using a reliable methodology. Systematic reviews and meta-analyses are transparent and rigorous methodological tools that have been settled as the cornerstones of evidence-based clinical practices. 22 Thus, we aim to examine the effect of RBPM in hypertension management in urban contexts through a systematic review and meta-analysis of studies focusing on systolic blood pressure (SBP), diastolic blood pressure (DBP), and target BP.
In this study, we analyze the effects of urban telemedicine for the benefit of policymakers, who must allocate finances efficiently and formulate effective strategies in accordance with the global trend toward urbanization. We also provide perspectives on the direction of the future of telemedicine in treatment of hypertensive patients.
Methods
Searching for Eligible Studies
This meta-analysis was performed according to the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Intervention 23 and the protocol for this study was previously published. 24
To identify eligible studies, electronic databases such as EMBASE, EBSCOhost, the Cochrane Library, ProQuest, and Medline through PubMed were scanned. The authors searched for articles, published in English, in peer-reviewed journals from inception to the end of October 2018. In addition, we manually searched previous meta-analyses related to the topics of the obtained studies. 9,17,25,26 Additional searches were conducted of clinical trial registers such as the Meta-Register of Controlled Trials, the U.S. National Institutes of Health ongoing trials register. Two independent reviewers (W.S.C. and J.O) scrutinized all data resources and selected free terms and Medical Subject Headings (MeSH) terms related to hypertension, RBPM, urban population, and RCT. Utilizing Boolean operators, we built a search strategy for each database (Appendix A1).
Inclusion and Exclusion Criteria
Controlled trials were included in which two subject groups were randomly assigned: the RBPM group and the UC group. In these studies, urban patients older than 17 years, who were able to measure their own BP at home, were included. In addition, their hypertension was managed at urban medical institutions. Data were included, which were transmitted to remote medical providers by telephone, the internet, mobile phones, and letters. Cases were included in which patients with hypertension were compared pre-results and post-results of RBPM. However, the following cases were excluded: if the area in which each study was conducted was not a city; where urban and rural patients were combined; if medical professionals visited the patients' households or if the patients willingly visited the hospital for track monitoring; and cases in which the effects of different interventions were compared based on remote monitoring.
The main outcomes targeted mean differences in SBP and DBP between baseline measurements and follow-up points and the target BP achievement rate.
Study Selection Process and Data Extraction
The abstracts and references of the articles retrieved for this study were imported to the Endnote X8 software (Thomson Reuters, Philadelphia). To remove extraneous articles and duplicates among the retrieved materials, two reviewers (W.S.C. and J.O.) independently screened the titles and the abstracts before analysis. Potentially eligible studies were then extracted and the full text was reviewed for further scrutiny. Two reviewers (I.-S.S. and J.-S.Y.) independently selected the relevant primary studies that were to be included in the meta-analysis.
Two researchers (J.H.C. and J.O.) independently extracted data from the selected primary studies and entered them into an electronic spreadsheet. We coded the measured BP values using an automated electronic sphygmomanometer; for entries in which an ambulatory BP monitor was used, the mean BP values at each step were extracted. If BP and the corresponding standard deviation (SD) values were not reported or could not be calculated from the 95% confidence intervals (CI), we attempted to make contact with the authors or obtained the necessary data through the relevant websites. In some studies, this was not feasible or SD data were missing; in these cases, 5,27 –30 the average of the SDs of all remaining studies was calculated 25 and utilized in the analysis. Using the relative risk (RR), we estimated the effect of intervention by calculating the ratio of patients who had reached their target BP at the time of final follow-up.
If there were multiple follow-up durations within a study, this study was included in the meta-analysis as an independent primary study that corresponded to the study of intervention effects at different follow-up periods. 31 –36 Issues for which there was no consensus among the researchers were resolved by discussion with the senior authors (I.S-.S. and J.-S.Y.).
Quality Assessment
The quality of the methodology in the primary studies included in this analysis, including the risk of bias, was assessed by two authors (W.S.C. and J.O.) according to the guidelines from the RevMan meta-analysis software (version 5.3.5) for Windows (Copenhagen: The Nordic Cochrane Center, 2014) by the Cochran Collaboration. 23
Statistical Analysis
The data analysis was conducted by two authors (W.S.C. and I.-S.S.). As each study's population is heterogeneous, the random effect model was adopted for the meta-analysis. The Comprehensive Meta-Analysis software (Biostat, NJ) was used to perform the analysis. Weighted mean differences (WMD) were used to calculate average changes in the mean differences in SBP and DBP, which were measured using office BP. The RR, which was estimated by extracting BP target achievement data, was used to compare the dichotomous variables. All results were reported with a 95% CI. To determine the effect size, the standardized mean difference (SMD) was determined by applying the rule of thumb. 37 Differences between studies were assessed using the χ 2 test and p < 0.10 was indicated to be statistically significant. Heterogeneity was quantified using the I 2 statistic and the values were assessed using the rule of thumb. 38 Thus, if I 2 was over 50%, it was accepted as being significantly heterogeneous in our study. 37 The effect of each trial on the overall outcomes was also assessed. To determine material quality, a sensitivity test was conducted. A further sensitivity analysis was performed to test for differences between when studies with the missing values imputed were included and when they were not included.
Results
Study Characteristics
In total, 1,433 references were retrieved through searching databases, making contact with authors, and other electronic sources. First, the titles and abstracts of these references were screened to exclude 817 duplicates and identify 616 citations. Four hundred ninety more articles were excluded as unsuitable for the analysis, leaving a total of 126 potentially eligible publications. Among these, 54 studies did not involve remote monitoring, 28 had no data available, 12 were ongoing studies, 3 described the trial design only, and 2 concerned remote monitoring programs of other diseases; these were all excluded. As the 34 comparisons included in the final 27 independent studies fit the inclusion criteria, these were selected as the target materials for inclusion in this meta-analysis (Fig. 1). The main characteristics of the included studies are summarized in Table 1.
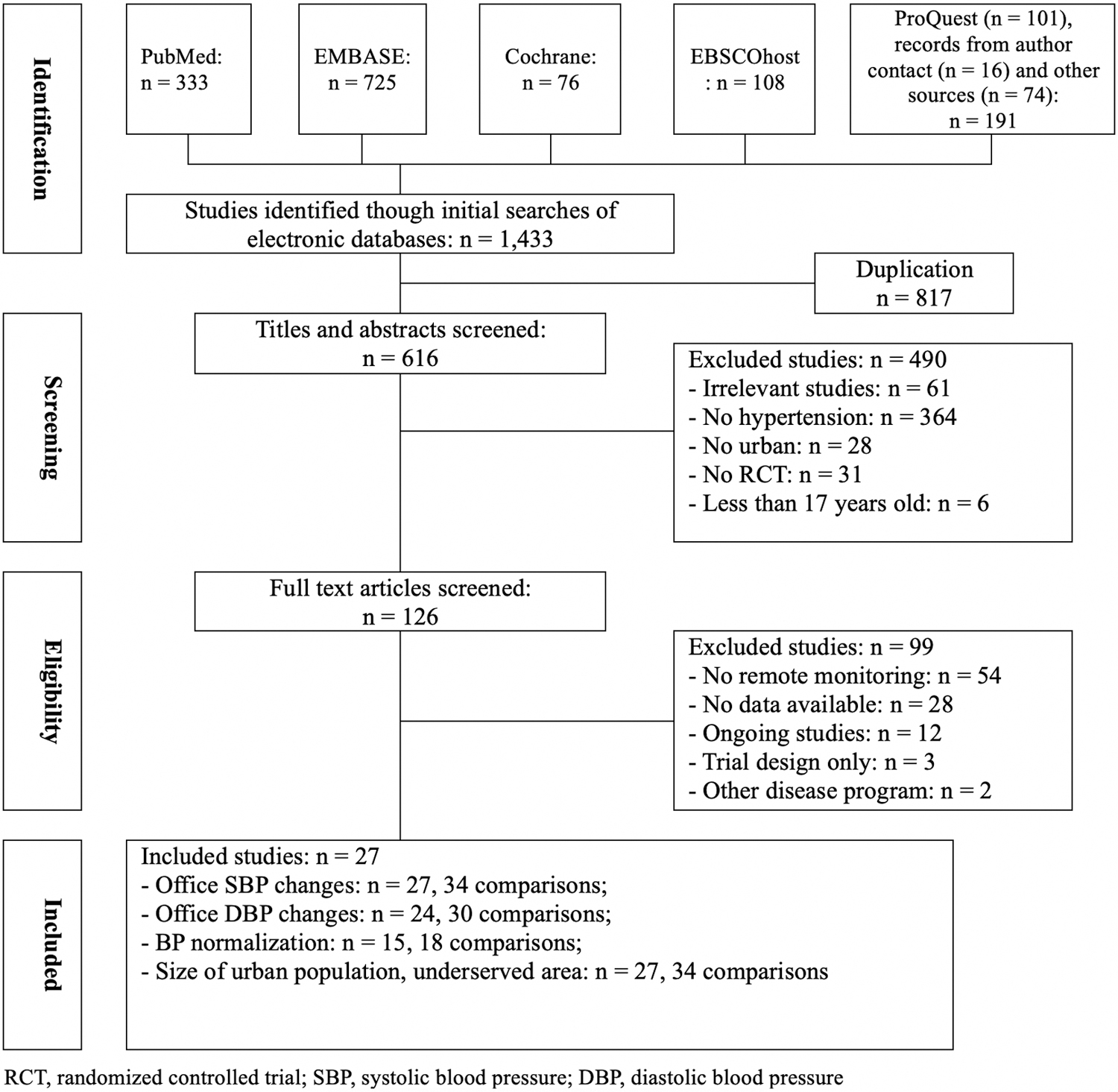
Flow diagram of selection of studies included in the meta-analysis.
Characteristics of Included Studies in the Meta-Analysis
ABPM, ambulatory blood pressure monitoring; BMI, body mass index; BP, blood pressure; DBP, diastolic blood pressure; RBPM, remote home blood pressure monitoring; SBP, systolic blood pressure.
A, B, and C represent different periods of time within the same study.
The overall average length of follow-up was 7.56 months. The mean age was 60.7 years for the control group and 60.3 years for the intervention group. Differences in gender and baseline BP were not significant.
Risk Assessment
For most studies, the selection process (e.g., random sequence generation or allocation concealment) was properly performed and adequately reported. The degree of risk caused by reporting and attribution bias was either high or unclear for most studies.
The publication bias for office SBP was checked using the trim-and-fill method. 55 Although the data distribution of the observed funnel plot showed good symmetry visually, three studies were imputed, and some studies may have remained unpublished due to the limitations of trials with small sample sizes (Fig. 2). The SMD was 0.212 (0.148–0.276) based on the funnel plot and the average imputed value was statistically significant (0.184, 0.112–0.255). The funnel plot for office DBP showed good symmetry; for this variable, no imputed values were included in the plot (SMD = 0.170) (Fig. 3). Therefore, we conclude that publication bias had no significant effect on the primary outcomes of the studies included in this analysis, and the presence of imputed values for missing studies had no substantial effects on our study's results.
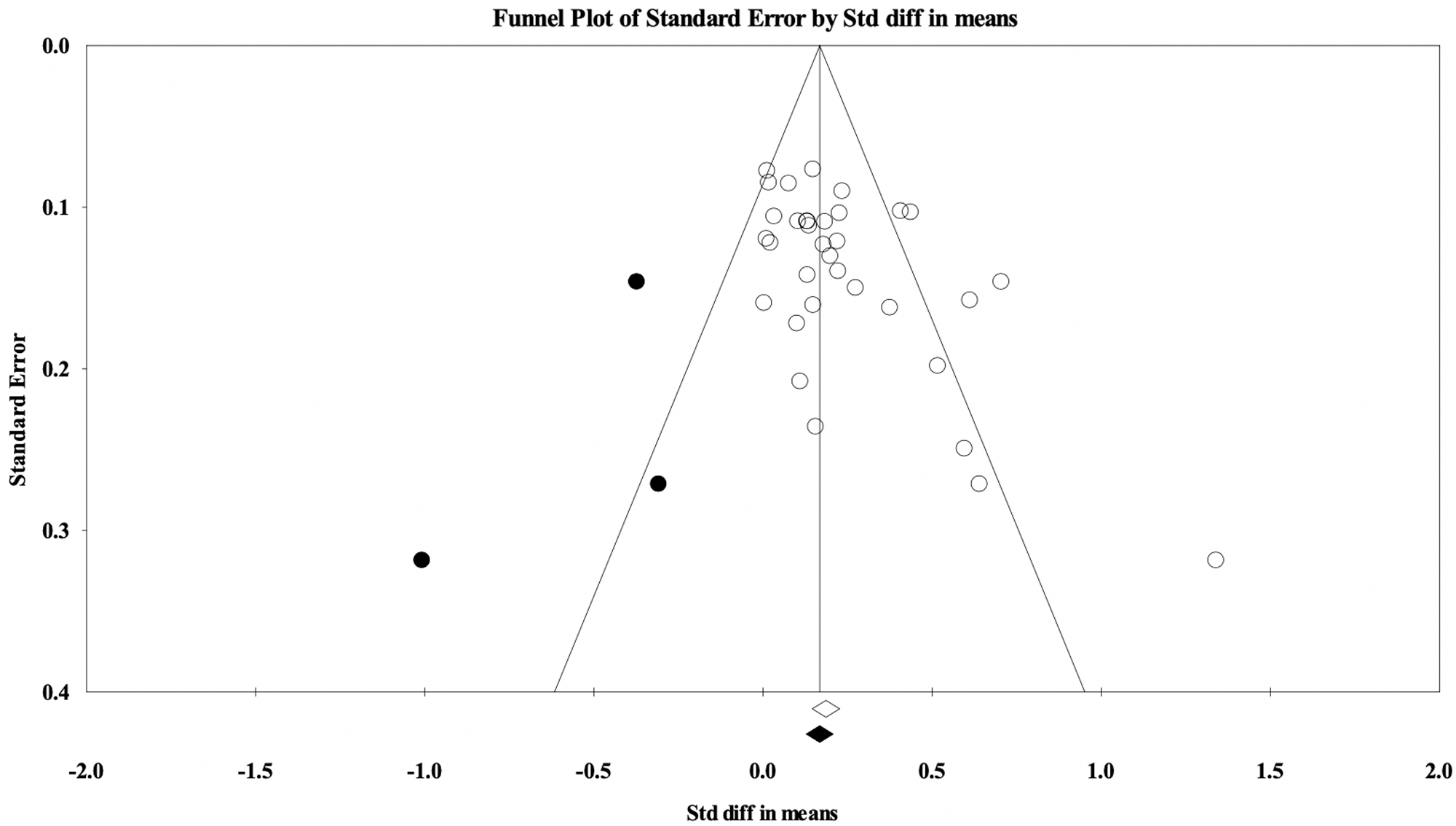
Funnel plot of SBP by standardized difference in means (plot observed and imputed). SBP, systolic blood pressure.

Funnel plot of DBP by standardized difference in means (plot observed and imputed). DBP, diastolic blood pressure.
The publication bias for the rate of office BP control showed good visual symmetry in the funnel plot with an RR value of 1.136 (1.022–1.264). No studies had imputed values, and the adjusted value was the same (Fig. 4).

Funnel plot of rate of BP control by relative risk (plot observed and imputed). BP, blood pressure.
Outcomes
Changes in BP
In total, differences in SBP for 9,435 patients from 27 RCT studies (34 comparisons) were assessed, including 4,717 from the RBPM group and 4,718 from the UC group. 5,15,27 –29,31–36,39 –54 Although the summary WMD in SBP was significant between the two groups (3.482 mmHg, 2.459–4.505; p < 0.001), the SMD was small (0.212, 0.148–0.275; p < 0.001) (Fig. 5). Heterogeneity between the studies was significantly high (I 2 = 58.904%; p < 0.001). In the sensitivity analysis, no significant difference in the summary point estimate of the study outcomes was found.
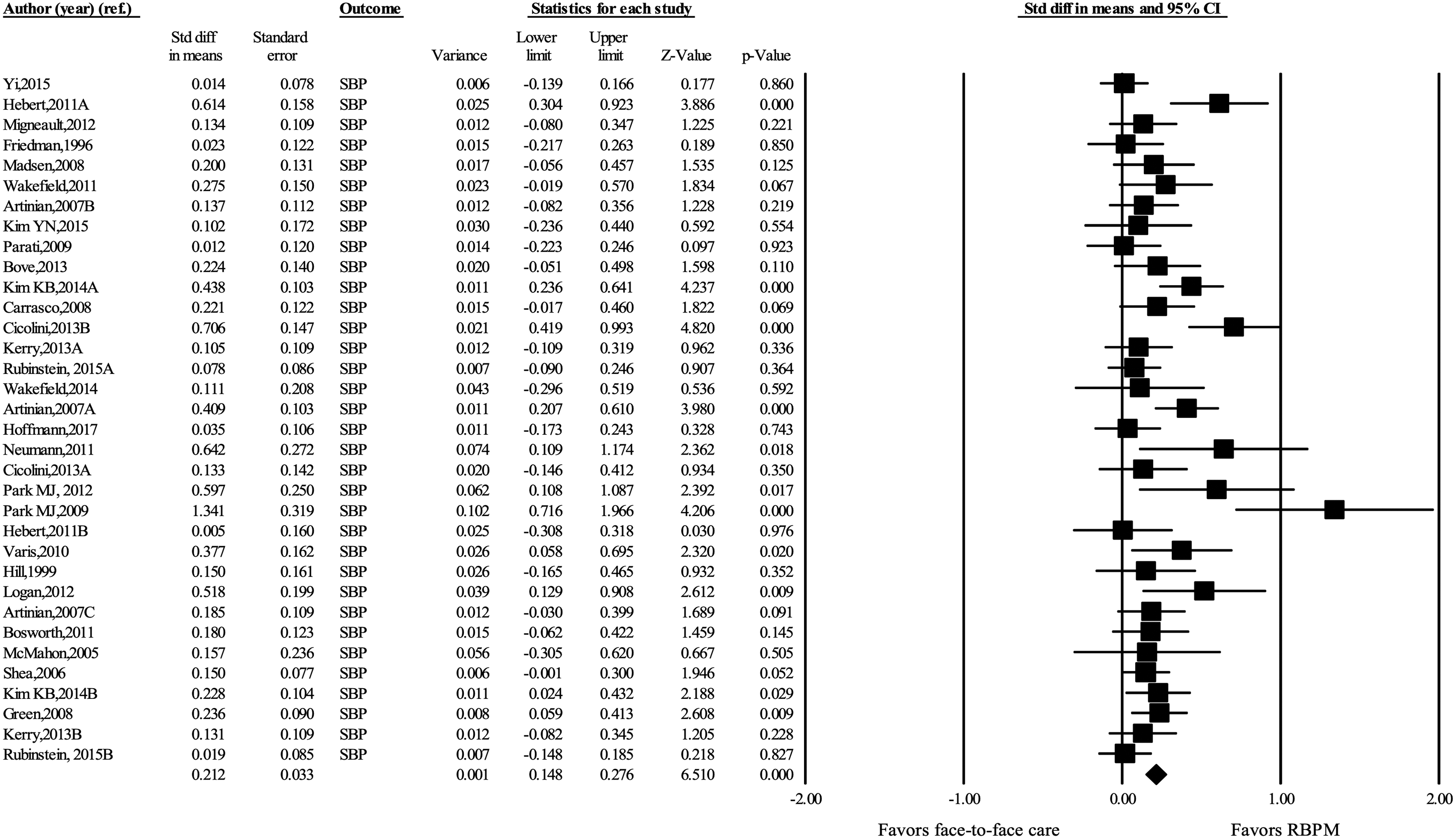
Standardized mean difference in office SBP changes. RBPM, remote home blood pressure monitoring.
To determine the mean difference in DBP, data for 8,522 patients, including 4,278 from the RBPM group and 4,244 from the UC group, were extracted from 24 available studies (30 comparisons). 5,15,27,28,31 –33,35,36,39 –52,54 The reduction in DBP was significantly greater in the group randomized to RBPM (1.638 mmHg, 1.084–2.192; p < 0.001) (Fig. 6), but the clinical significance of this finding was minimal and the SMD was also small (0.170, 0.111–0.228; p < 0.001). Heterogeneity between studies was significant (I 2 = 42.310%; p < 0.001). A sensitivity analysis was carried out to test for the effect of removing studies, which was not significant.

Standardized mean difference in office DBP changes.
BP normalization rate
We determined the achievement rate associated with RBPM based on the BP values previously set in each primary study. BP control events were reported in 15 studies (18 comparisons) that involved a total of 4,955 individuals, including 2,515 from the RBPM group and 2,440 from the UC group. 5,15,28,32,33,35,40 –42,44–46,48,52,54 In comparison to the UC group, the rate of normalization of BP for the RBPM group showed a significantly larger improvement (45.05 vs. 38.42%; RR: 1.136; 1.022–1.264; p = 0.018) (Fig. 7) and heterogeneity was significant in these studies (I 2 = 58.848%; p < 0.001). In the sensitivity analysis, the summary point estimate was unchanged.

Risk ratio of BP control.
Subgroup Analysis
City size
Changes in the intervention group's office SBP were compared among 34 comparisons, according to the size of the cities in which the trials were conducted (Fig. 8). WMD in studies of 16 small- to medium-sized cities 27 –29,31,35,39,42 –44,46–48,52 was 3.765 mmHg (2.271–5.258; p < 0.001) and the value was 3.229 mmHg (1.839–4.618; p < 0.001) in studies of 18 larger cities. 5,15,32 –34,36,40,41,45,49 –51,53,54 Heterogeneity between studies was significant (I 2 = 58.904; p < 0.001). The intervention was therefore more effective in smaller cities compared to larger cities.
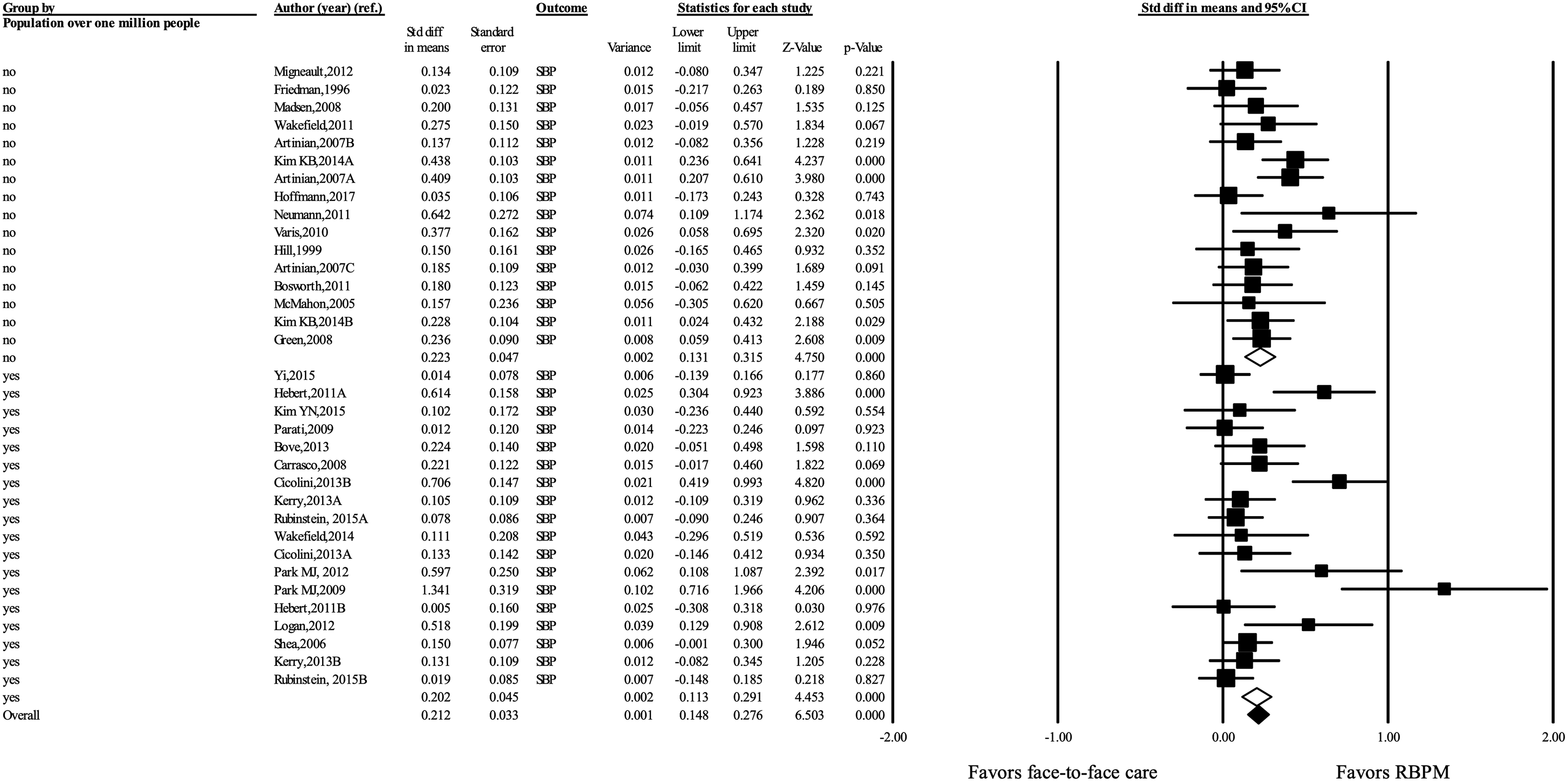
Standardized difference in means of SBP changes by population over 1 million people.
In 18 available studies, where data were reported, the rate of normalization of BP was higher for larger cities. The RR in small- to medium-sized cities 42,44,46,48,52 was 0.996 (0.788–1.259; p = 0.974) and the point estimate from the 10 studies (13 comparisons) targeting larger cities was 1.175 (1.045–1.323; p = 0.007). 5,15,28,32,33,35,40,41,45,54 Overall heterogeneity was significant (I 2 = 58.848; p = 0.001).
Medically underserved areas
In 9 studies (14 comparisons), 28,31,33,35,36,40,43,51,54 including 2,654 people in medically underserved areas, the effect of RBPM on office BP was assessed (Fig. 9). Although the WMD for intervention showed a significant change of 3.542 mmHg (1.965–5.119; p < 0.001), the SMD was small (0.188, p < 0.001). In 18 studies (20 comparisons), 5,15,27,29,32,34,39,41,42,44 –50,52,53 including 2,065 people, there was no mention of medically marginalized areas. In this group, the mean difference in BP due to intervention was 3.456 mmHg (2.077–4.835; p < 0.001) and the SMD was below the median (0.235, p < 0.001). Heterogeneity among these groups was significant (I 2 = 58.904; p < 0.001). The reduced WMD of SBP was 2.978 mmHg (1.739–4.217; p < 0.001), showing relatively high heterogeneity (I 2 = 62.272; p < 0.001). Therefore, the effect of remote monitoring of BP within cities was similar regardless of the medically underserved areas.
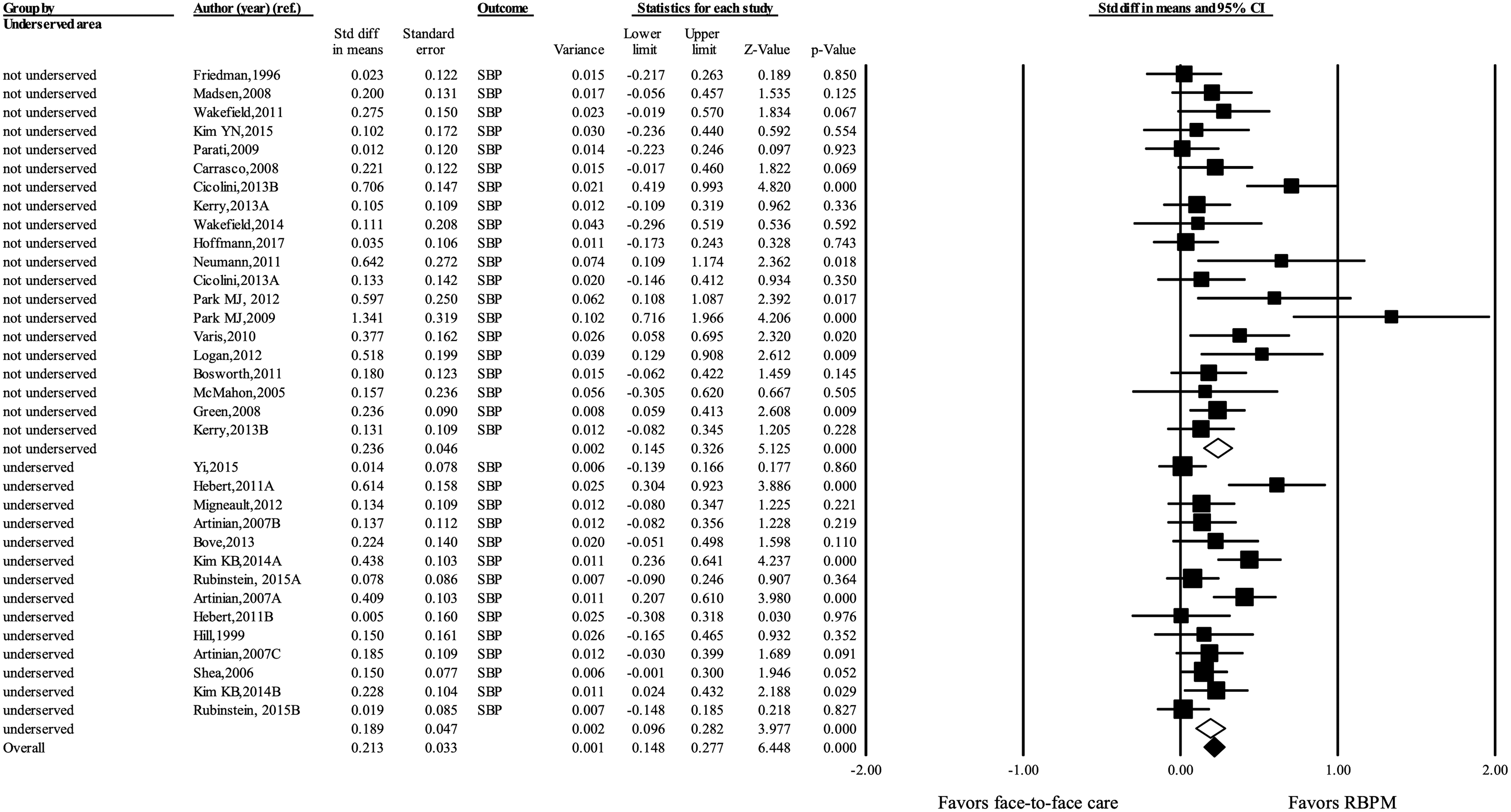
Standardized difference in means of SBP changes by underserved area.
Discussion
This review analyzed the effects of RBPM on outcomes for adult patients with hypertension living in cities with easily accessible and high-quality medical care. To assess the effects of RBPM quantitatively compared with patients receiving face-to-face care, we conducted a systematic analysis, including a reasonable amount of data from previously published RCT studies.
The effect of RBPM intervention was statistically significant. However, if the goal of intervention is to prevent cardiovascular complications, then the difference from the control group (3.482 mmHg SBP and 1.638 mmHg DBP, respectively) in our analysis is not relevant from a clinical standpoint. This is especially true when we consider that publication bias was taken into account. In a large-scale meta-analysis of 67,457 patients, a decrease in SBP of 4 mmHg is reported to have <5 people out of 1,000 (0.5%), compared to the baseline, avoid cardiovascular events and in the case of 2 mmHg reduction in DBP, 6 out of 1,000 patients. 56 The results show an SMD of 0.212, which also weakens the evidence for the effectiveness of this treatment. The RBPM group in the meta-analysis of Omboni and Guarda 8 showed a significant reduction in office BP (SBP 5.64 mmHg; DBP 2.78 mmHg; n = 4,389), but for such a significant reduction, other interventions must have accompanied RBPM. In other studies, 15,57 it was reported that significantly high fees were necessary to achieve a significant RBPM effect (over €662.92/patient). Our results therefore indicate that the reduction in BP due to RBPM in urban hypertensive patients is negligible, even after correcting for labor and costs. We therefore do not recommend this treatment as a sustainable useful tool in this setting.
However, the results differ for achievement rates. That is to say, the larger the city, the higher the achievement rate for target BP. Thus, RBPM in urban areas seems to have limited effects in preventing complications of hypertension. The results of this meta-analysis on RBPM have different implications to those of previous meta-analytic studies 10,17,26 that failed to distinguish between urban and rural areas and reported that RBPM reduces BP and thus helps prevent cardiovascular disease.
We classified city size by introducing the concept of metropolis (i.e., urban areas with a population of over 1 million). The populations included in this study were based on census data from each country at the time of each study. The intervention effect in small- to medium-sized cities was greater than in the larger cities (3.765 mmHg vs. 3.229 mmHg). This implies that the effects of telemedicine can be limited in large cities where high-quality health care is easily accessible.
The difference in effects of telemedicine for the purpose of improving accessibility to medical care was not clinically significant in underserved areas within cities (about 3.542 mmHg vs. 3.456 mmHg). This may be due to the low socioeconomic and education levels of the residents in marginalized areas or low awareness of health care options such as monitoring devices. 58,59
The establishment of policies related to telemedicine according to city size, even in areas with limited finances, can improve outcomes. Previous meta-analyses did not focus on the effects of RBPM in urban hypertensive patients or the effects of remote monitoring in medically underserved urban areas with consideration of city size. To the best of the authors' knowledge, this study is the first meta-analysis to evaluate the effects of RBPM in urban hypertensive patients. In this study, we expanded the contextual understanding of RBPM by exploring significant moderators.
Our study has the following limitations, despite the transparency of its systematic process, in which objective statistical methods were used and the effect of publication bias was nonsignificant. First, there was no detailed analysis of marginalized areas. This omission may have caused conceptual errors related to the medically underserved areas within the cities included in the analysis. To overcome this limitation, a categorical approach to various factors such as the residents' ethnicity, socioeconomic status, and education level may be necessary. Second, there are difficulties in generalizing the achievement rates of target BP, as different studies apply different standards for the severity of hypertension and the target control level. Careful selection using international standards would increase the reliability of the study outcomes. Third, although this research was conducted using various combinations of MeSH terms and free terms, this strategy is not perfect; some potentially relevant studies may be missing. The robustness of the study may be improved through additional updates.
Conclusions
The results of this study reveal that RBPM, performed in the city, does not provide clinically significant benefits over ordinary office-based hypertension management. Although the RBPM group shows a significant reduction in BP compared to the UC group, this difference is not relevant for satisfactory prevention of cardiovascular events.
To obtain even more robust results, future researchers must examine the duration of the intervention delivered, categorizing cities by size and further investigating the usefulness of RBPM in analyses that consider costs, manpower, and government efforts.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was receiving for this study.