
Abstract
Background:
Stroke expertise is critical for timely and appropriate intravenous thrombolysis (IVT) and affects IVT use.
Introduction:
In Slovenia, IVT is administered in general hospitals, which often lack on-site neurologic expertise. To overcome this obstacle, a national telestroke network, TeleKap, has been implemented. The aim of the study was to determine whether TeleKap is associated with enhanced IVT use.
Materials and Methods:
This investigation was a retrospective observational study comparing the number of acute ischemic stroke (AIS) patients and the use of IVT during the first 3 consecutive years. TeleKap, a decentralized hub-and-spoke telestroke model covering the entire nation, consists of one comprehensive stroke center and 12 spokes classified according to the availability of on-site neurologic expertise.
Results:
During the observation period, we treated a total of 1,316 patients with AIS, of which 508 (38.6%) received IVT. We found statistically significant positive trends in the number of IVT patients (142 in 2015, 158 in 2016, and 208 in 2017; B = 4.39, standard error (SE) = 1.59, p = 0.01) and the number of AIS patients (326 in 2015, 424 in 2016, and 566 in 2017; B = 14.42, SE = 5.19, p = 0.01) for all spokes. The trend in the IVT rate was numerically negative but did not reach statistical significance (43.5% in 2015, 37.3% in 2016, and 36.7% in 2017; p = 0.30).
Discussion:
TeleKap enhanced IVT use regardless of on-site neurologic expertise.
Conclusions:
TeleKap proved to be efficient. It could serve as a model of telestroke care for other similar countries.
Introduction
It is well known that intravenous thrombolysis (IVT) for acute ischemic stroke (AIS), when applied early after symptom initiation, improves patient outcomes in a time-dependent manner. 1 Additionally, telestroke, an application of telemedicine, allows a rapid and reliable recognition and treatment of AIS without on-site neurologic expertise. Eligible patients receive IVT in the emergency department and are admitted either to the stroke unit (SU) of the admitting hospital (drip and keep) or to a comprehensive stroke center (CSC) (drip and ship) to complete the infusion. 2 In most Slovenian general hospitals (GHs), neurologic expertise is limited to regular working hours; in others, it is entirely lacking.
In Slovenia, the national IVT rate was estimated to be <3% before 2015. Available stroke services before 2015 included GHs with around-the-clock neurologic staff (24 h, 7 days per week—24/7), GHs with limited availability of neurologists only during regular working hours (8 h, 5 days per week—8/5), and GHs without neurologists (0/0). The only CSC was located in the capital city of Ljubljana. Only three GHs had an SU. The other GHs were equipped with standard intensive care units for critically ill medical patients. The system as it existed at that time did not allow appropriate coordination. To overcome these inconsistencies, we launched the national telestroke network, TeleKap. TeleKap has been established as an extension of the existing system merely offering optional support to attending neurologists and internists in treating AIS patients. The main aim of our telestroke network has been to enhance IVT use in Slovenia by using telemedicine. Thus, we established a hub-and-spoke system covering the entire nation. We hypothesized that TeleKap could enhance IVT use throughout the country.
Materials and Methods
Infrastructure
Slovenia is a mostly rural country with a population of two million inhabitants and covers a surface area of 20,273 km2. Population density is very variable, ranging from over 1,000/km2 in Ljubljana, the capital town, to only 5/km2 in some Alpine regions. TeleKap conforms to the decentralized hub-and-spoke model. Given the relatively small size of Slovenia, we set up a nationwide stroke care telemedicine system covering the entire country. The network started operating on September 15, 2014, and is approved by the appropriate authorities. The service is fully reimbursed by the Health Insurance Institute of Slovenia. A map of the national TeleKap network is depicted in Figure 1.

The Slovenian national TeleKap network (adapted with permission from
Spokes are classified according to the availability of a neurologist. There are two around-the-clock neurologist spokes (24/7). Around-the-clock neurologic expertise is also available at the university medical centers (UMCs) in both Ljubljana and Maribor. There are six spokes with 8/5 neurologic expertise. Outside regular working hours, these spokes have access to neurologic expertise via telemedicine only. There are two 0/0 spokes without a neurologist, which rely entirely on neurologic expertise via telemedicine. UMC Ljubljana (UMCL) is the foremost hub hospital covering the entire nation in regard to 24/7 comprehensive stroke care, including endovascular treatment (EVT). Additionally, UMCL offers the only neurologic critical care unit, 24/7 neurosurgical expertise, and an SU. The emergency neurologic department (END) at the UMCL is also one of the beneficiaries of teleconsultations in the network, especially if a junior neurologist or a neurology resident is the attending physician. UMC Maribor (UMCM) has not been asking for teleconsultations in TeleKap regarding IVT in their own patients but has been participating as the hub for neurosurgical patients from its spokes. At the same time, UMCM is not yet the hub for EVT in AIS patients from its spokes, who have been transferred to UMCL. Hopefully, UMCM will emerge as the second neurovascular center with 24/7 availability of EVT and, with an anticipated further increase of teleconsultations, will become the second teleconsultation center in future. Currently, there are only three SUs in Slovenia, and only one of them is outside the UMCs.
The technical equipment in the TeleKap center consists of a dedicated stationary workstation with an HD videocamera (Polycom® High Definition Group 700) and a high-quality microphone (Polycom RealPresence), enabling two-way teleconsultations. Dedicated mobile workstations (with an integrated HD videocamera and microphone) allow teleconsultations from home with the same quality as videoconferencing from the TeleKap center. Spokes are equipped with a mobile telemedical cart consisting of a fully remotely controlled HD videocamera, HD display, and microphone (Polycom RealPresence). Videoconferencing is enabled at a resolution of at least 720 p HD at 60 fps. The servers and software used in the network are part of the Slovenian medical network “eZdravje” (English: “eHealth”). Safety and confidentiality are ensured through safe connections over the closed Z-NET® network, which is an integral part of eHealth. There is a platform for reviewing neuroradiological images in DICOM® format (XERO® Viewer; Agfa HealthCare).
AIS versus Stroke Mimics
In TeleKap, we establish the clinical diagnosis of AIS on the recognition of typical stroke symptoms and consistent findings on neurologic examination, including the National Institutes of Health Stroke Scale (NIHSS) score. This is corroborated by multimodal computed tomography (CT) imaging, including non-contrast brain CT and aortocervical CT angiography, in every patient with suspected AIS. CT perfusion is being used increasingly but is limited to both UMCs and three spoke hospitals. MRI is not part of the standard imaging protocol, and we perform it only in exceptional cases predominantly in both UMCs (e.g., pregnant women, very rarely in wake-up AIS). Standard laboratory work-up is simultaneously performed. To increase the diagnostic accuracy of AIS versus non-vascular stroke mimics based on clinical grounds alone, we find the recently proposed TeleStroke Mimic Score as a useful adjunct in clinical decision-making even in TeleKap. 2
Workflow
The TeleKap network operates on a 24/7/365 schedule. Telemedicine comprises telephone contact between a physician at a spoke center and a consultant vascular neurologist, transmission of digital images, and real-time clinical examination of patients via videoconferencing. It is not mandatory for a treating physician to consult TeleKap for every patient suspected with AIS. A spoke physician asks for a teleconsultation at his/her own judgment. A dedicated stroke team assists in the workflow at spoke hospitals, including a nurse. Every spoke is able to provide hyperacute ischemic stroke care as well as further medical care of such patients. A telemedical follow-up can be requested at any time during the in-hospital stay for care-related issues.
Data Collection and Statistical Analysis
We analysed the data of patients treated in the TeleKap network from January 1, 2015, to December 31, 2017 (observation period). We used linear regression to determine the trends. The IVT rate was calculated as the ratio between the absolute number of IVT patients and the absolute number of AIS patients in a given year. We tested the differences between the groups with Student's t test. For every statistical test, p < 0.05 was regarded as statistically significant.
Results
During the observation period, we treated a total of 2,224 patients. The demographic data for a subgroup of 2,165 patients are available, of which there were 1,094 (50.5%) males. A total of 1,219 (56.3%) patients were aged >70 years. We treated a total of 1,316 patients (59.2%) with AIS, of which 508 (38.6%) received IVT. There were 142 IVT patients in 2015, 158 in 2016, and 208 in 2017. The absolute numbers of AIS patients and IVT patients increased, as depicted in Figure 2. Linear regression showed statistically significant positive trends in the absolute number of IVT patients (B = 4.39, standard error (SE) = 1.59, p = 0.011) and the absolute number of AIS patients (B = 14.42, SE = 5.19, p = 0.010). The trend of IVT rate was numerically negative (43.5% in 2015, 37.3% in 2016, and 36.7% in 2017), although not statistically significant (p = 0.302). We treated a total of 591 (26.5%) patients with nonvascular neurologic conditions, of which we identified 261 (16.6% of 1,577 patients with suspected AIS) patients with stroke mimics (almost a half of them due to postictal neurologic deficit or encephalopathy).
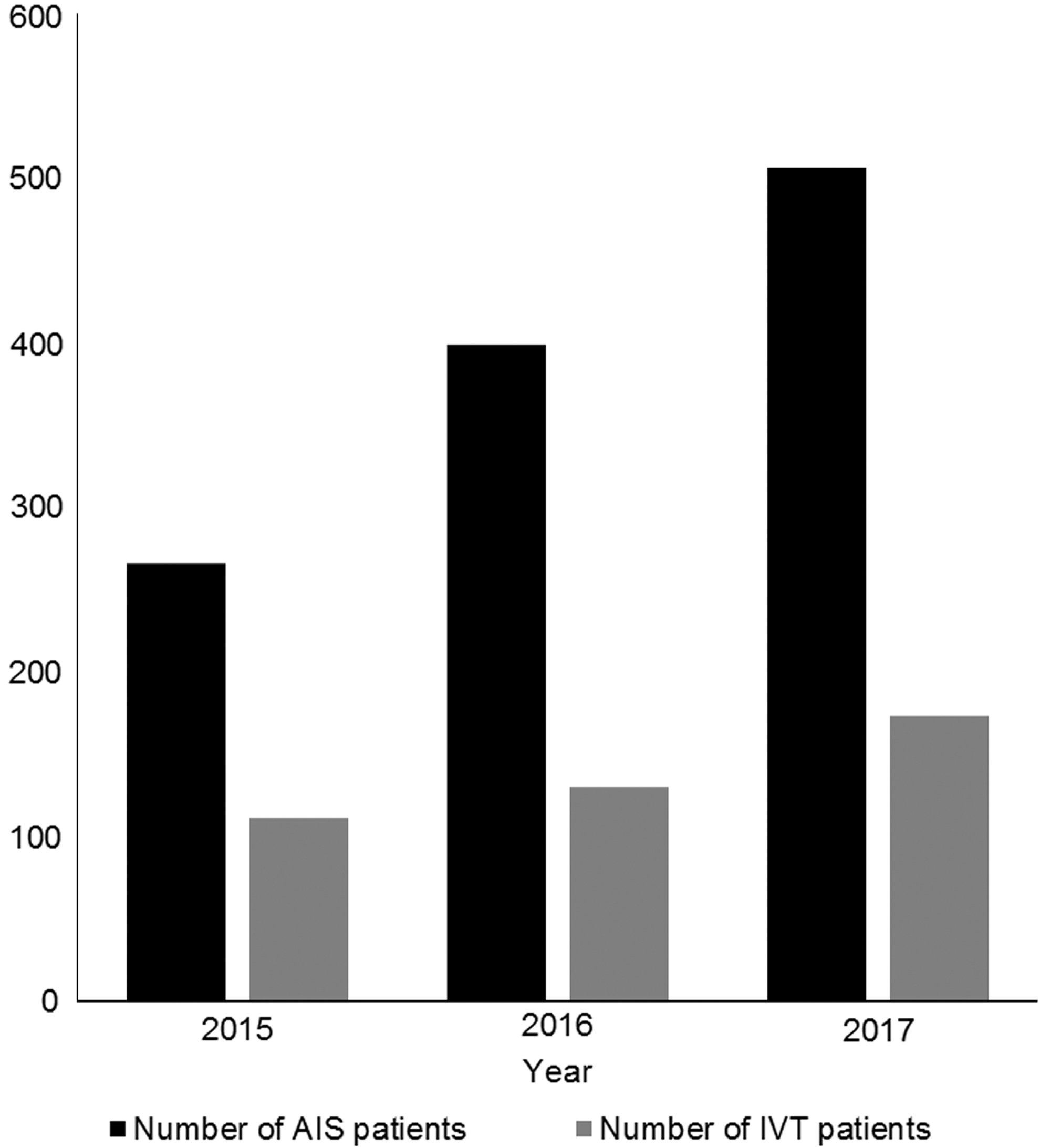
Absolute numbers of patients with AIS and patients treated with IVT from 2015 to 2017. AIS, acute ischemic stroke; IVT, intravenous thrombolysis.
We analyzed the trend of IVT patients in different types of spokes (Fig. 3). In our foremost 24/7 spoke, GH Celje, we found statistically significant positive trends in the absolute number of AIS patients (B = 8.75, SE = 0.14, p = 0.022) and the absolute number of IVT patients (B = 4.25, SE = 0.14, p = 0.011). However, the IVT rate in the 24/7 spoke did not change sufficiently to reach statistical significance (54.0% in 2015, 52.2% in 2016, and 51.8% in 2017; p = 0.204).
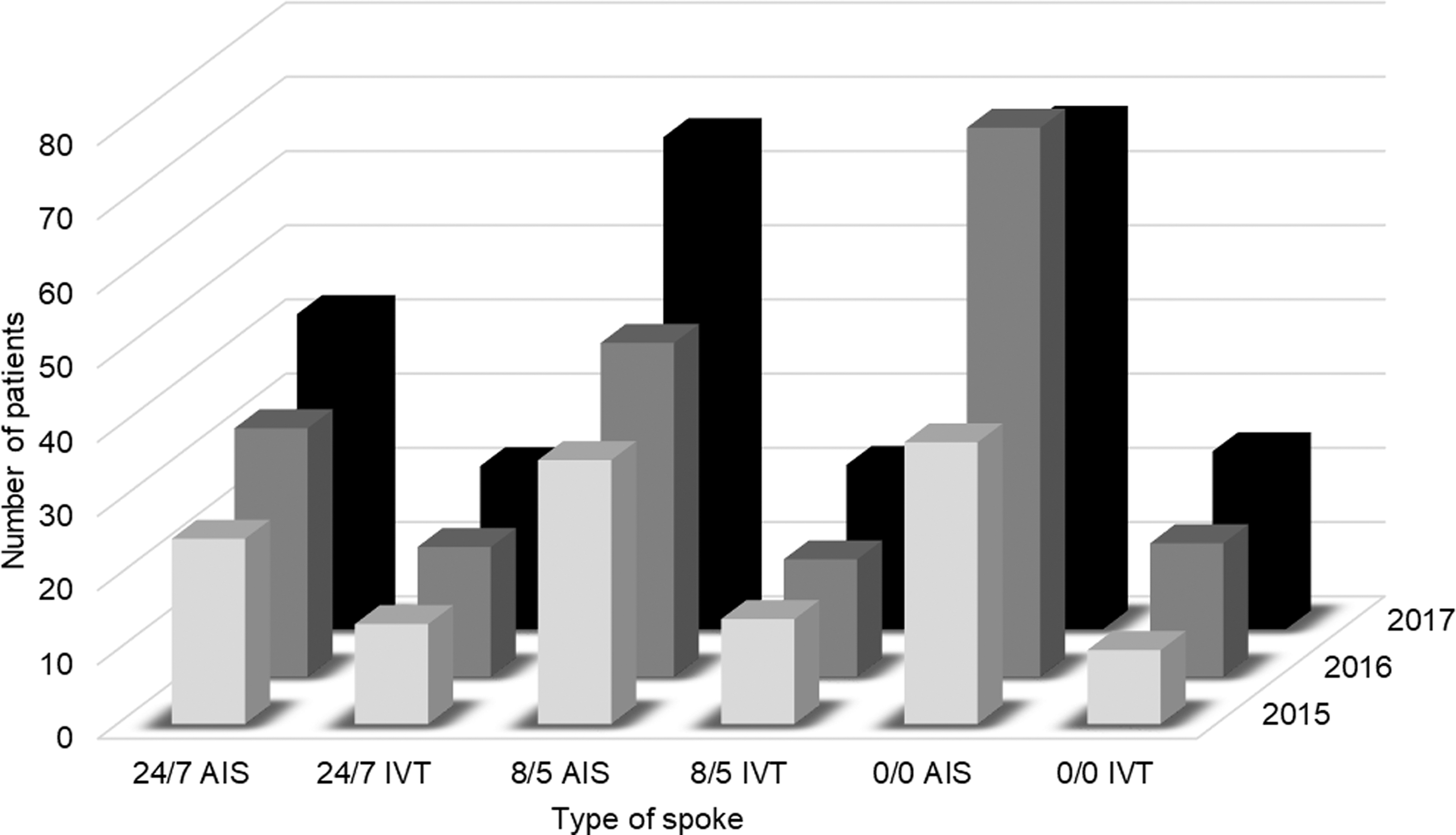
The mean number of AIS patients and the mean number of patients treated with IVT in 24/7, 8/5, and 0/0 spokes. AIS, acute ischemic stroke; IVT, intravenous thrombolysis.
In 8/5 spokes, we found statistically significant positive trends in the absolute number of AIS patients (B = 15.56, SE = 7.21, p = 0.048) and the absolute number of IVT patients (B = 4.00, SE = 1.74, p = 0.036). The IVT rate did not show a statistically significant trend (39.8% in 2015, 35.2% in 2016, and 33.4% in 2017; p = 0.249). We found a statistically significant difference in the IVT rate between 24/7 and 8/5 spokes (p = 0.007).
In a 0/0 spoke, we found a borderline statistically significant positive trend in the absolute number of IVT patients (B = 7.00, SE = 0.58, p = 0.052). However, the trends in the absolute number of AIS patients (B = 15.00, SE = 12.12, p = 0.433) and the IVT rate did not reach statistical significance (26.3% in 2015, 24.3% in 2016, and 35.3% in 2017; p = 0.442). The difference in IVT rate between 24/7 and 0/0 spokes was statistically significant (p = 0.016). We did not find a statistically significant difference in IVT rate between 8/5 and 0/0 spokes (p = 0.144).
In the 24/7 spoke GH Celje, the absolute number of IVT patients showed an upward trend after the initiation of the network in 2015, further increasing in 2016, compared with the years before the introduction of the network; the trend almost reached statistical significance (p = 0.05). The trend in the absolute number of telestroke-assisted IVT patients in GH Celje was positive and reached statistical significance (p = 0.02). There was no rising trend in the number of IVT patients before 2015 in GH Celje (p = 0.38) (Fig. 4).
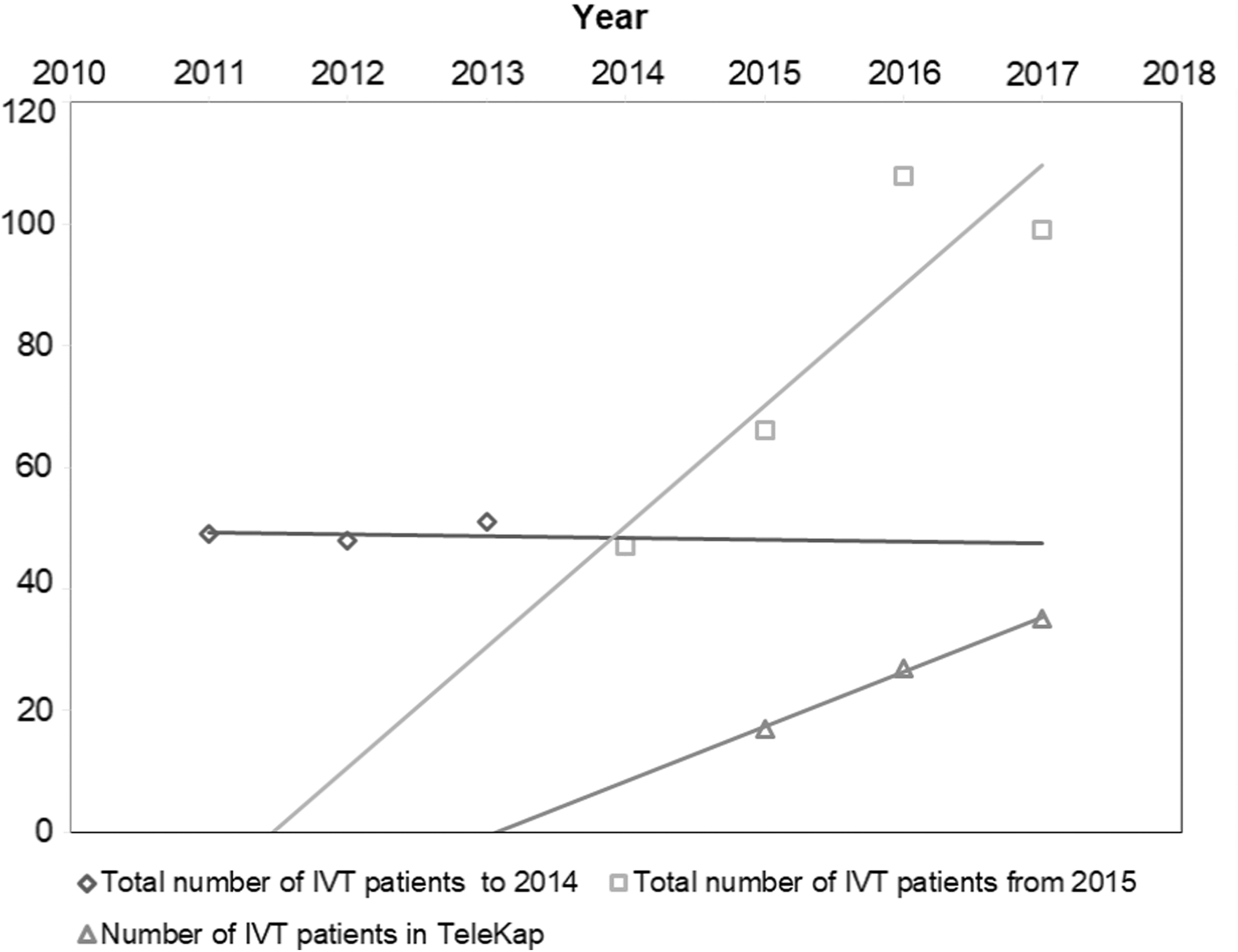
Trends of IVT use in a 24/7 spoke GH Celje before (2011–2014) and after inclusion in the TeleKap network (2015–2017). GH, general hospital; IVT, intravenous thrombolysis.
At the UMCL, the absolute number of IVT-treated patients did not change significantly during the observation period (p = 0.33). Similarly, the absolute number of telestroke-assisted IVT patients did not differ significantly from 2015 to 2017 (p = 0.18). The IVT rates were 57.1% in 2015, 40.0% in 2016, and 47.4% in 2017. The trends of IVT rates at the UMCL (hub hospital) did not significantly differ from those at 24/7 spokes (p = 0.46).
Regarding the whole network, our analysis showed significant positive trends in the absolute number of AIS patients (B = 7.66, SE = 0.59. p < 0.001) and in the absolute number of IVT patients (B = 2.16, SE = 0.56, p = 0.003). Furthermore, there was a significant positive trend in other diagnoses, principally nonvascular stroke mimics (B = 3.58, SE = 0.90, p = 0.003).
Discussion
The main finding of our study is a constant, progressive increase in the absolute number of IVT patients in the TeleKap network. In addition, we found a statistically significant progressive increase in the absolute number of AIS patients. At the same time, we did not observe significant changes in the IVT rate. The analysis showed a significant relationship between teleconsultations and IVT use.
The reported high IVT rate in the network is comparable with those in some other networks 3 and merits further clarification. Since there is no national stroke registry in Slovenia, we can only estimate as to what extent TeleKap contributed to the elevated national IVT rate. According to these estimations, the national IVT rate has increased to 8.6% during the last 3 years, 4 which is substantial given that <3% of AIS patients received IVT before 2015. But the national IVT rate is still far below the IVT rate inside TeleKap. This high rate reflects the fact that TeleKap does not include all IVT patients in the country. Only a minor share of all AIS patients in Slovenia have been treated thus far in TeleKap. TeleKap has been designed merely as an additional support of the existing AIS care system and not as a mandatory part of AIS care for every (suspected) AIS patient. Many AIS patients have been treated by attending neurologists in UMCs and spoke hospitals during regular working hours outside TeleKap. We believe that AIS patients treated in TeleKap are primarily highly selected patients often eligible for IVT. This consideration is the main reason the IVT rate is so high, which is in stark contrast with the Telemedical Project for integrative stroke care in the region of southeastern Bavaria (TEMPiS [in German]) network (IVT rate of 16.7% according to recent data 5 ), where virtually every patient with suspected AIS is treated inside the network. We expect that with further years of TeleKap activity, internists from spoke hospitals will increasingly opt for teleconsultations, which will further decrease the IVT rate inside TeleKap and bring it closer to the rate of most other telestroke networks.
In contrast, it seems that the awareness of AIS as a fundamental medical emergency among emergency medical services has noticeably improved. Thus, an increased number of stroke sufferers reach spokes during the treatment window for IVT. Our hub-and-spoke model has been designed with daytime IVT provided by a local spoke (in case of 8/5 spokes) and coverage outside regular working hours provided by the TeleKap center by means of teleconsultation. A Finnish pilot study found a high percentage of teleconsultations leading to IVT in spokes with features, and results very similar to on-site IVT in a CSC, which translated into the enhancement of IVT rate in spokes. 6
We found a significant increase in the total number of IVT patients in a 24/7 spoke after the initiation of the network, which was also true for patients who did not undergo telestroke-assisted IVT. Both trends were significant during the entire observation period. This may be due to improved prehospital management and especially higher level of expertise of in-house neurologists, achieved through practice-based education. Thus, the enhancement of IVT use can be observed in a spoke with permanent on-site neurologic expertise. However, we did not observe a significant change in the total number of telestroke-assisted IVT patients at the tertiary END UMCL, where there is also a 24/7 neurologic expertise available. This discrepancy can be explained by the additional experience of a neurologist at the CSC. For instance, four of the TEMPiS hospitals also have 24/7 neurology service, and telemedicine has been used in these hospitals mainly for second opinions and organization of transport. 7 Thus, TeleKap showed benefits in spokes with permanent neurologic expertise.
The absolute number of IVT patients in a 0/0 spoke shows a positive trend with a stronger enhancement effect than other spoke types. This effect could be due to better recognition of IVT candidates because of staff education provided by TeleKap. Simultaneously, we did not find a statistically significant increase in the absolute number of AIS patients despite a positive but nonsignificant increase in the IVT rate. Indeed, the number of AIS patients decreased in 2017, which may have contributed to a higher IVT rate. An explanation may be that teleconsultations were conducted for all patients with AIS, and the response time of teleneurologists might have been shorter. The positive trend may be attributed to improved prehospital management of patients with AIS. In addition, internal medicine specialists in 0/0 spokes could have grown more familiar with AIS management. Another explanation for this considerably high IVT rate could be that it is a GH covering a small area (∼300 km2 with about 30,000 inhabitants) with short travel times so the AIS patients arrive considerably earlier and more of them become eligible for IVT. Therefore, even a 0/0 spoke can be highly effective.
In 8/5 spokes, we observed a moderate enhancement of IVT use. In the Finnish telestroke model, the combination of daytime on-site neurologic expertise and night-time teleconsultation also resulted in a high IVT rate and favorable outcomes. 6 Advanced education of a classical neurologist could be the driving force. Presumably, better prehospital management of AIS patients and education in the network were additional factors that improved IVT use. It is interesting that the IVT rate was higher in 24/7 spokes than in 8/5 spokes. This difference may be attributable to the higher level of expertise in 24/7 spokes. We did not observe any difference in IVT rates between 8/5 and 0/0 spokes. The level of expertise seems to have increased even in 0/0 spokes.
Telestroke offers the ability to link rural hospitals and those with lower volumes of stroke patients with CSCs. 8 It is well known that difficulties may arise in very scarcely populated areas where IVT volume is low. Many of our spokes have a low IVT volume, and consequently, the level of experience is low. Therefore, TeleKap enables sharing of stroke expertise from a CSC to spokes and contributes to optimal care.
It is known that AIS diagnosis is not straightforward. The frequency of stroke mimic admissions varies extensively, ranging from 1% to 30% of all strokes, being lower in hospitals with higher neurologic expertise. 9 Therefore, it is very important to have a neurologist available in a spoke at least during regular working hours. 10 In the TeleKap network, nonvascular emergency neurologic patients represented >25% of all teleconsultations, so we are considering general teleneurology coverage in the future.
The national TeleKap network enhanced IVT use in AIS patients in Slovenia. The enhancement was observed in all spoke types. The availability of permanent neurologic expertise in spokes is not mandatory for enhancement. The TeleKap network is indeed exclusive in two major points: it covers the whole nation and is seemingly the first functioning telestroke network in an Eastern European country. This network may, when adapted, serve as a model of telestroke care for other similar countries.
Footnotes
Acknowledgments
We express our gratitude to Mrs. Mojca Blejec for her assistance in preparing the data; to Mr. Ivan Mori for his assistance in graphic design; and to all consultant vascular neurologists of TeleKap for their willingness to participate in the network and for sharing their time, expertise, and ideas. The Ministry of Health of the Republic of Slovenia has financially supported the TeleKap network and this research.
Disclosure Statement
No competing financial interests exist.