
Abstract
Introduction:
Many patients struggle with colonoscopy preparation, which is complex and can be an uncomfortable as well as a time-consuming process. The confusion and anxiety from the preprocedure process may lead patients to delay their colonoscopy or skip it altogether. Digital health technology that focuses on patient engagement can play an important role in promoting colorectal cancer screening.
Methods:
A digital preprocedure instruction program was implemented for outpatient colonoscopy by sending critical reminders and instructions to patients through a series of short message service messages and/or emails. Eligible patients included English speakers on GoLYTELY®/NuLYTELY® or MiraLAX® preparation regimens with a valid cellphone or email address in the electronic health record. We examined the impact of digital instructions on bowel preparation quality, no-show and same-day cancellations over a 3-month period between an intervention group of 756 patients and a control group of 2,103 patients. Patients who enrolled in the digital instructions also received a patient satisfaction survey.
Results:
Our controlled study demonstrated the effectiveness of digital instructions to reduce no-show and same-day cancellation rates for outpatient colonoscopy from 10.40% to 6.08% (p < 0.001). Bowel preparation quality was not significantly different between the two groups (p = 0.23). However, 90% of patients who enrolled in the program rated their satisfaction with the digital reminders very highly.
Discussion:
A digital preprocedure instruction program can have a positive impact on operational efficiency, quality of care, and patient satisfaction. This study shows how digital health tools can effectively engage patients scheduled for a colonoscopy, increase appointment adherence, and, therefore, lead to better cancer screening.
Introduction
Utilization of digital applications and devices has increased to improve patient engagement and quality of care. Doctors and health care teams effectively communicate with patients and access medical information via smartphones. 1,2 Other patient-centered technologies have been built to improve health outcomes among a population that is becoming more tech savvy. 3,4 According to the 2017 Pew Research Center Survey, 77% of Americans now own a smartphone and among Americans 50 years and older, nearly three-quarters (73%) are smartphone owners. These individuals use their mobile devices to text message, access the internet, and check emails. 5 By leveraging on technologies that are already a part of patients' everyday lives, digital messaging programs can be potentially powerful tools in the health care setting.
Despite investments aimed at optimizing efficiency and improving the delivery of care, many health care systems still struggle with simply getting patients to their appointments on time or at all. 2,6 Research from various endoscopy outpatient clinics show a range between 12% and 40% in missed appointments. 7 –10 Colonoscopy appointment adherence presents a challenge, as patients are required to follow rigorous and time-sensitive steps in preparation for their exam. Patients must adhere to a strict dietary regimen, which consists of consuming a large volume of unpalatable fluids to purge their bowels before the exam. 11 This preparation can be stressful for patients, who often underestimate the amount of time and complexity involved, leading patients to cancel or reschedule at the last moment. This lack of adherence to medical appointments can lead to operational inefficiencies and potential increased patient risk for interval cancer. Moreover, even if the patient arrives for their colonoscopy, inadequate bowel preparation remains a major issue. 11,12 Colon prep has been noted to be less tolerable by patients due to its poor tasting solution, dietary modifications, and forced adjustment to work schedule. 12 Inadequate bowel preparation has been associated with poor visualization of mucosa, incomplete examination, prolonged procedure time, and high costs. 13,14
To address the issues of poor appointment adherence and suboptimal endoscopic outcomes, a digital platform for patient education and reminders was developed and implemented for a subset of the outpatient population at a large academic medical center. The program was designed to send brief instructions and reminders via short message service (SMS) message or email to the patient at specific points during the prep process. Messages were customized based on the patient's scheduled procedure date and time, location, and prescribed preparation regimen as captured in the endoscopy scheduling system. Patients received messages starting 2 weeks from their scheduled appointment date and they were delivered according to a defined schedule. Some messages also included a link to a specific online module carrying additional detailed instructions in the form of text, graphics, and/or video education. These message types were chosen for this program rather than an application, as they eliminated the additional step of having to download an application to the patients' mobile device or computer.
The goal of the intervention was to keep patients engaged throughout the week-long prep process to ensure that they arrived at their appointment on time and were properly prepared. The larger aim of the project was to reduce the no-show and same-day cancellation rates and improve the prep quality in the outpatient population.
Methods
Design
This research was conducted at a large academic medical center. We collaborated with Medumo (Boston, MA), a digital health solution company, to transform our paper colonoscopy preparation instructions into digital form. This study focused on adult outpatient colonoscopy and is an extension of a previously successful uncontrolled pilot study completed from May 1, 2017 through June 30, 2017. This extended study, which ran from February 1, 2018 through April 30, 2018, was controlled and scaled to a larger patient population to assess the impact of the digital instruction program on no-show and same-day cancellations, bowel preparation quality, and polyp detection rates. Patient engagement and satisfaction with the digital instruction program were also measured. The intervention group continued to receive the standard of care paper prep instructions, in addition to the new digital instructions in their preferred format (SMS message and/or email). This study was an exempt IRB review due to its classification as a quality improvement project.
Selection of Intervention and Control Groups
Thirteen out of the 34 endoscopists with representative practices volunteered to be a part of the program to test for scalability and future practice-wide implementation. Inclusion criteria were adult outpatients on Standard (GoLYTELY®/NuLYTELY®) or MiraLAX® prep, English literate, had a valid mobile phone number or email address in the electronic health record (EHR), and who were scheduled at one of the participating endoscopy centers. Eligible patients were automatically enrolled shortly after they were scheduled, and patients could unsubscribe from the digital messages at any time. Patients in the intervention group who chose to opt out of the program (n = 20) were excluded. Other exclusion criteria included age younger than 18, non-English-speaking, received alternative bowel preparations, and invalid mobile phone number or email address listed in the EHR. To control for the seasonal variations of our short-term study, the intervention group was compared with a contemporaneous control group consisting of English-speaking patients receiving care from the remaining non-participating providers (n = 21). 15 The participating endoscopy sites were located at the main medical center campus. We extracted patient information, date and time of the scheduled procedure, scheduling status, and final disposition from our EHR from February to April 2018 (n = 2,363). Our study primarily examined no-show and same-day cancellations as these last-minute cancellations have disruptive effects. We excluded patients who provided 24-h notice because early cancellations or rescheduling demonstrate better patient education and planning. The final cohort only includes patients who arrived and completed their exams, canceled within 24 h of their procedure, or who did not attend their scheduled appointment. This left a total of 756 and 2,103 in the intervention and control groups, respectively.
Clinical Metrics
For patients who arrived for their procedure, bowel prep qualities of the two groups were also compared. A patient's prep was classified as “acceptable” if it was reported by the endoscopist as “Excellent,” “Good,” “Adequate,” or had a Boston Bowel Preparation Scale (BBPS) score of 5 or higher. A patient's prep was classified as “unacceptable” if it was reported as “Fair,” “Poor,” “Unsatisfactory,” “Inadequate,” or had a BBPS lower than 5. A “Complete” procedure was achieved if the scope reached cecum, the ileocecal valve, or terminal ileum. A procedure was deemed “Incomplete” if it was aborted or the scope only reached the anus, rectum, sigmoid colon, splenic flexure, or transverse colon. Polyp detection rate was defined as the number of colonoscopies in which polyps were detected as a percent of total colonoscopies performed for all indications.
Patient Engagement
Patient engagement was measured by determining the number of online modules viewed by each patient. Timestamped activity indicated when patients opened each SMS or email message; however, we were unable to ascertain whether patients read through each additional page.
Patient Satisfaction
On completion of the colonoscopy procedure, an 11-item patient satisfaction survey consisting of multiple choices using a 5-point Likert scale and open-ended questions was administered to all patients enrolled in the digital instruction program (Appendix A1). The survey was sent immediately after the scheduled procedure date regardless of whether the patient had completed its exam. In addition to patient satisfaction, the survey assessed technical issues encountered, preferred instruction delivery method, and the perceived value of the program for enhancing bowel preparation and appointment adherence.
Statistical Analysis
Data were analyzed for differences with statistical significance (p < 0.05) between the two groups. Descriptive statistics were compared by using independent t-tests for continuous variables and chi-square tests for categorical variables. Multivariate logistical regression analyses were performed to determine the significance, odds ratio (OR), and corresponding 95% confidence intervals (CIs) of various predictive factors for no-shows. Predictive factors were only assessed among the study cohort, since the equivalent variables were not available for the intervention group. We selected the variables in the model because we were interested in understanding different characteristics and behaviors that can inform potential preventive strategies. Statistical analysis was performed by using R Statistical Software® (version 3.5.0; R Foundation for Statistical Computing).
Results
A total of 756 patients were enrolled in the digital instruction program (intervention group). We identified a total of 2,103 elective outpatient colonoscopies scheduled in the control group that fulfilled the inclusion criteria. The control and intervention groups were comparable with a few differences (Table 1). Males and females were distributed similarly within the two groups (p = 0.06). Most of the patients were white (57% vs. 59%, p = 0.74). The mean age of the intervention and control group was 57 ± 12.5 and 59 ± 11.9 years, respectively. We used zip codes as a proxy to determine the median income by household provided by the U.S. Census Bureau, 2012–2016 American Community Survey 5-year estimate. We found no difference between the two groups in median household income level below and above $50,000 (p = 0.91). The most common indication for outpatient colonoscopy among both groups was screening for colorectal malignant neoplasm followed by colorectal cancer (CRC) surveillance with a personal history of adenomas or polyps. The intervention group had a higher indication for assessment of Inflammatory Bowel Disease compared with the control group (8.73% vs. 2.81%, p < 0.001) (Table 1). No significant difference was observed in cecal intubation rate and polyp detection rate. Bowel preparation quality was also not significantly different (p = 0.23). We found that patients in the digital instruction program did not demonstrate any deterioration in bowel preparation from its baseline. The combined no-show and same-day cancellations rate was significantly lower in the intervention group compared with the control group (6.08% vs. 10.40%, p < 0.001) (Fig. 1).
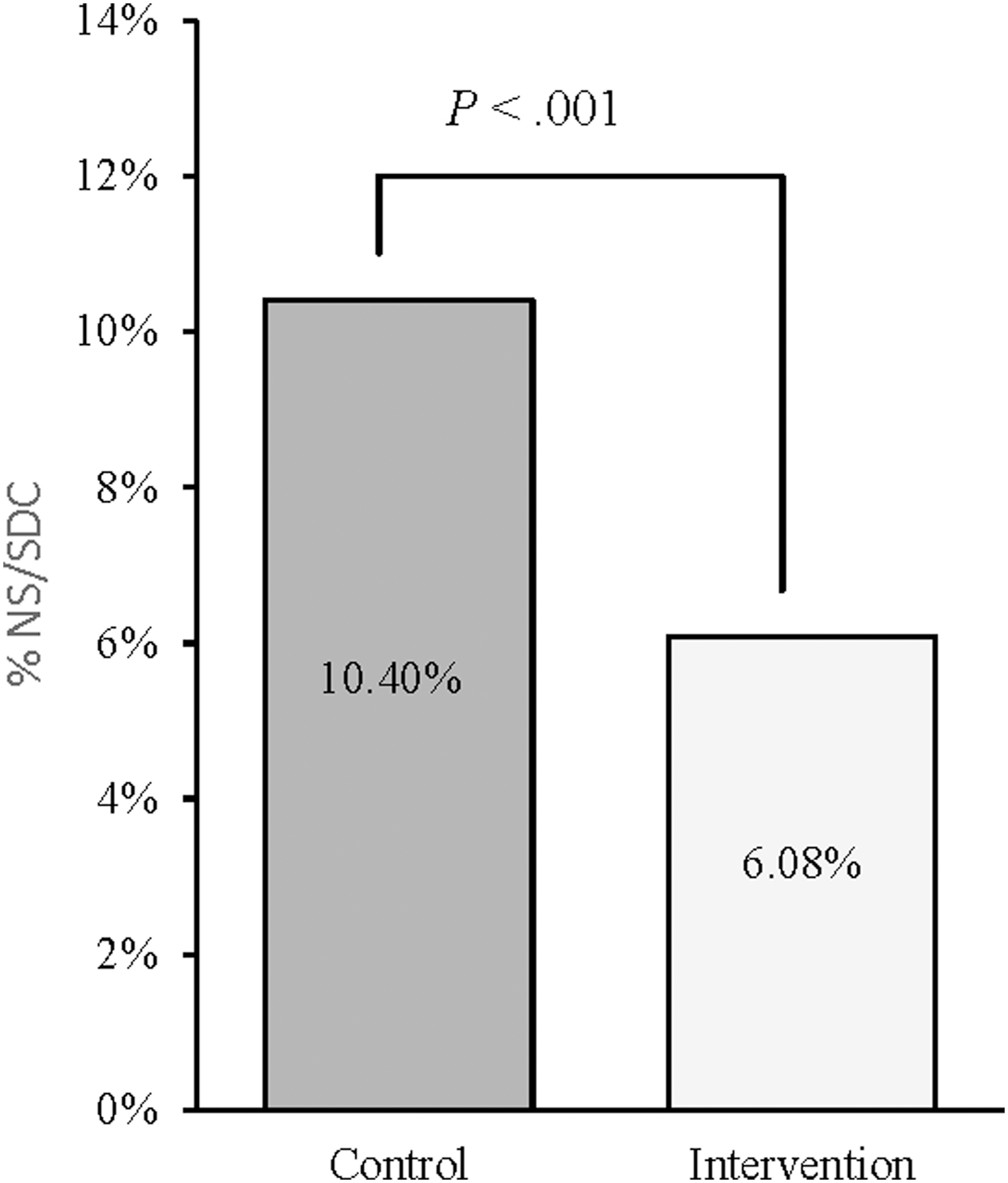
Overall no-show/same-day cancellation rates. Comparison of total no-show and same-day cancellation rates between the control and intervention group. Chi-square test; significance level of p < 0.05. NS, no-show; SDC, same-day cancellation.
Patient Characteristics and Quality Metrics of the Intervention and Control Cohort
Percentage does not add up to 100 because only the top 5 indications of both groups were compared.
Income based on U.S. Census Bureau, 2012–2016 American Community Survey 5-year estimate. Reports data on median household income for ZCTAs.
Polyp detection denominator includes all completed procedures except “Assessment of IBD” cases because the motive of colonoscopy is not to look for polyps.
CI, confidence interval; CRC, colorectal cancer; FH, family history; IBD, inflammatory bowel disease; SD, standard deviation; ZCTA, zip code tabulation area.
To analyze this further, we performed a multivariate logistic regression analysis to determine predictors of patient appointment adherence, including sex, age, income, and digital instruction engagement. In the logistic regression model, gender and the patient's level of engagement with the digital instruction program had a significant effect on appointment adherence (Table 2). However, patient engagement factor was a much stronger predictor than gender (p = 0.04 vs. p < 0.001). Level of engagement was characterized by the number of modules viewed by each patient. Patients who viewed five or more modules were 1.44 times more likely to arrive and complete their appointments than those who viewed four or less modules (p < 0.001). As presented in Figure 2, 97.9% of the patients who viewed at least five modules arrived and completed their procedure compared with 82.3% of the patients who viewed fewer than five modules (Fig. 2).
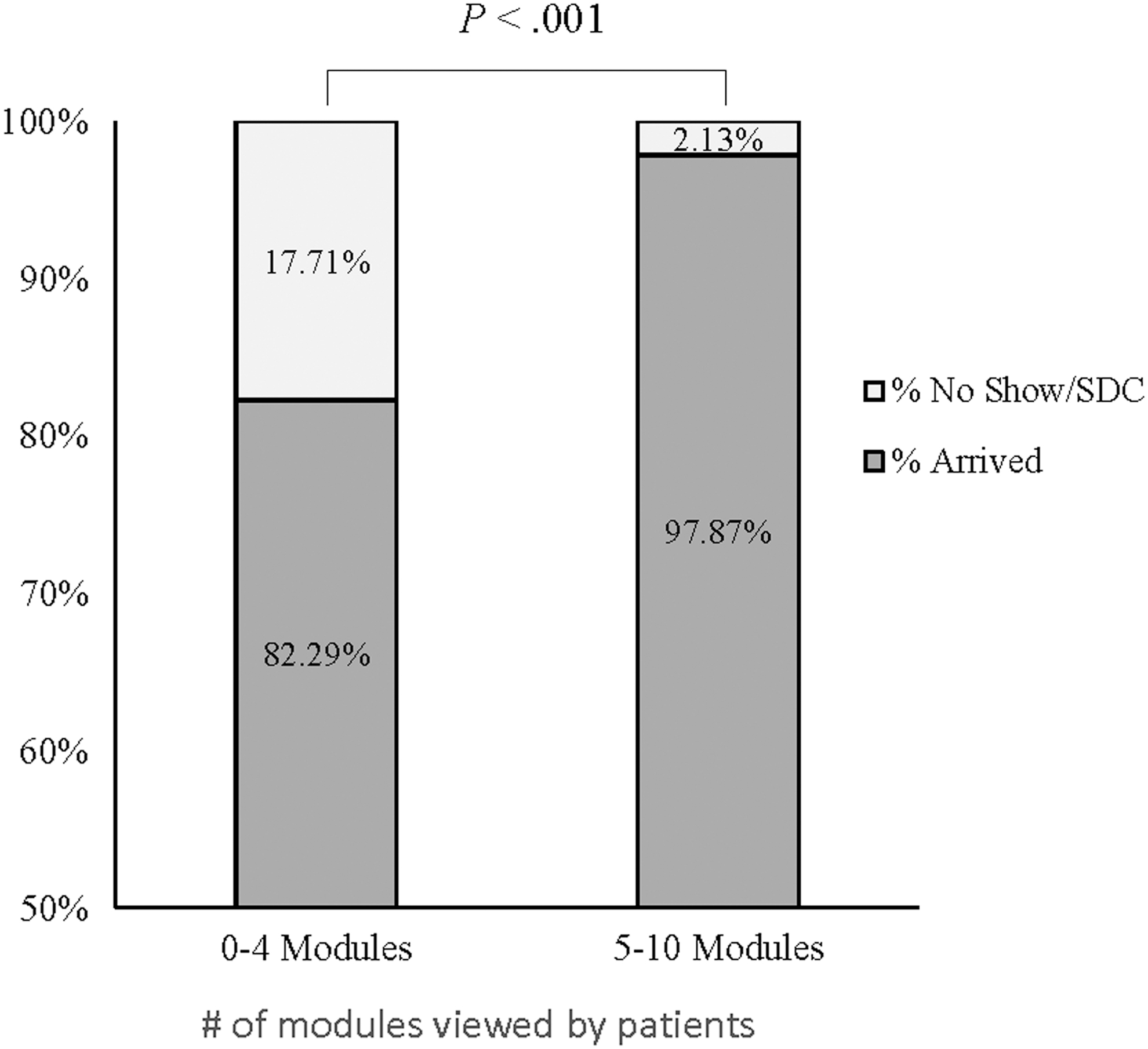
Effect of number of modules viewed on appointment adherence. Effect of patient engagement on appointment adherence among the intervention group. Stratified comparison of the no-show/same-day cancellation and arrival rates between patients who viewed 0–4 modules versus 5–10 modules of the digital instructions. Chi-square test; significance level of p < 0.05. SDC, same-day cancellation.
Effect of Demographic and Digital Instruction Engagement Factors on Appointment Adherence (N = 756)
Displays a multivariable logistic regression analysis to assess the effect of demographic and digital instruction engagement factors on appointment adherence (n = 756). Significant at the p < 0.05 level.
CI, confidence interval; OR, odds ratio.
Our analysis also shows that male patients were almost twice as likely (1/0.53 = 1.89) than their female counterparts to show up to their scheduled appointment (OR = 0.53, 95% CI, 0.28–0.98). Women in the intervention group accounted for 63% of the total no-show and same-day cancellations. In contrast, the control groups' total no-show and same-day cancellation rate for male and female was 53.4% and 45.6%, respectively. To understand technological usability and efficacy between younger and older users, we also examined age as a potential factor for adherence. We stratified those age <50 and those age ≥50 since 50 is the recommended age for a screening colonoscopy as per the U.S. Preventive Services Task Force. 16 Neither age nor income proved to have a significant effect on appointment adherence (Table 2).
After the completed procedure, patients who did not unsubscribe from the program received a patient satisfaction survey via the digital platform. The overall response rate was 58% (432/746). Among the 432 patients who completed the exam and submitted a survey, 90% said they would highly recommend the digital instruction program (rated 4 or 5) to a family member or friend; whereas only 2.6% said they would not recommend the program (p < 0.0001). In addition, 97% of patients indicated that they were highly satisfied with the overall care received at the hospital. Regarding the desired method for instruction delivery, 52.5% of the survey respondents said they prefer text message reminders as opposed to paper handouts; whereas 15.8% said they would still prefer paper handouts (p = 0.006). The survey results also showed that 72% were satisfied with the frequency of the reminders, and 63% indicated that they felt more confident in completing the prep (p < 0.0001) (Fig. 3).

Patient satisfaction survey responses (n = 432). The percentage shown are based out of the total number of surveys completed (n = 432).
Discussion
More patients are taking an active role in their health care, which is supported by technology to make health care information more easily accessible and patient-centered. Our digital platform attempts to improve bowel preparation and appointment adherence for outpatient colonoscopy by sending timely preprocedure instructions and reminders to patients. The digital reminders are equipped with various multimedia elements to simplify the instructions and further engage patients in the importance of a good prep. Although our results did not show significant improvement in prep quality, our recent adoption of the improved split-dose prep for all our patients may have blunted our ability to detect additional improvement in preparation outcomes. Nelson and Keswani suggest that SMS technology can be an important adjunct to colonoscopy preparations even when the overall bowel preparation quality is adequate, because amelioration of bowel preparations can increase the likelihood of detecting sessile serrated polyps. 17
We also elicit patients' perspectives on the program by asking them about their user experience. Our study demonstrated high patient satisfaction and was notable for decreasing the total no-show and same-day cancellation rate by more than 40%. Some studies have shown that implementation of higher cost programs such as patient navigators can improve both patient appointment adherence and prep quality, although some report nonsignificant results. 18 –20 Here, we demonstrate how a lower cost digital navigation program can have a positive impact on appointment adherence.
Our results coincide strongly with other studies reporting on the use of mobile applications to improve appointment adherence. Leffler et al. showed that an alert system to remind patients of their next colonoscopy screening increased adherence to surveillance recommendations by 30%. 21 A randomized control trial done by Lin et al. found that text message reminders decreased no-show rates in a pediatric clinic from 38.1% to 23.5% (p < 0.04). 22 With a low per patient cost as well as decreased no-show rates (and therefore decreased lost revenue), we predict that the digital instruction program could positively impact the endoscopy unit's budget.
Patient no-shows and late cancellations represent a huge loss of productivity and cost burden on the health care system. A cost analysis using micro-costing and time-and-motion technique showed that the median direct cost of a colonoscopy was $379 in 2004. 23 This was a small study, however, performed at two sites with a unique patient population, limiting the generalizability. Payments are highly variable and are often around $800 per procedure. Consequently, missed or delayed appointments are not only disruptive to a practice but also represent millions of dollars in lost revenue and fixed overhead for many programs that cannot be recouped.
In addition to facilitating attendance, our findings also shed light on the importance of adapting health information and communication to digital form for enhancing patient engagement. We found that the level of patient engagement with the program is a critical factor for appointment adherence. Patients were more likely to arrive to their appointments when they viewed five or more modules. The results of our patient satisfaction survey also pointed toward the importance of engagement, as 63% of respondents reported feeling more confident in completing the bowel prep, along with 90% saying that they would highly recommend the digital instruction program. Among low-income and minority populations, rates of CRC screening remain low, putting these groups at risk for developing the disease. 24,25 A program aimed at increasing CRC screening rates among these groups found that the most common reason for nonadherence to colonoscopy was related to patient readiness (60.7%). 26 For non-native English speakers, it is critical to deploy a multi-faceted approach, such as SMS messaging and videos, to increase comprehension of the written instructions. 17 Therefore, an SMS program presents an opportunity to improve patient education by engaging with at-risk populations in multiple languages, reading levels, and visual mediums.
Conclusions
Our study had some limitations. The intervention and control groups were not randomized, so the characteristics of the patients were similar. Some of the differences in the clinical indications could have affected our outcomes. Future research could study patients undergoing first-time screening colonoscopy to assess the impact of a digital instruction program on bowel preparation for patients without any prior experiences.
We also acknowledge that this study spanned over a 3-month period where weather, including several snowstorms, could have inevitably affected arrival, cancellation rates, and patient prep quality but equally impacted both groups. We also did not have measures of employment status, which is a potential barrier in colonoscopy completion. Chang et al. found that active employment was associated with a 62% lower probability of endoscopy no-show. 8 Despite similar demographic and socioeconomic characteristics in the intervention and control groups, differences in patient employment status could have affected appointment adherence. Lastly, about half of the nonparticipating providers in the control group were part of a simultaneous appointment adherence effort, which involved confirmation calls reminding patients of their appointments. Nevertheless, our intervention group still performed significantly better than the control group in appointment adherence. This has major implications of the use of a digital tool to optimize administrative resources and alleviate staff burden from reduced outbound phone calls.
Our multifaceted digital instruction program was successful in improving attendance rate for scheduled appointments and enhancing patient education and overall satisfaction. By connecting digitally with patients through SMS messages and email, we were able to effectively engage and motivate patients through each step of the prep process, which is essential to improving care and increasing screening rates. Our digital program was cost-effective (estimated $3/patient), but the current market rate is competitive. This platform and others alike are commercially available. As the health care system shifts to a value-based model, an important resource will be health care technology to achieve efficiency and greater patient satisfaction. 27 Moving forward, it would be important to refine and implement these instructions in other languages, such as Spanish, to reach more underserved populations with low CRC screening rates.
Footnotes
Acknowledgments
The authors thank Medumo for their service in providing a customized platform for digital patient education through an SMS and email reminder system for colonoscopy preparation. The following people provided assistance in data acquisition: Adeel Yang, MD, Aiden Feng, MD, Rohit Singh, MBA, and Katrina Bennett, BA.
Disclosure Statement
No competing financial interests exist.
Appendix A1 Patient Satisfaction Survey
Page 1 of 11
Would not recommend 1–5 Would highly recommend
Page 2 of 11
Not satisfied 1–5 Very satisfied
Page 3 of 11
[Free Text]
Page 4 of 11
A. Paper handout
B. Emails
C. Texts
D. No preference
Page 5 of 11
A. Way too many reminders
B. Too many reminders
C. Just the right number of reminders
D. Too few reminders
E. Way too few reminders
F. Other
Page 6 of 11
A. Within the text messages and/or emails
B. Within the digital instruction program
C. On the paper handout
D. I searched online
E. Other
F. I did not use/need clinic contact information
Page 7 of 11
1 (not at all helpful) to 5 (very helpful)
I do not remember the Home Page
I remember the Home Page, but I did not use it
Page 8 of 11
1 (not at all helpful) to 5 (very helpful)
I do not remember the Timeline
I remember the Timeline, but I did not use it
Page 9 of 11
A. I felt more confident in completing the prep
B. I felt more motivated to show up
C. I could cancel/reschedule more readily
D. It did not change my value of the procedure
Page 10 of 11
[Free Text]
Page 11 of 11
A: 5-min phone call
B: In-person interview
C: I don't want to be contacted