
Abstract
Background:
Reducing door-to-balloon time may not reduce mortality, but reducing the time from symptom onset to first medical contact (FMC) may alone improve patient outcomes. The purpose of this study was to focus on analyzing sex differences in FMC call delay and its trend over the decades in patients with suspected acute coronary syndrome (ACS).
Methods:
Large private telemedicine data in patients with suspected ACS were used to investigate time delay in contacting a telemedicine call center. We identified 24,592 calls to a primary call center of patients with anginal symptoms and first electrocardiogram (ECG), using mobile 12-lead ECG devices. For the purpose of the current analysis, we included the first call of 14,420 patients for whom demographic, clinical ECG data were available.
Results:
First mobile ECG changes included suspected S-T Segment (ST) elevation in 2,220 (16%) cases, ST depression in 3,143 (22%) cases, or both in 685 (5%) patients. There were 6,721 (47%) calls to the center within less than 1 h of symptom onset. Chest pain, dyspnea, heart rate, male sex, absence of diabetes mellitus, early time period of the study, and ischemic ST segment changes on the first ECG were all independently associated with the increased likelihood of contacting the center within less than 1 h of symptom onset to FMC (p < 0.01 for all).
Conclusions:
Both chest pain and ischemic ECG changes were sex dependent for early medical contact, as such factors were significant among men (p = 0.001 and p = 0.024, respectively), but not among women (p = 0.024). The later time period of the study was associated with a shorter time delay among women more than that of men (p = 0.014). Women with prehospital chest pain or ischemic ST segment changes tend to seek medical help later than men. Temporal trends show attenuation of this sex disparity, with more women presenting earlier in the last decade.
Introduction
Women with acute coronary syndrome (ACS) have higher mortality rates than men. 1 While some data suggest that differences are influenced by older age, greater comorbidity, or different therapeutic modalities, 2 others suggested that sex differences appear to be driven by prehospital delays in women compared with men. This was defined as a longer time between symptom onset and accessing health care for those symptoms, resulting in treatment-seeking delays and consequently a worse prognosis. 2 –4
Although door-to-balloon times have improved significantly for S-T Segment (ST) segment elevation ACS, inhospital mortality has remained virtually unchanged. 5 These data suggest that other factors other than door-to-balloon time may improve mortality rate, such as shortening “first medical contact” (FMC), which is advocated by international guidelines. However, the concept of FMC is advocated by international guidelines, and little has changed in treatment-seeking delay times for women, a worldwide phenomenon that is independent of geographical, cultural, or racial relationship. 6 –9 Unfortunately, while no specific attempts were evaluated in women per se, attempts to intervene at the community level to decrease the prehospital delay in both sexes were unsuccessful. 8,10 The objectives of the current study were to examine whether women have longer symptoms-to-FMC time than men and to identify temporal trends in FMC delay among men and women with suspected ACS, using the largest prehospital telemedicine database in Israel.
Methods
The study was approved by the Institutional Review Board of the Baruch Padeh Medical Center. SHL Telemedicine Center (SHL Telemedicine Ltd., Tel-Aviv, Israel) is the largest private telemedicine program in Israel, operating for more than two decades, with centers for cardiac telemedicine worldwide (
All medical backgrounds of the patients are validated via a personal medical history interview and by hospital medical health record and discharge reports. The primary care summary information was included in a specific computerized individual SHL medical record for each patient. Once a patient calls the center, a history is taken and an initial home full 12-lead electrocardiogram (ECG) recorded by telemedicine and transmitted by the patients themselves simultaneously during their FMC call for an instant professional analysis by the call center team, which acts based on medical protocols that are updated periodically based on the guidelines of the European and Israeli heart societies.
Center staff underwent training according to current European Society of Cardiology (ESC) guidelines. Patients were instructed, using lay language, of what constitutes ACS symptoms and were trained on how to record and transmit ECG recordings by experienced SHL representatives. Patients were able to request as many training sessions as needed to reach adequate proficiency. For note, patients with severe crushing chest pain with dyspnea were instructed to call emergency medical services (EMS) and chew aspirin before recording and transmitting ECG.
The two devices that were used to record ECG data remotely are CardioSen'C™, the first mobile cellular-digital 12-lead ECG transmitter, and Smartheart™, the mobile full 12-lead ECG, enabling the detection of ischemic cardiac events. The devices transmit the data both digitally and acoustically over both cellular (iPhone, iPad, Android, etc.) and landline communication, within 30 s and without the assistance of a medical professional. The patients positioned the device on the chest area and performed the ECG by pushing a single button, and a full ECG reading was then transmitted to the monitoring center. The sequence of events included a patients' FMC to the SHL call center, staffed by an experienced medical team, including physicians and nurses who were specifically trained in telemedicine. ECGs were transmitted within seconds to the SHL call center. Data were integrated, baseline and current and baseline ECG, medical history, and current clinical presentation. A health care provider contacted the patients for further instructions. When deemed necessary, EMS, staffed with a physician and paramedics, were sent with to the patients within a few minutes.
Study Population
Over a period of more than two decades, between the years 1996 and 2017, we identified 24,592 calls from subjects with cardiac symptoms with suspected ACS, defined as one or more of the following: previous cardiac events, family history of ACS and risk factors, current symptoms, and first initial home recordings of a full 12-lead recorded ECG. The ECG recordings were transmitted simultaneously during the FMC call by the patient via telemedicine to our call center and noted to have ischemic changes by the professional team on the line. For the purpose of the current analysis, we included the first call of 14,562 subjects for whom demographic, clinical ECG data were available. Inclusion criteria were SHL patients with risk factors for ACS, who exhibited subjective symptoms of ACS (such as dyspnea, pain, and/or discomfort of the chest). In addition, we included only patients with adequate cognitive capacity to comprehend instruction, and were able to independently record and transmit ECG recording. In cases where the quality of the 12-lead recordings was low, an SHL call center representative contacted the patients to repeat ECG recordings and provided additional instructions as required.
Definitions and Study Endpoint
The primary outcome of the current study was time delay of less than 1 h from symptom onset to FMC of early time versus very late time (i.e., >6 h), as previously defined. 11 ST segment elevation or depression was documented by nurses with acute cardiac care training and based on ESC guidelines at the time of documentation. For the purpose of the current analysis, ischemic ST changes include the combination of ST elevations and ST depressions, each in at least two consecutive leads. Subjects were considered to have diabetes mellitus, hypertension, or dyslipidemia if their primary care physicians treated them for these disorders or based on self-report. For the purpose of identifying temporal trends, calls were dichotomized to two time period groups according to the median (March 2005).
Statistical Analyses
Continuous variables were expressed as mean ± standard deviation if normally distributed or median with interquartile range if skewed. Categorical variables were presented as frequency (%). Continuous data were compared with the Student's t-test and categorical data were compared with the use of the chi-square test or Fisher exact test. Univariate and multivariate binary logistic regression analysis was performed to identify parameters that were associated with a time delay of more than 1 h. Parameters that were found to be significant in the univariate model were then incorporated into the multivariate model. The consistency of the association of any parameter with FMC time delay was further assessed with the use of statistical tests of interaction between sex and multiple important parameters within the logistic model. The p-value of <0.05 was considered statistically significance. The statistical analyses were performed with IBS SPSS version 20.0 (Chicago, IL).
Results
The final study population included 14,420 patients, of whom 59% were men (Table 1). The mean age of the study population was 71 ± 13 years. More than 80% of the patients who called the SHL call center were able to perform ECG with adequate quality. The most common presenting symptom was chest pain (74%), followed by dyspnea (30%). Irregular heart rate, as confirmed by the ECG, was present in 8% of the patients. Medical history was significant for current smoking, hypertension, and diabetes mellitus among 23%, 57%, and 27% of the population, respectively. Fifty percent of the population had a history of myocardial infarction. Presenting ECG included suspected ST elevations in 16% of the patients, ST depressions in 17% of the patients, and inverted T waves in 55% of the patients. Ischemic ST changes, defined as a combination of ST elevation and depression, were present in 5% of patients. Nine percent of the patients were not referred for further evaluation. Table 1 includes a comparison of baseline characteristics of men versus women, demonstrating significant differences between the two groups with respect to demographics, clinical and medical history, and presenting ECG. There were 2,723 (19%), 2,171 (15%), and 1,827 (13%) calls to the center within 15, 30 min, and 1 h of symptom onset, respectively. In addition, there were 1,208 (8%), 4,008 (28%), and 2,483 (17%) patients who contacted the center after more than 1, 2, and 6 h of symptom onset, respectively. When dichotomized to two mutually exclusive groups, there were 6,721 (47%) and 7,699 (53%) patients who contacted the center within less or more than 1 h, respectively.
Characteristics of Study Population
After March 2005
SBP, systolic blood pressure; ST, s-t segment; DBP, diastolic blood pressure; MI, myocardial infarction; CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention; ECG; electrocardiogram; FMC, first medical contact; ACS, acute coronary syndrome.
Predictors of Time Delay <1 h
Predictors of time delay of less than 1 h between symptom onset and FMC are summarized in Table 2. Men were significantly more likely to present within less than 1 h compared with women. In addition to male sex, chest pain, dyspnea, irregular heart rate, low blood pressure, heart rate, and personal history of myocardial infarction were all associated with time delay of less than 1 h in the study cohort. Univariate odds ratio (OR) for all important predictors of shorter time delay is presented separately for men and for women in Table 2. Notably, while ischemic ST changes were associated with a significant 64% increased likelihood of shorter time delay in the overall cohort, this association was significant for men but not for women in the univariate model (OR 1.89 and p < 0.001 for men vs. OR 1.21 and p = 0.16 for women). Multivariate predictors of time delay of less than 1 h are summarized in Table 3 for the entire cohort as well as separately for men and women. Male sex, chest pain, dyspnea, diabetes, heart rate, ischemic ST segment changes, and later time period of the study were all associated with shorter time delay (p < 0.01 for all).
Predictors of First Medical Contact <1 h—Univariate Model
After March 2005.
OR, odds ratio.
Predictors of First Medical Contact <1 h—Multivariate Model
The model is further adjusted to age, personal history of myocardial infarction, irregular heart rate, and systolic blood pressure (p > 0.01 for all).
p for interaction for sex 0.02.
Sex Disparities in Predictors of Time Delay
Interaction analysis demonstrated that the association between three of the parameters in the multivariate model was sex specific (Table 3). First, chest pain was associated with shorter time delay among men but not among women (1.36 for men vs. 0.94 for women, p for interaction <0.001). Consistently, ischemic ST segment changes were also associated with shorter time delay among men but not among women (1.93 for men vs. 1.36 among women, p for interaction = 0.024). Second, while the later time period was associated with shorter time delay among both sexes, the association was more pronounced among women (1.23 for men vs. 1.48 for women, p for interaction = 0.014).
Subgroup Analysis of Patients Sent to Hospital
There were 7,052 (57%) patients who were evaluated by a prehospital team, and among them 6,699 (95%) were sent to hospital for further evaluation and treatment. Results of the multivariate subgroup analysis of this group are summarized in Table 4 and are consistent with the analysis of the entire study cohort. The subanalysis shows that male sex, ischemic ECG changes, and later time period of the study were all independently associated with shorter time delay to FMC (p < 0.001 for all).
Predictors of First Medical Contact <1 h—Multivariate Subanalysis of Subjects Sent to Hospital
The model is further adjusted to age, personal history of myocardial infarction, irregular heart rate, and systolic blood pressure (p > 0.05 for all).
Discussion
The main findings of our current study were that women, when compared with men, were not only less likely to have an early FMC (<1 h) but are also late in doing so (>6 h). Moreover, the presence of chest pain and ischemic ST changes in the very initial ECG recording, which were clear triggers for an early call in men, did not promote such an early call in women (Fig. 1). A trend analysis demonstrated that over the last two decades, FMC time delay has significantly shortened in both men and women; however, women still have a longer FMC time delay compared with men (Fig. 2). In addition, less than 50% of the men have time delay to FMC of less than 1 h, suggesting that there is an opportunity for improvement.
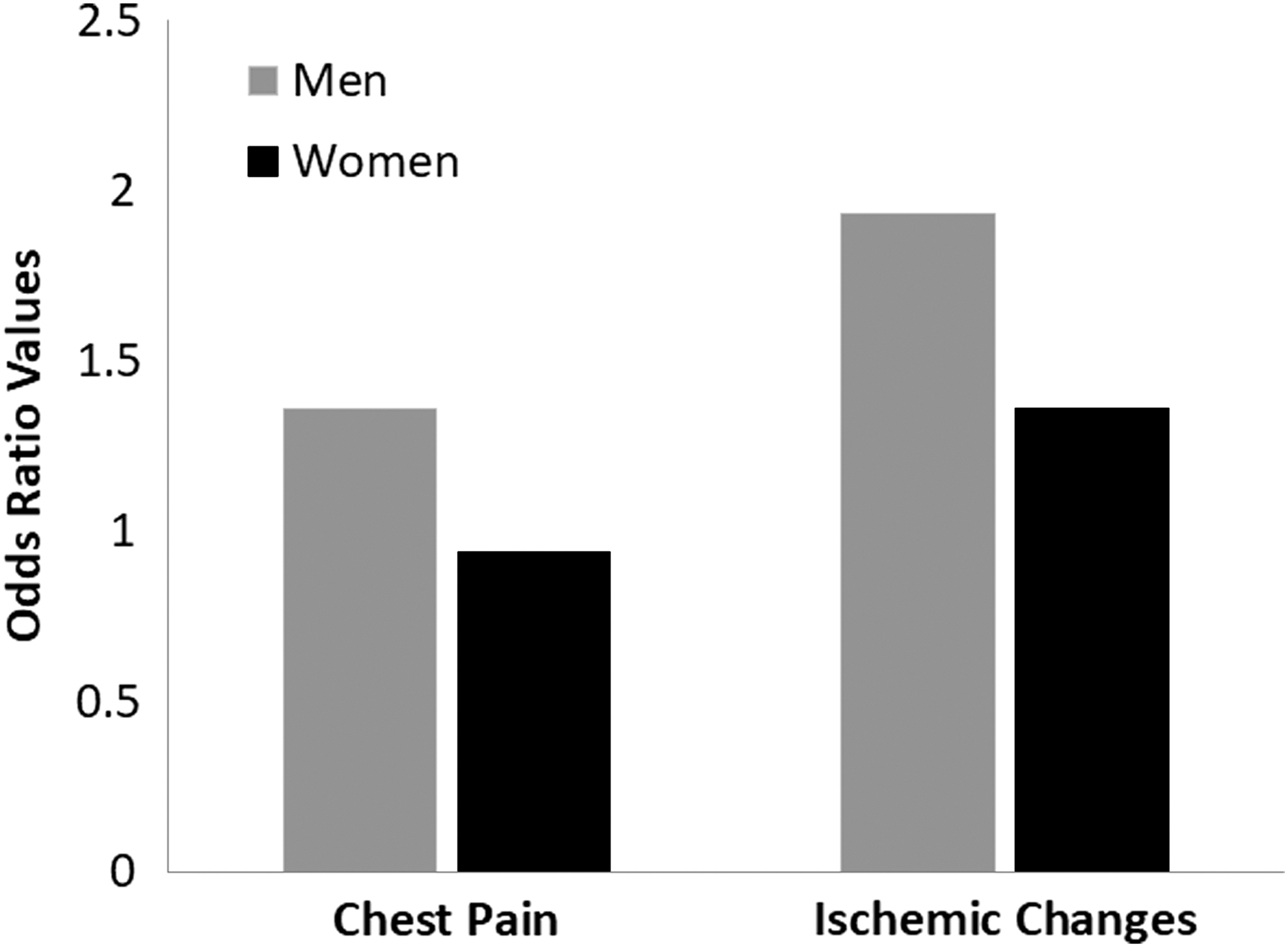
Sex disparities in multivariate ORs. The y axis represent the OR for chest pain, and ischemic electrocardiogram change for male patients (blue bars) and female patients (red bars). OR, odds ratio.
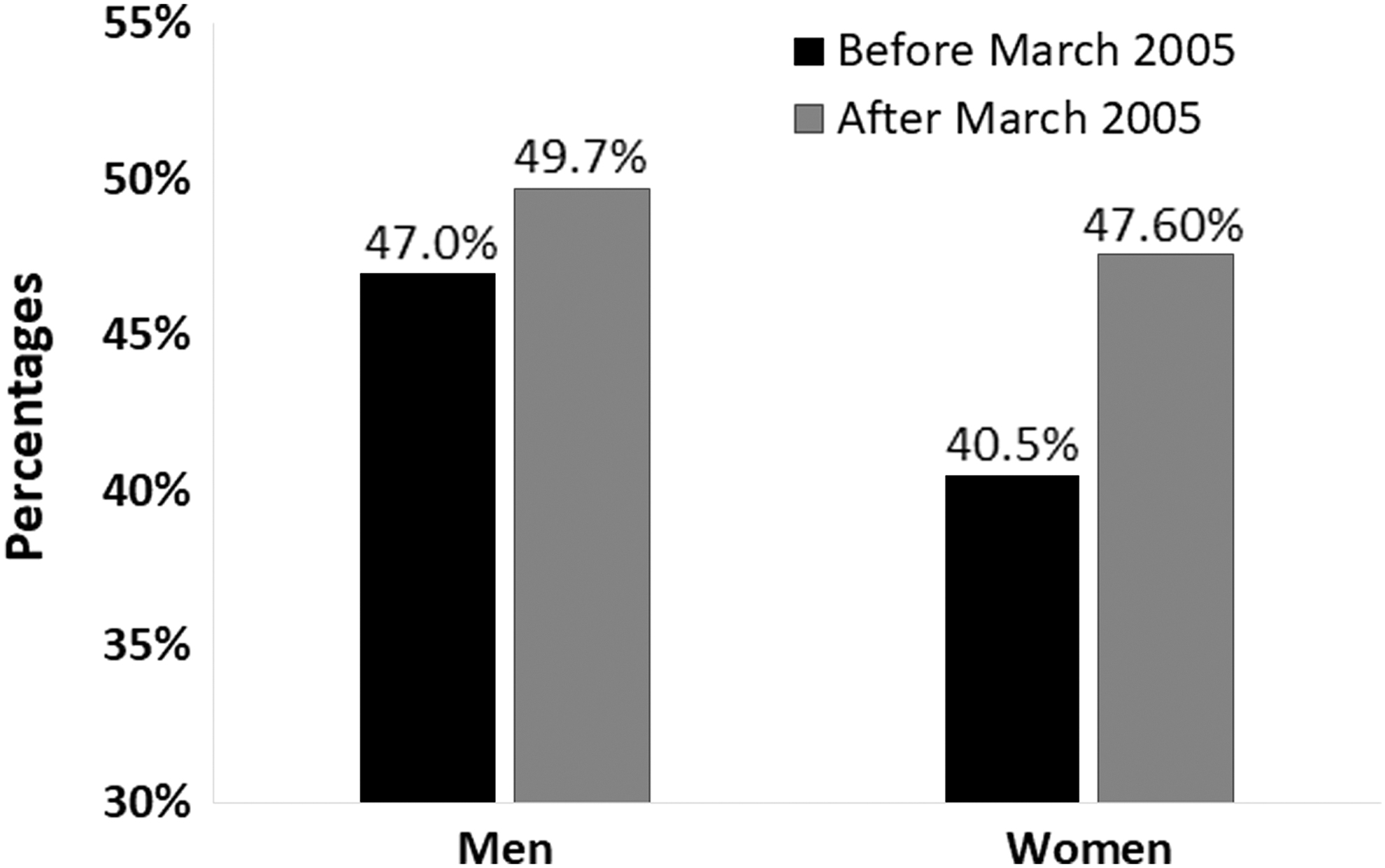
Time delay of <1 h in men and women. Time delay of <1 h in men and women in percentages, before March 2005 (red bars) and after March 2005 (blue bars).
Our study used a large telemedicine cohort to investigate time delay in contacting a telemedicine call center, using an analysis of a very initial home recording full 12-lead ECG and telemedicine transmitted by the patients themselves simultaneously with their FMC call for an instant professional analysis. This combination of clinical presentation associated with the earliest ECG recording, which practically can be done, is unique and to the best of our knowledge is the first to be reported. Indeed, the Immediate Myocardial Metabolic Enhancement during Initial Assessment and Treatment in Emergency Care trial with a similar cohort of ACS patients, as defined by symptoms and ECG changes, reported that older people and women have longer total times for EMS call. In contrast to our study, this study was performed over a 5-year duration and the prehospital 12-lead ECG was done only on the arrival of the EMS team to the patients' homes, rather than the instantaneous online 12-lead ECG, which was transmitted in our study as part of our call center FMC protocol. 3
Despite an already acknowledged difficulty in establishing prehospital delay times due to inconsistent measurements, 12 women have been notoriously noted to have a significantly longer prehospital delay compared with men. 1,9,11,13 –15 While sex differences exist in the pathophysiology of ACS, several studies have attempted to elucidate what causes women to delay seeking medical help for ACS compared with men. Specific women-related prodromal clinical signs, 9 misinterpretation of symptoms by women, 16 and psychosocial elements 17 were all suggested as potential explanations.
The fact that women are less likely to experience typical chest pain has also been noted in scientific statements, registries, and cohort studies. 9,18 –20 In a Swedish survey of women with STEMI, longer prehospital delay was primarily attributed to atypical symptoms in women compared with men. 13 Interestingly, and in contrast to the notion that emphasizes this atypical presentation in women as the major cause for prehospital delay in ACS, in our study, in the female cohort, the presentation of chest pain, when it did occur, was not recognized as a trigger for an early FMC as clearly and significantly as it was for our male cohort. 11,15 Diabetes mellitus 11,21 and previous MI 21 –27 were associated with shortened prehospital delay times.
In contrast to these studies, yet similar to others, the current analysis demonstrated that older age and history of MI were not associated with early FMC, while chest pain, dyspnea, and elevated heart rate were all associated with an early FMC. 22,23,28 Similar to chest pain and dyspnea, diabetes mellitus was also associated with shorter time duration to FMC. However, in contrast to these two clinical symptoms, interaction analysis showed that the association was sex dependent and noted to be significant among men.
Of note, the significant triggers reported in the primary analysis remained significant in the subanalysis of patients who were eventually referred to the hospital by the EMS team. The decision to send them to the hospital was made only after arriving to the patient's home following the initial FMC call. Furthermore, while a team was sent to aid women more often than men, fewer women were sent to the hospital.
Yet, another unpredicted and intriguing finding of our study was that ischemic changes on the ECG (i.e., an ischemic combination of ST elevation and depression) were the most significant trigger associated with an early FMC call. Several critical observations should be emphasized. This is the most initial 12-lead ECG a patient may have, since it was easily recorded in moments by the patients themselves at home and transmitted over the phone as part of our telemedicine call answering center protocol. The significance of these findings is underscored by the fact that these very initial ECG ischemic changes were blinded to the lay calling patients, yet were superior to any other clinical parameters, including relevant comorbidities in triggering an early FMC. Of note, while this was the case in the general population and especially in the men cohort, interaction analysis failed to observe this phenomenon among women. A potential explanation for these significant sex differences may be related to the different mechanisms of angina known to occur in women. 29
While other studies, which evaluated trends of prehospital delay in ACS over long-term follow-up, found no significant change over that period in both sexes, 11,14 we did find some encouraging trends when comparing the last decade with the previous one in our two decades of analysis. While both men and women had significantly shorter FMC call delay, women had a more significant improvement in shortening their FMC call time compared with the men. However, in the last two decades, despite greater improvement in time delay among women, women still have a longer FMC time delay compared with men.
Study Limitations
This is a retrospective observational study of a selected study population. The findings may not be applicable to other patient populations. 13 As we focused on the prehospital FMC delay, the inhospital course, which may have a complementary important aspects, was not analyzed here. However, the critical role of time delay in improving patient outcome is based on robust clinical data and endorsed by all guidelines.
Conclusion and Clinical Implications
The finding of the study is that over the last two decades, time delay for FMC was shortened significantly as evidenced by data from innovative telemedicine technology. While over the last decade, women were noted to shorten the delay from chest pain onset to FMC, women are still lagging behind men in their FMC time, even when they present with anginal chest pain accompanied by simultaneous ischemic ECG changes. Therefore, novel approaches should be developed to bridge this gap to reduce cardiovascular morbidity and mortality in women.
Footnotes
Disclosure Statement
Professor O.A. is a consultant to SHL Telemedicine Ltd. Dr. A.L. is a member of the Board of Directors of SHL and Dr. Y.A. is an SHL Telemedicine employee.