
Abstract
Background:
Electronic consultation (eConsult) services have been shown to reduce the need for face-to-face consultations. The largest expense is remunerating the specialist.
Introduction:
The Champlain BASE™ eConsult service remunerates specialists based on their self-reported billing time. It is important for funders of eConsult systems to understand and plan for specialist remuneration. This study examined specialists' time commitments pertaining to eConsult, identified factors that affect their self-reported billing time, and determined if self-reported billing time is associated with changes in primary care provider (PCP) behavior.
Methods:
A cross-sectional study of eConsults was completed between January 1 and December 31, 2017. Data were collected automatically by the service and through mandatory closeout surveys. Logistic regressions identified associations between specialists' self-reported billing time and volume of cases completed, PCP characteristics, specialty group, impact on PCP behaviors, and PCP satisfaction.
Results:
A total of 11,985 cases met inclusion criteria. Self-reported billing time was <5 min in 18.3% of cases, 5–10 min in 35.6%, 10–15 min in 27.3%, 15–20 min in 11.3%, and >20 min in 7.5%. Self-reported billing time demonstrated significant variation between specialty groups. Cases with higher self-reported billing time were more likely to lead to new/additional course of action for PCPs (p ≤ 0.0001), resulted in fewer referrals (p ≤ 0.0001), and received higher rankings for helpfulness and educational value (p ≤ 0.0001).
Discussion:
A thorough understanding of when and how specialists respond to eConsult cases is critical to ensuring the service's long-term sustainability. Examining these factors and their impact on PCP behaviors helps us to better understand the service's overall value and serve to inform the structure of its remuneration process.
Conclusions:
Specialists' self-reported billing time varies by specialty group and is associated with changes in PCP behavior and satisfaction. Further research is needed to identify what factors influence self-reported billing time and how eConsult can be best incorporated into clinicians' workflows.
Introduction
An electronic consultation (eConsult) service is a secure online platform that allows primary care providers (PCPs) and specialists to communicate electronically regarding a patient's care, to improve access and avoid unnecessary referrals. In recent years, multiple organizations in Canada, the United States, and Europe have implemented eConsult services with the goal of improving timely access to specialist advice. 1,2 eConsult services have shown value across the quadruple aim of improved population health, lower costs, greater provider satisfaction, and better patient experience. 3 –5
Cost considerations are a critical part of implementation and sustainability planning for eConsult services. 6 Specialist remuneration is the main cost driver in established eConsult services and, thus, an important factor when planning how to sustain pilot services. Payment schemes for specialists vary across the organizations that have implemented eConsult services, including flat fee-for-service (Alberta Health Services), use of salaried specialist physicians (San Francisco General Hospital), workload “credit” (Mayo Clinic; Veteran Affairs), and prorated hourly reimbursement (Champlain BASE™). 7 The decision of how to structure remuneration is influenced by various factors, including how specialists are paid for face-to-face visits (i.e., fee-for-service vs. salaried) and whether there was opportunity for new payment methods when the services were launched, and may have implications on the amount of physicians who join the service, the quality of care it provides, and its overall cost.
In a time-based payment model, in which remuneration is prorated to the length of time a specialist spends responding to a case, an understanding of specialists' typical response time is naturally of great importance in determining the service's overall cost. However, there are other factors pertaining to specialist responses that are also important. For instance, burnout among physicians and other health care providers is a common risk when implementing new technologies and workflows. Although feedback from specialists have shown high satisfaction and value to providing eConsults, 4,8,9 many providers answer eConsults without reducing other clinical activities or responsibilities, potentially increasing workload in a manner that is neither sustainable nor healthy. An understanding of what factors affect specialists' self-reported billing time would help users integrate the service into their workflows and reduce the risk of burnout. Likewise, a longer period spent responding to a case, although more expensive, may nevertheless be preferable to a shorter response, if the extra time spent is commensurate with higher quality. If a quick response results in a face-to-face specialist referral that could have been avoided had the reply been more detailed, then the total cost of the interaction would be higher overall. A clearer understanding of the association between response time and quality would be invaluable in informing user guidelines and determining best practice.
In this study, we aimed to (1) examine specialists' time commitments pertaining to eConsult, including when they answer cases and how long it takes them to reply; (2) identify the factors that affect the length of time specialists spend responding; and (3) determine if the length of time specialists spend on their replies is associated with differences in PCP behavior, such as changes in their course of action, decision to refer, and perceived educational benefit.
Methods
Design
This is a cross-sectional analysis of all eConsults submitted to the Champlain BASE™ eConsult service between January 1, 2017 and December 31, 2017.
Setting
The Champlain Local Health Integration Network (LHIN) is one of 14 health regions in the province of Ontario, Canada. Located in the easternmost part of the province, The Champlain LHIN spans a catchment area of ∼16,000 square kilometers and includes the capital city of Ottawa. A total of 1.2 million people live in the area, mostly in urban centers. The region has comparable health outcomes and demographic characteristics to the rest of Canada. 10
The Champlain BASETM eConsult service
The eConsult service is an asynchronous Web-based application that allows a PCP to submit patient-specific clinical questions to a specialty service using a standardized electronic form. 4,11 Laboratory results or photos can be attached. The case is assigned to an individual specialist, who responds within 7 days. Specialists can request more information, provide a recommendation, or suggest a face-to-face referral. There may be back-and-forth communication between the specialist and PCP until the PCP is satisfied and closes the case.
After completing a case, physician specialists are paid $200 per hour prorated to the amount of time they spent writing their response, a value we will henceforth refer to as “self-reported billing time.” When submitting their response, specialists are asked to enter their self-reported billing time using a series of 5-min intervals between zero and 20 min. If the specialist spent longer than 20 min responding, they may indicate this but are asked to provide an explanation. If a time to respond is not indicated, a period of 25 min is assumed.
Data collection
The eConsult service routinely collects data each time an eConsult is submitted, including PCP demographic information (e.g., gender, clinic name, provider type (i.e., family physician or nurse practitioner), and postal code), the specialty service the case was directed to, the number of cases the specialist received, and the date and time of each question/response. PCPs' postal codes were used to determine their rurality, based on the Rurality Index of Ontario. Cases were excluded if they were (1) submitted by PCPs outside of the Champlain LHIN, (2) sent to specialties that had received fewer than 20 cases before the study period, (3) answered by specialists who had completed fewer than 10 cases since joining the service, or (4) marked with a self-reported billing time of zero minutes.
For the purpose of this study, we were interested in examining the association between change in PCP behavior and specialists' self-reported billing time. At the completion of each eConsult, PCPs complete a mandatory closeout survey. The PCP is asked if information from the eConsult was (1) able to confirm their original course of action, (2) able to provide advice for a new or additional course of action, (3) not very useful, or (4) none of the above (with free text field provided). A behavioral change due to eConsult was considered to have occurred if the PCP selected option two (i.e., a new or additional course of action). The PCP is also asked if the eConsult impacted on the need for a face-to-face consultation by selecting one of five options: Referral was originally contemplated but now avoided at this stage. Referral was originally contemplated and is still needed. Referral was not originally contemplated and is still not needed. Referral was not originally contemplated, but the eConsult process resulted in a referral being initiated. Other (with free text field provided).
A change in referral plans was deemed to have occurred if the PCP chose options one or four. Finally, PCPs are also asked to rank the helpfulness and educational value of the case on a scale from one (minimal) to five (very valuable).
Analysis
Descriptive statistics was generated. We used ordinal logistic regressions to determine the impact of specialists' self-reported billing time on changes in PCPs' course of action and rating of the case's educational value/helpfulness and nominal logistic regressions to determine the impact of specialists' self-reported billing time on PCPs' decision to refer. The analysis adjusted for other variables, such as volume (categorized by quartiles), PCP characteristics, and specialty. Specialists who met inclusion criteria (i.e., those who had completed 10 or more eConsult cases) were considered as random effect to account for correlation among repeated consults.
All statistical analyses were completed using SAS® software version 9.4 (SAS Institute, Cary, NC).
Results
A total of 12,220 eConsults were completed during the study period, of which 11,985 met inclusion criteria (Fig. 1). Included cases were completed by 124 individual specialists from 36 different specialty groups. Cases were submitted by 823 PCPs, of whom 695 (84.4%) were physicians, and 689 (83.8%) practiced in an urban setting.
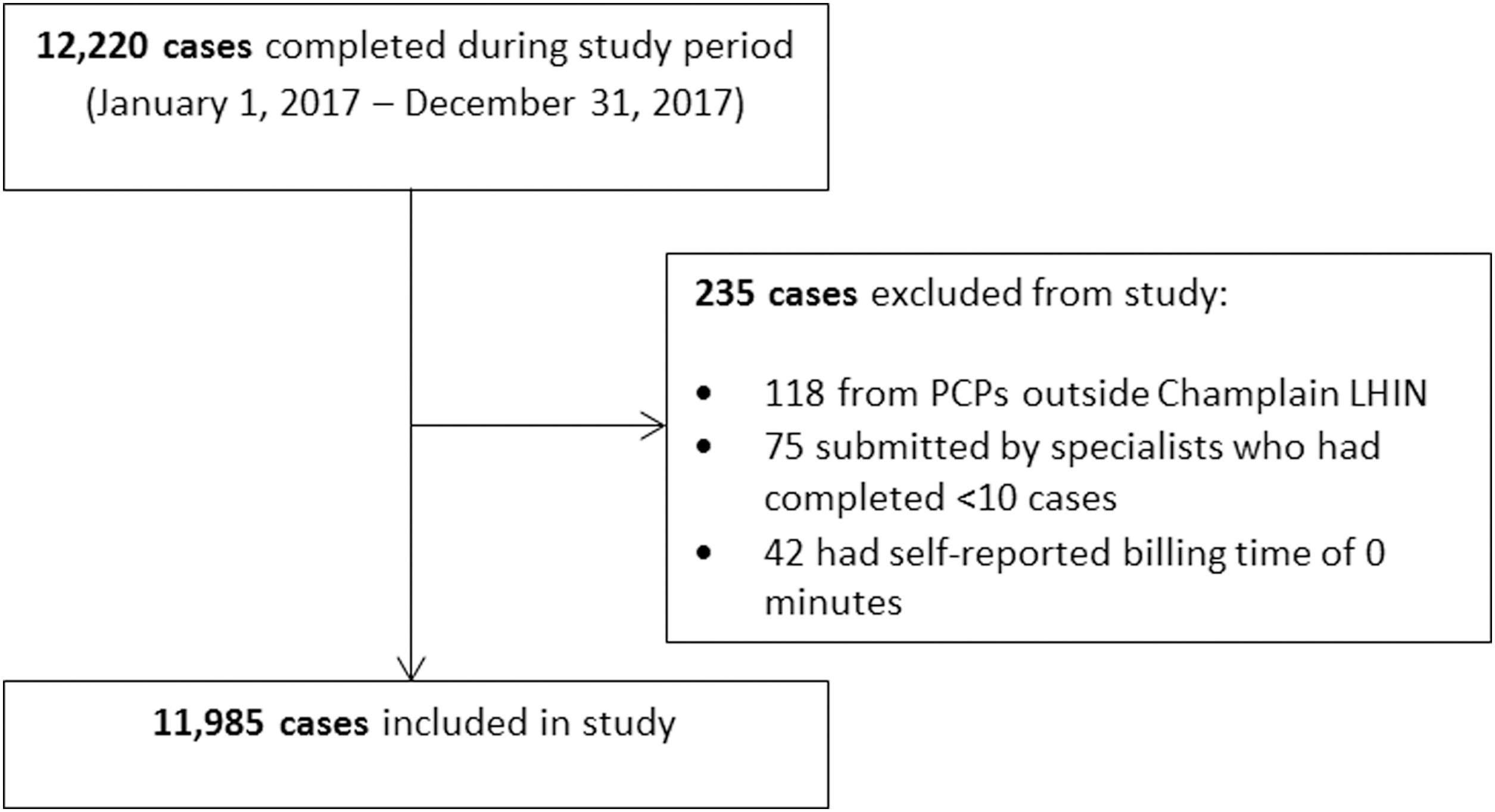
Flowchart of data collection.
The majority of eConsults were directed to dermatology (19.6%), pediatrics (10.0%), OBS/GYN (6.9%), hematology (6.6%), endocrinology (6.1%), and cardiology (5.2%). Overall, the median (IQR) number of eConsults completed by an individual specialist was 64 (28,124.5).
Self-reported billing time was less than 5 min in 18.3% of cases, between 5 and 10 min in 35.6%, 10–15 min in 27.3%, 15–20 min in 11.3%, and over 20 min in 7.5%. The median self-reported billing time was 5–10 min.
Self-reported billing time by specialty group is shown in Figure 2. Specialists answered questions throughout the week, with the majority (54%) being answered outside of a typical work day (Monday–Friday 8:00 am–5:00 pm), including 18% answered on the weekend (Fig. 3).
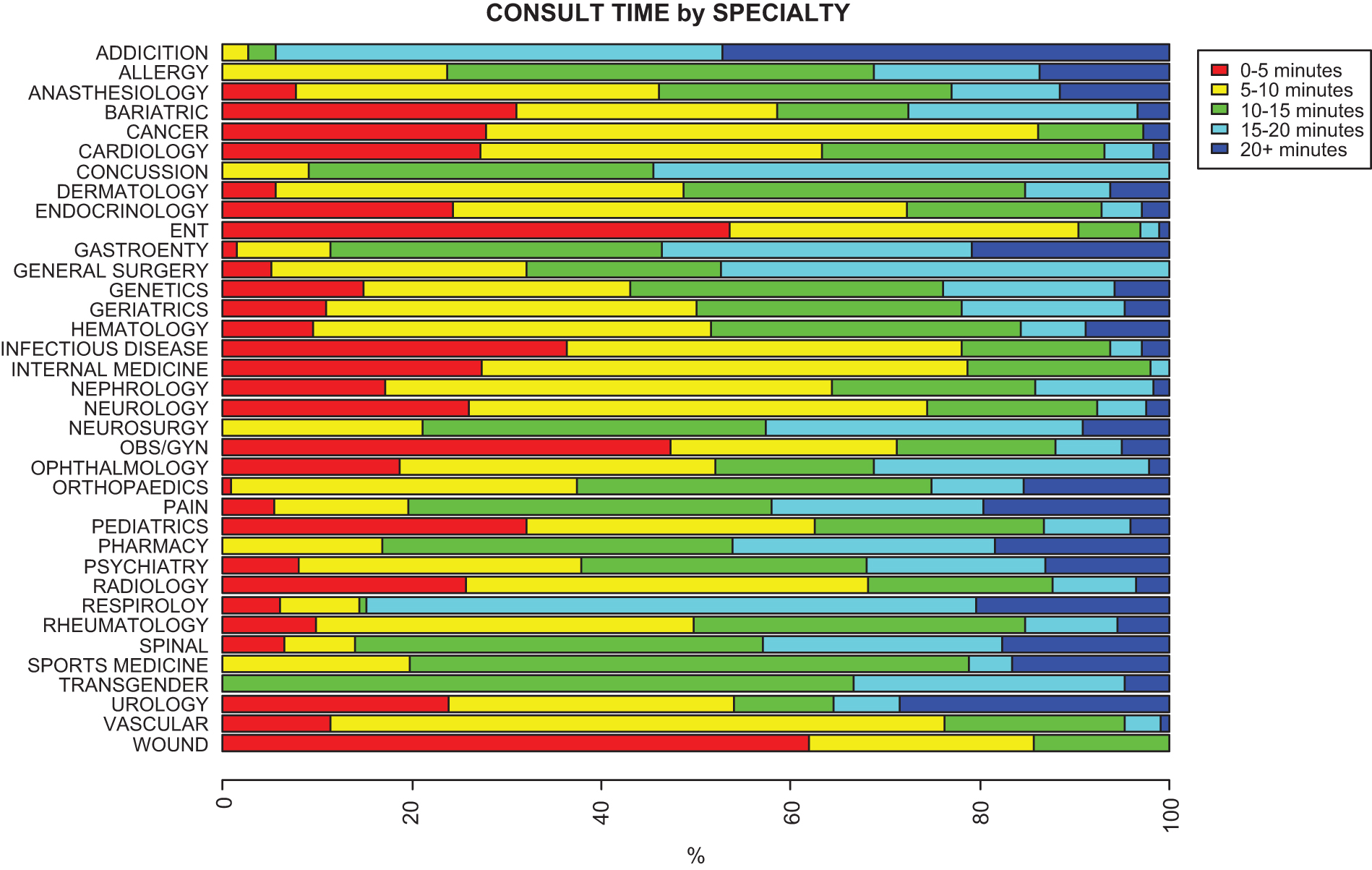
Specialists' self-reported billing time by specialty group.
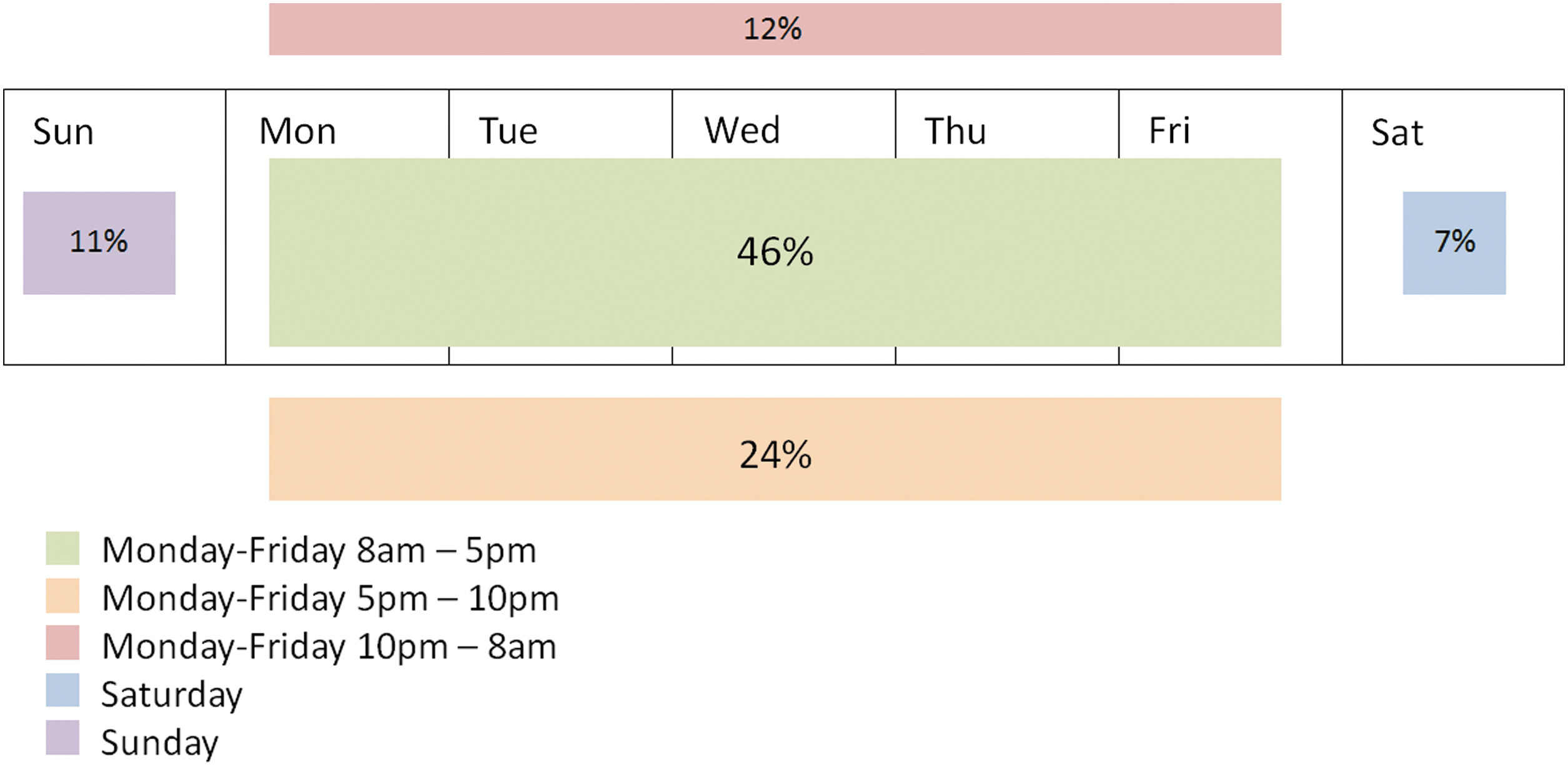
Proportion of cases answered within and outside of traditional office hours (n = 11,985).
When comparing self-reported billing time across different variables, including volume of cases the specialist completed, PCP characteristics, and specialty group, only specialty group was significant (p ≤ 0.0001). The specialties with the longest self-reported billing times were transgender, addiction, concussion, gastroenterology, and spinal services.
There was a significant association (p ≤ 0.0001) between specialists' self-reported billing time and change in PCP behavior, indicated by PCPs' reports of receiving new/additional information through the eConsult (Fig. 4). PCP characteristics (p = 0.015), specialty group (p ≤ 0.0001), and specialist time (p ≤ 0.0001) were significantly associated with changes in PCPs' decision to make a face-to-face referral. A face-to-face referral was less likely when the specialist's self-reported billing time was longer (Fig. 5). Specialist time (p ≤ 0.0001) and specialty group (p = 0.0026) were associated with educational value/helpfulness of the response. PCPs were less likely to find the advice specialists provided as highly valuable when the specialist's self-reported billing time was less than 5 min (Fig. 6).
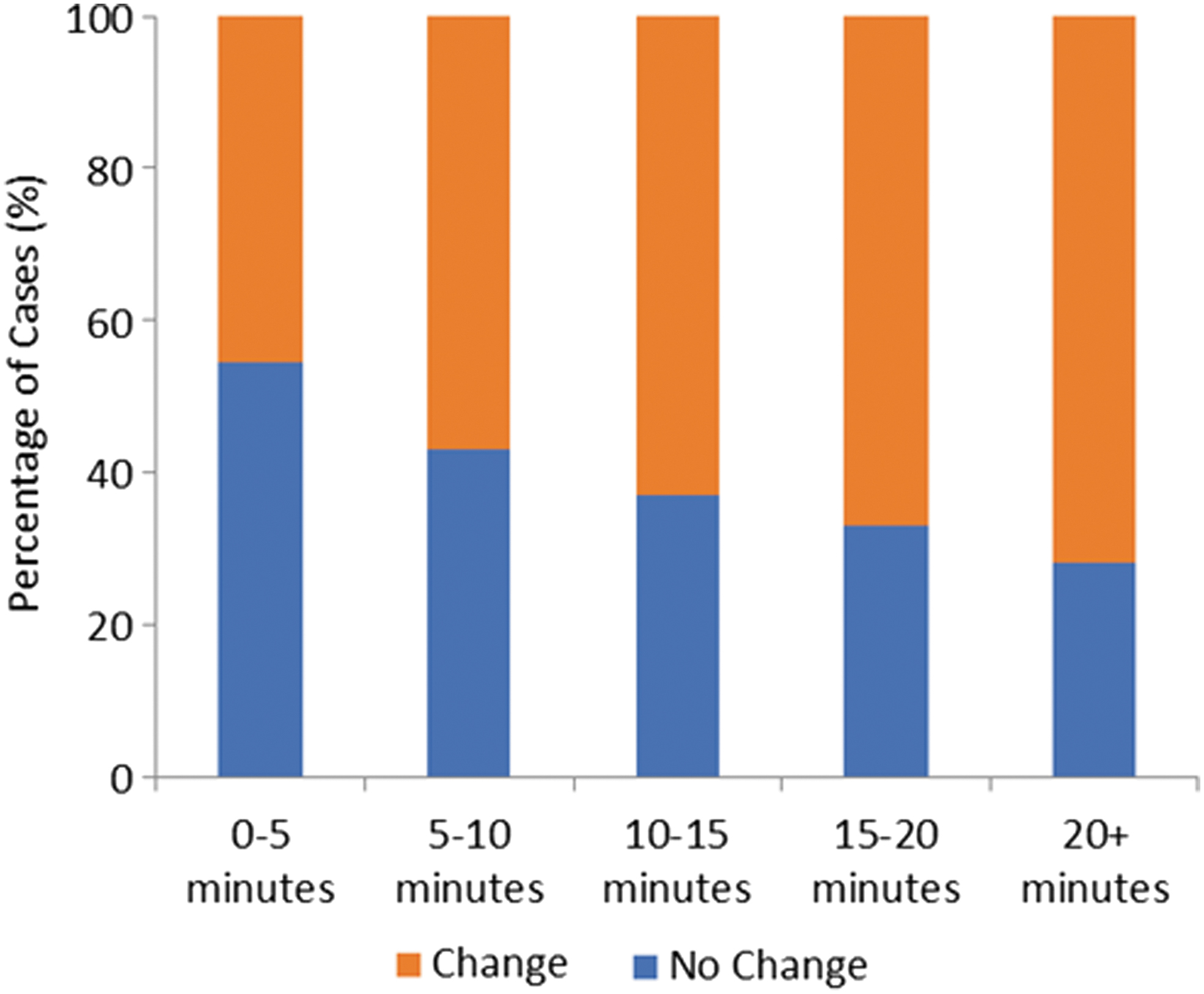
Association of specialists' self-reported billing time with primary care provider's change in action.
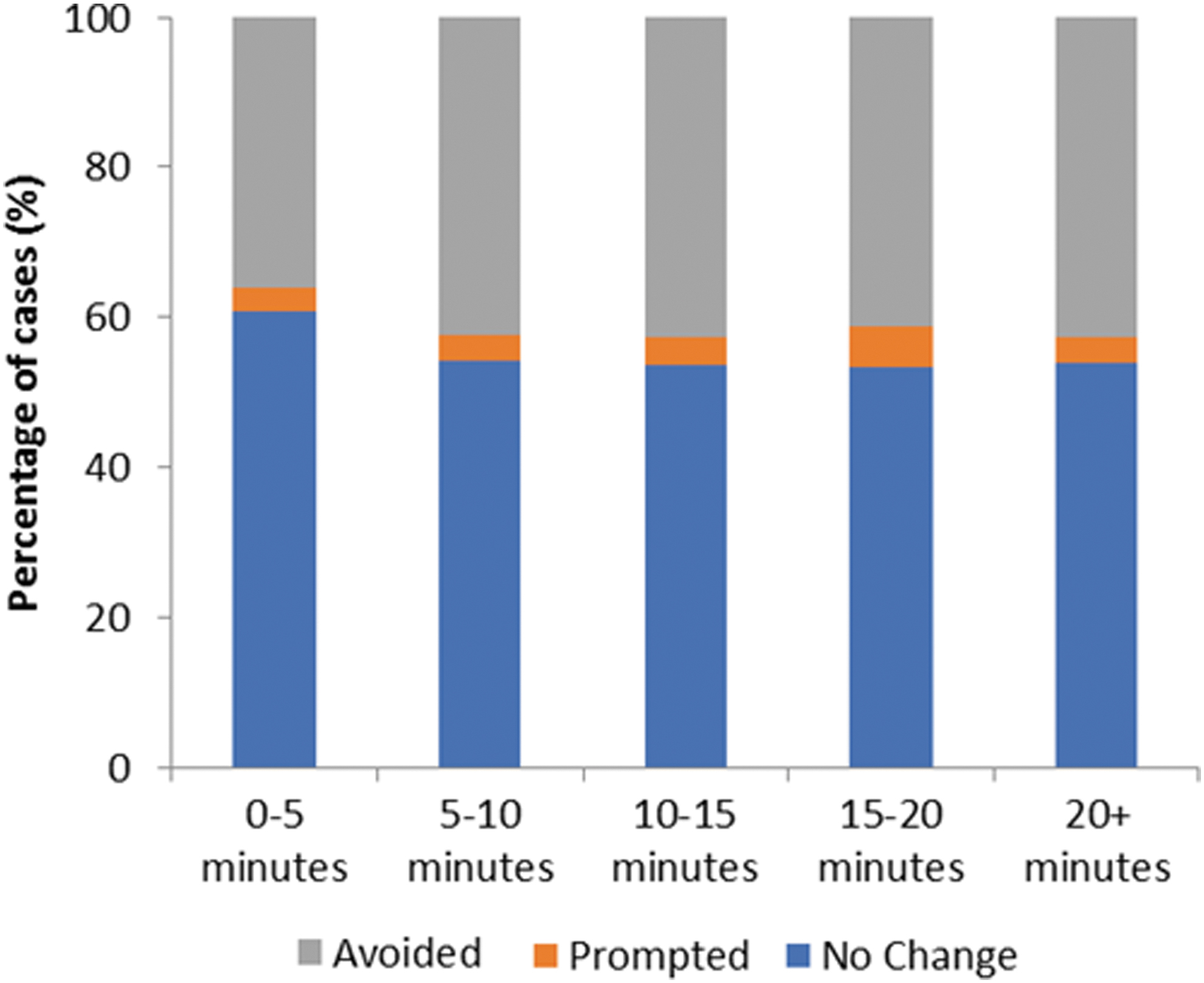
Association of specialists' self-reported billing time with primary care provider's decision to refer.

Association of specialists' self-reported billing time with primary care provider's perceived level of educational value/helpfulness of the case.
Discussion
A thorough understanding of when and how specialists respond to eConsult cases is critical to ensuring the service's long-term sustainability. Examining these factors and their impact on PCP behaviors helps us to better understand the service's overall value and serve to inform the structure of its remuneration process. Upon examining nearly 12,000 cases from 124 specialists across 36 specialty groups, we found that most responses were completed in less than 15 min and that the majority of specialists responded outside of typical office hours. While the flexibility offered by after-hours responses likely leads to quicker response times, there is some concern that such schedules may not be sustainable if case volumes expand, especially among specialties with high demand but a limited number of specialists (e.g., dermatology). We also found substantial differences in self-reported billing time between specialty groups, perhaps reflecting the complexity of the questions. Although long self-reported billing times result in higher costs up front, they also allow for more detailed answers, which offer the potential for greater savings through a larger impact on PCP course of action, fewer face-to-face referrals, and higher provider satisfaction.
While research on specialists' self-reported billing time for eConsult services is limited, our findings are nevertheless reflected in a previous study of response times. In one academic medical center in San Francisco, researchers asked specialists from 11 specialty groups to complete a survey in which, among other items, they provided the amount of time they spent in drafting their response to PCPs' questions. Payment was not dependent on this self-reported time. Despite this, the response times that specialists reported align closely with those of our study, with 55% of cases completed in less than 10 min (vs. 54% in our study), 36% in 10–20 min (vs. 39%), and 9% over 20 min (vs. 7.5%). 9
Self-reported billing time also varied significantly between specialty groups. A number of different factors may affect the amount of time specialists require to respond to a PCP's question, including its length, the complexity of the clinical question, whether it included attachments, and whether the specialist had to consult additional sources (e.g., the patient's electronic medical record [EMR], journal articles, and clinical guidelines). The effect of some of these factors has been reported in the literature. For instance, a study of an eConsult service implemented on a shared EMR found that in 41% of cases, the specialist reviewed information within the EMR that was over 1 year old. 12 Furthermore, some specialty groups were more likely than others to access historical medical data before answering the question. While our study was unable to identify in which cases specialists consulted additional sources or provided references or clinical guidelines, the potential for these factors to influence self-reported billing time is clear and further research is needed to examine their effect.
Most of the specialists who use our service are paid under a fee-for-service model, and the volume of eConsults they complete (a median of 64 per year) does not generally provide sufficient income to justify reducing their other clinical work. In a 2015 survey, 80% of responding specialists agreed that the eConsult process could be integrated into their clinical workload without difficulty. 13 Nevertheless, specialists answer the majority of eConsults outside of typical office hours, a practice that extends their working day and could potentially contribute to burnout. 14 In one small qualitative study involving four specialists from the VA health care system, specialists noted that eConsult does not save them time overall and, in fact, may create additional work. 8 As such, specialists who choose to join eConsult should not view the service as a means of reducing their overall workload, but rather as another means by which they provide patient care, one which must be balanced alongside their other duties in a manner that is not unduly taxing.
Finally, one of the key findings of this study was the relationship between self-reported billing time and changes in PCP behavior. Specifically, responses that took longer to complete were more likely to provide PCPs with new or additional information, resulted in fewer referrals, and were rated as more informative or educational. Given the potential cost savings associated with these outcomes, it is not clear that encouraging shorter self-reported billing times would ultimately be more cost effective, as shorter responses could lead to more referrals and a lower overall quality of care. Therefore, when it comes to self-reported billing time, it is important to note that shorter is not necessarily better and that specialists who take longer to respond appear to be using that extra time to deliver responses of commensurate value.
Our study had several limitations. While the length and complexity of PCPs' questions likely have some bearing on specialists' self-reported billing time, we were unable to quantify this in our analysis. Further complicating matters, providers who use our service are able to attach documents containing clinical questions or additional data relevant to the case. The length of these documents can range considerably in size. Our analysis could not account for the presence of attachments nor could it assess their length or content. There were too few individual specialists within each specialty group to evaluate differences between individual specialists. Finally, this study drew on data from cases submitted in a single health region in Ontario and, therefore, may not be generalizable to other locations. However, it is worth noting that the eConsult service has been replicated in five provinces across Canada, and the majority of metrics, such as response time, referral avoidance, and provider satisfaction, have been remarkably similar across jurisdictions.
Conclusion
Specialists' self-reported billing time varies by specialty group and is associated with changes in PCPs behavior and satisfaction. Further research is needed to identify what factors influence self-reported billing time and how eConsult can be best incorporated into clinicians' workflows.
Footnotes
Acknowledgments
The Champlain BASE eConsult service is a collaboration between the Champlain Local Health Integration Network, The Ottawa Hospital, the Bruyère Research Institute, and the Winchester District Memorial Hospital. Initial seed funding was provided by The Ottawa Hospital Academic Medical Organization's Alternate Funding Plan Innovation Fund and e-Health Ontario. Service sustainability funding is provided by the Champlain Local Health Integration Network and the Ontario Ministry of Health and Long-Term Care. Research funding for this project was provided by the University of Ottawa's Department of Medicine and the Canadian Institutes of Health Research. The authors affirm their independence from these funders. The funders played no part in the study design, collection, analysis, or interpretation of the data, in the writing of the report, or in the decision to submit the article for publication. The authors thank Ranjeeta Mallick for her work on the statistical analysis and Isabella Moroz and Justin Joschko for their assistance in preparing this article for publication.
Disclosure Statement
No competing interests declared by the authors.