
Abstract
Aims:
This study aimed to determine the impact of tele-intensive care unit (ICU) on ICU mortality rate (%), and to quantify association of the tele-ICU intervention with ICU length of stay (LOS, days), readmission rates (%), reintubation rates (%), hospital-acquired pressure ulcer (HAPU) rate (%), and discharge against medical advice (DAMA) rate (%) in five hospitals.
Methods:
A multicenter case-historical control study was conducted on short-term outcomes of tele-ICU program in five private hospitals within Arabian Gulf Region. Critically ill adult patients admitted into ICU without tele-ICU were recorded as control group (pre-tele-ICU), whereas those admitted to tele-ICU were grouped as treatment group (post-tele-ICU). The observed outcomes for each patient were then recorded, namely mortality, reintubation, readmission, HAPU, DAMA, and length of stay (LOS).
Results:
Chi-square test showed that there are significant differences in mortality rate (χ2 = 6.596, p = 0.010), readmission rate (χ2 = 4.315, p = 0.038), HAPU rate (χ2 = 10.445, p = 0.001), and DAMA rate (χ2 = 4.485, p = 0.034) between pre-tele-ICU and post-tele-ICU, at 0.05 significance difference level. Independent t-test showed that there is significant different in LOS (t = 43.63, p < 0.001) between pre-tele-ICU (mean = 6.72 days) and post-tele-ICU (mean = 5.79 days). Odds ratio showed that critically ill adult patients who admitted to post-tele-ICU have 19% less reduction in mortality rate, 23% less reduction in readmission rate, 43% less reduction in HAPU rate, and 11% less reduction in DAMA rate as compared with those admitted to pre-tele-ICU.
Conclusion:
Tele-ICU as a step to improve the quality of health care project has shown statistically significant improvement in the adult ICU patients' outcomes, which lead to lesser mortality rate, readmission rate, HAPU rate, DAMA rate, and shorter LOS.
Background
Tele-intensive care unit (ICU), which is also known as virtual ICU, e-ICU, and remote ICU, is a remote monitoring technology that enhances the effective distribution of intensivists and other critical care resources. 1,2 It can enable critical ill patients to stay in remote setting using audio, video, and electronic links rather than travel to specialist centers. 3 Furthermore, tele-ICU can provide ICUs with 24/7 access to expert critical care physicians and nurses. Care provided by tele-ICU includes ability to notice patient's instability, ordering diagnostic testing, communicating with bedside providers and patients, and making diagnoses. 4 Tele-ICU monitoring system has spread quickly over the past 10 years, with ∼1 million patients being monitored. 2
The complexity of ICU services necessitates the need for sharing health data through off-site ICU centers. What is unknown is there specific elements of tele-ICU that possibly can affect quality of patient care. Better understanding on how tele-ICU effects care processes and patient outcomes is needed. This study concentrates on some significant quality indicators of patient care pre- and post-tele-ICU implementation.
A PubMed and Google Scholar search have revealed that there was a variation in benefits reported whether tele-ICU can improve patient care or not. The majority of studies have studied two specific patient short-term outcomes that are mortality and length of stay (LOS) pre- and post-tele-ICU implementation. 5 As a result, improvement in both of these outcomes as evidence by reduction in their rates implies potential cost savings.
Furthermore, other studies found significant positive change in readmission rates and financial outcomes with tele-ICU use. 6 –9 Tele-ICUs can improve intensive care quality and reduce the costs. Those profits can offer a beneficial chance for patients, hospitals, and payers. 10 Only a few studies evaluated the financial returns from implementation of tele-ICUs and are difficult to generalize to guide hospitals when considering implementation of the tele-ICU. However, there were some studies that oppose the positive short-term outcomes of tele-ICU and did not significantly improve patient outcomes. 11,12
Health care services in Saudi Arabia have progressed greatly over current years in all levels of health care services that require more advanced critical care capabilities. 13 Indeed, the effectiveness and the impact of tele-ICU on patient outcomes in Saudi Arabia remains unclear. Only one study has been conducted in Saudi Arabia about tele-ICU that showed no association between tele-ICU implementation and patient outcomes in terms of mortality or LOS rates. 11 However, the study was conducted in a single center that would affect the generalizability of the results. In addition, the study did not utilize Acute Physiology Score (APS) and Acute Physiology and Chronic Health Evaluation (APACHE) scores to measure the severity of disease in ICU.
This study was conducted at Dr. Sulaiman Al Habib Medical Group (HMG) that is considered the largest private tertiary medical center in the Middle East. HMG has the first tele-ICU command center in the Middle East that monitors several national and international branches. This study was conducted in multicenters inside and outside Saudi Arabia. All patients admitted to the ICUs in Dr. Sulaiman Al Habib Medical Group were being measured with APACHE score. The primary outcomes of this study were to determine the impact of tele-ICU on ICU mortality. The secondary outcomes were to quantify association of the tele-ICU intervention with ICU LOS rates, readmission rates, and reintubation rates.
Methods
Design and Setting
This study design is a 2-year multicenter case-historical control study. Data for control group (pre-tele-ICU) were collected during the period of November 2015–October 2016, whereas data for treatment group (post-tele-ICU) were collected during the tele-ICU implementation period during November 2016–October 2017. The study was conducted at HMG Tele-ICU command center in Riyadh, Saudi Arabia. It included adult ICUs in five different hospitals that belonged to the medical group projects. A total of 125 beds of critically ill patients were investigated in this study. The tele-ICU is an off-site command center that is covered 24/7 by nurses and physicians where intensivist conduct daily virtual clinical rounds. In addition, intensivist in the tele-ICU could cover units that did not have intensivist. Furthermore, junior doctors could contact the intensivist in the command center for any concern regarding their patients. In other words, the resources for intensivist were centralized for more efficient resources allocation.
Data Collection
Tele-ICU command center monitor has been in compliance through a weekly audit report. Data were collected using auditing chart of the tele-ICU command center. A total of 20,280 adult patients were admitted to the ICU between November 2015 and October 2017. In addition, 9,779 samples were collected for pre-tele-ICU intervention group from November 2015 to October 2016, whereas 10,501 samples were collected for post-tele-ICU intervention group from November 2016 to October 2017. The observed outcomes for each patient's ICU mortality, LOS, readmission, reintubation, hospital-acquired pressure ulcer (HAPU) rate, and discharge against medical advice (DAMA) rate were recorded for analysis purpose.
Ethical Considerations
The study proposal was submitted for approval to the institutional review board (IRB) committee at Al Habib Research Center. An approval to exempt a review of the study was obtained to conduct the study (IRB No: RC1804/01). Researchers of this study highly considered the privacy and confidentiality issues of the study during data collection procedure and ensured that participants will not be identified.
Data Analysis
Data collected were analyzed through the mean of descriptive and inferential statistics using IBM-SPSS® Version 22 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.). Data were first entered into an Excel spreadsheet and then imported to SPSS for analysis. To assess the differences in mortality rate, reincubation rate, readmission rate, HAPU rate, and DAMA rate between pre-tele-ICU and post-tele-ICU groups, the study utilized χ 2 -square test. All significant results were further analyzed by computing the Mantel-Haenszel odds ratio. Furthermore, the study also employed independent t-test to evaluate the significant difference in mean of stay (days) between pre-tele-ICU and post-tele-ICU. It is important to note that significance level of 0.05 was used in this study.
Results
A total of 20,280 samples were collected from five hospitals, in which 9,779 patients were from pre-tele-ICU intervention and 10,501 patients were from post-tele-ICU intervention (Table 1). For mortality rate, results revealed that there is significant difference in mortality rate (χ 2 = 6.596, p = 0.010) between type of ICU at 0.05 significance level (Fig. 1). Mortality rates have significantly dropped from 3.4% (pre-tele-ICU) to 2.8% (post-tele-ICU). Odds ratio of 81% indicates that having tele-ICU reduced the mortality rate of patients by 19%. It was also found that post-tele-ICU had significantly lower readmission rate (1.1%) than pre-tele-ICU (1.5%) at 0.05 significance level (χ 2 = 4.315, p = 0.038) (Fig. 2). In addition, odds ratio of 77% showed that adult patients admitted in post-tele-ICU are 23% less likely to encounter readmission as compared with those admitted in pre-tele-ICU. Next, results showed that there is significant difference in HAPU rate (χ 2 = 10.445, p = 0.001) at 0.05 significance level (Fig. 3). The HAPU rate was 0.9% in conventional ICU, which significantly dropped to 0.5% with implementation of tele-ICU. Moreover, odds ratio of 57% implied that adult patients admitted to pre-tele-ICU have 75% higher chances to get HAPU than those admitted to post-tele-ICU. For DAMA, results showed that there is significant difference in DAMA rate (χ 2 = 4.485, p = 0.034) between pre- and post-tele-ICU intervention, at 0.05 significance level. Odds ratio of 89% showed that adult patients admitted to pre-tele-ICU have 12% higher chances to get DAMA than those admitted to post-tele-ICU (Fig. 4). As far as LOS is concerned, this study discovered that there is significant difference in LOS (t = 43.63, p < 0.001), at 0.05 significance difference level (Fig. 5). Results showed that adult patients admitted to pre-tele-ICU had higher mean LOS of 6.72 days than those admitted to post-tele-ICU with lower mean LOS of 5.79 days. Data analysis also showed that there was no statistically significant difference in reintubation rate during post-implementation of tele-ICU period, p value >0.05 (Fig. 6).

Mortality rate. ICU, intensive care unit.

Readmission rate. ICU, intensive care unit.

HAPU rate. HAPU, hospital-acquired pressure ulcer; ICU, intensive care unit.
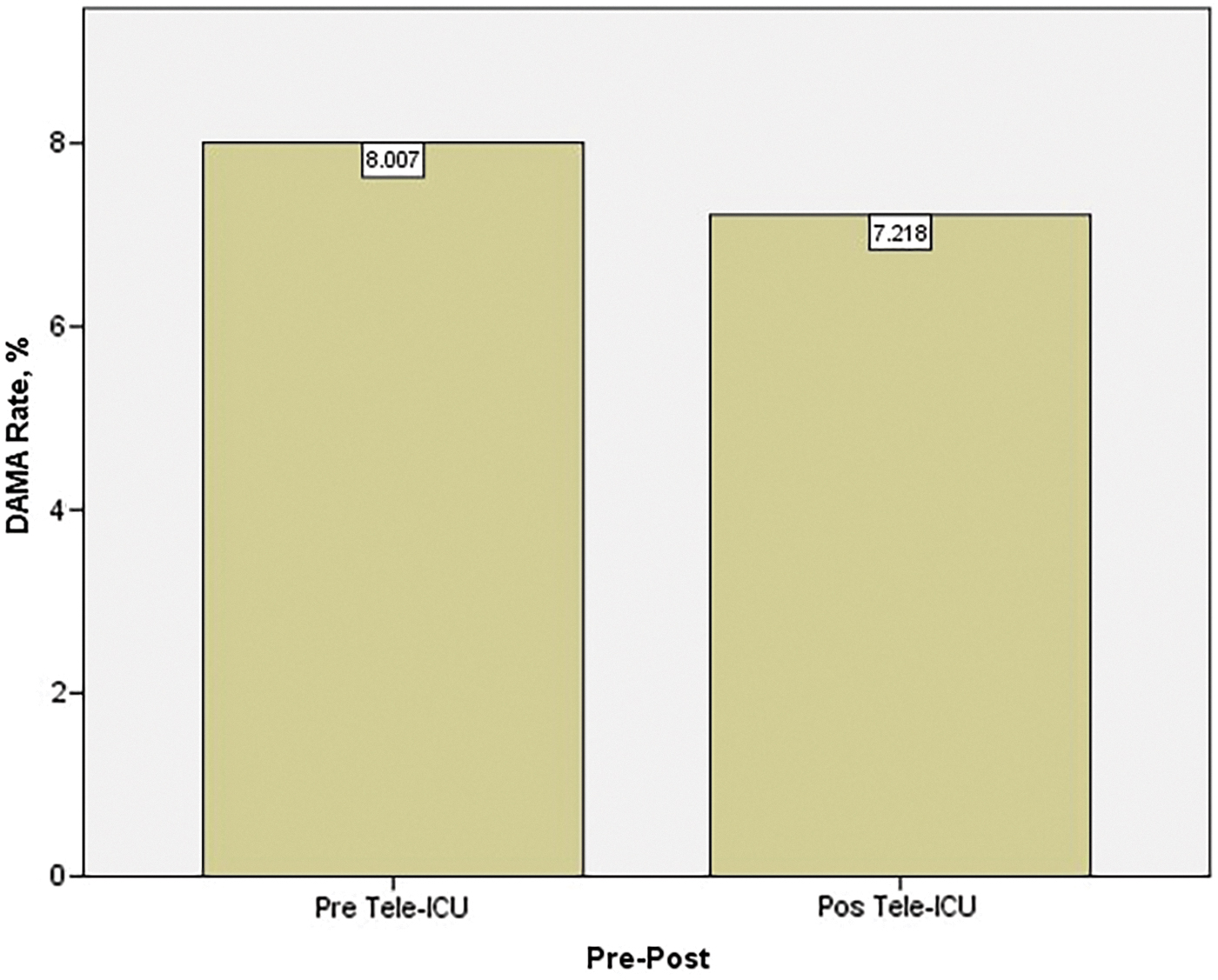
DAMA rate. DAMA, discharge against medical advice; ICU, intensive care unit.

CI LOS. CI, confidence interval; ICU, intensive care unit; LOS, length of stay.

Reintubation rate. ICU, intensive care unit.
Patient Outcomes Sample
ICU, intensive care unit; LOS, length of stay.
Discussion
The tele-ICU command center of HMG is a multicenter and has a very consistent measurement, as well as reporting. This study aimed to evaluate the impact of tele-ICU on ICU mortality rate, LOS, readmission rate, reintubation rate, HAPU rate, and DAMA rate. Assessing and comparing pre- and post-tele-ICU outcomes can illustrate its effect on patients' progress and condition. The results of this study showed that the tele-ICU program intervention significantly improved or reduced mortality rate (%), LOS (days), readmission rate (%), HAPU rate (%), and DAMA rate (%).
The study, however, found that there is no significant difference in reintubation rate of adult patients between pre- and post-tele-ICU. This means that tele-ICU adoption does not have significant impact on reincubation rate of adult patients. The findings of this study were congruent with many previous studies that proved tele-ICU significantly (statistic) reduced ICU mortality rate and LOS. 8,14 –20 The reduction in mortality rate and LOS was probably due to better resource allocation and constant real-time monitoring of patient conditions by the tele-ICU command center, which, in return, contributes to better patient safety and reduced patients' stay in ICU. Taking the article of Lilly et al., 16 for example, the researchers conducted the study in 56 ICUs in 32 hospitals and concluded that tele-ICU decreased ICU mortality rate and LOS. ICU mortality rate and LOS were statistically significantly shorter for tele-ICU intervention group patients.
Looking at readmission outcomes of adult patients, the study found that there is significant decrease in readmission rate of patients after implementation of tele-ICU. This finding is parallel with a recent study done by Fortis et al., 6 which showed that readmission rates were remarkably lower after implementing tele-ICU (p = 0.0064). This study provides extra insights into HAPU and DAMA rates that were not assessed by previous researches. The findings showed that tele-ICU managed to decrease the rate of HAPU and DAMA rates.
The tele-ICU program actually brings more benefits beyond just the cost savings of hospitals. 21 Researchers emphasized that tele-ICU will actually benefit hospitals in a manner that could promote better patient outcomes. In this study, researchers hope that the evidence collected pertaining to benefit or effectiveness of tele-ICU will provide solid insights for the tele-ICU program to be fully integrated into the hospital system in Saudi Arabia. Tele-ICU could be recognized as a technological and strategic advantage since it is cost-effective and helps in reducing the cost through a decrease in mortality rate and LOS. 22 Furthermore, tele-ICU offers a crucial opportunity to recognize conditions of adult critical care that affect patients' outcomes, 5 in this case mortality, LOS, readmission, HAPU, and DAMA rates.
A number of limitations should be taken into considerations while interpreting this retrospective study. The fact is that this study represents associations rather than cause and effect relationship. The study findings may not be generalized to other hospitals as the study design was only observational rather than randomized control trial. This study represents a large sample size of 20,280 adult patients. The findings of this study were similar to findings of previous studies, which further validate the current study findings, in the context of Saudi Arabia.
Conclusion
Tele-ICU is an approach for improving the quality of critical care services. This multicenter case-historical control study on short-term outcomes of tele-ICU study showed substantial statistically significant differences in patient's outcomes including ICU mortality rate, LOS, readmission rate, and reintubation rate. The study revealed a positive impact of adult tele-ICU in those outcomes.
Footnotes
Acknowledgments
The authors thank the clinicians at Dr. Sulaiman Al Habib Medical Group Tele-ICU command Center for their time and contribution to this study.
Authors' Contributions
A.O. was involved in conception, proposal, ethical approval, recruitment, and data collection. A.A. carried out conception, proposal, ethical approval, data analysis, and article preparation. M.A. was involved in proposal, ethical approval, and article preparation. F.J. carried out article preparation.
Disclosure Statement
No competing financial interests exist.