
Abstract
Background/Introduction:
In 2015, five high-quality trials demonstrated the effectiveness of endovascular thrombectomy for certain patients. Patient selection for transfer to a hub hospital is mostly focused on the patient's eligibility for a potential thrombectomy. However, it remains challenging to correctly select those patients with the highest probability of undergoing a thrombectomy.
Materials and Methods:
In this study, we investigated which factors promote or impede the transfer of patients and whether the impact of these factors has changed since the publication of the five randomized thrombectomy studies in 2015. We analyzed 12,048 cases of telestroke consultation from the stroke telemedicine network in Thuringia (SATELIT) and compared the decision-making process related to patient transfer based on consultations that occurred before and after 2015.
Results:
In both time intervals, we found that the patient's age and the identification of a proximal vessel occlusion independently influenced the decision to transfer a patient. The age factor remained unchanged over time. A known proximal intracranial vessel occlusion had a strong positive influence on the decision to transfer patients.
Discussion:
The decision of whether to transfer a patient is currently focused on the identification of intracranial vessel occlusion. However, the age of the patient remains an unchanged but important factor that might be overemphasized. The time elapsed from symptom onset to consultation was not found to have an independent influence on the decision-making process, so it might be underemphasized.
Conclusions:
The decision-making process to transfer a patient within our telestroke network has been strongly affected by the publication of the endovascular thrombectomy studies, but those studies are not solely optimized for this aim.
Introduction
The service of a telestroke network provides neurological expertise to hospitals in remote locations that have limited access to direct neurological care. The two most important questions in every telestroke consultation are whether to treat the patient with tissue plasminogen activator (tPA) and whether there are reasons that the patient should be transferred to the hub hospital. In general, a patient is transferred when the planned treatment is not available in the rural hospital.
In this regard, the acute endovascular thrombectomy is of primary importance. 1 In 2015, five high-quality trials demonstrated the effectiveness of endovascular thrombectomy in addition to the use of tPA for specific patients.
Currently, there are multiple studies available that demonstrate that endovascular thrombectomy is of benefit to most patients with ischemic stroke due to a proximal intracranial vessel occlusion. 2 The results of these studies were published in 2015. These studies have strongly influenced clinical decision-making and have implications on the structuring of care systems that provide this treatment option. 3 –7
However, it remains unclear how we can apply the benefits of the endovascular thrombectomy to patients in a telestroke network. Theoretically, patients with intracranial vessel occlusion should be transferred for an endovascular thrombectomy at a hub hospital so that there is a short time delay between symptom onset and their arrival at the hub hospital.
However, diagnosing an intracranial vessel occlusion requires angiographic information, which is often not available in many rural hospitals due to the poor availability of computed tomography (CT) or magnetic resonance imaging (MRI) angiography. 1 Furthermore, it is not completely known in which time window an endovascular thrombectomy is beneficial. 2 A meta-analysis of the initial randomized trials suggests that the benefits of an endovascular thrombectomy become nonsignificant after ∼7 h. 8 However, it was also shown that patients benefited in a time window of up to 24 h from endovascular thrombectomy if the patients were selected based on perfusion imaging. 9,10 There are also studies available indicating that the individual predictability of clinical benefits from endovascular thrombectomy is based on perfusion imaging. 9,11 However, this method is currently not available in most rural hospitals.
It remains an important and regularly encountered question in practical telestroke medicine: how are patients selected who have the highest probability to undergo endovascular thrombectomy and who also might benefit the most from this intervention. This selection is particularly difficult as the potential individual benefits for patients are determined by multiple factors (e.g., age, availability of angiographic information, thrombus position, time from symptom onset, travel time, and severity of symptoms). 1
We hypothesized that the knowledge about the benefits of endovascular thrombectomy has changed decision-making in our telestroke network. To test this hypothesis, we analyzed 12,048 written telemedicine consultations. We were further interested in analyzing which factors promote and which factors impede the decision to transfer a patient and whether those factors have changed over time.
Materials and Methods
Network Description
The stroke telemedicine network in Thuringia (SATELIT) was founded in April 2012 and consists of 2 hubs and 19 spoke facilities in the plane country of Thuringia (2.2 million inhabitants). Both hubs are designated as tertiary stroke centers. The spoke facilities entered the SATELIT network at different times (Fig. 1).
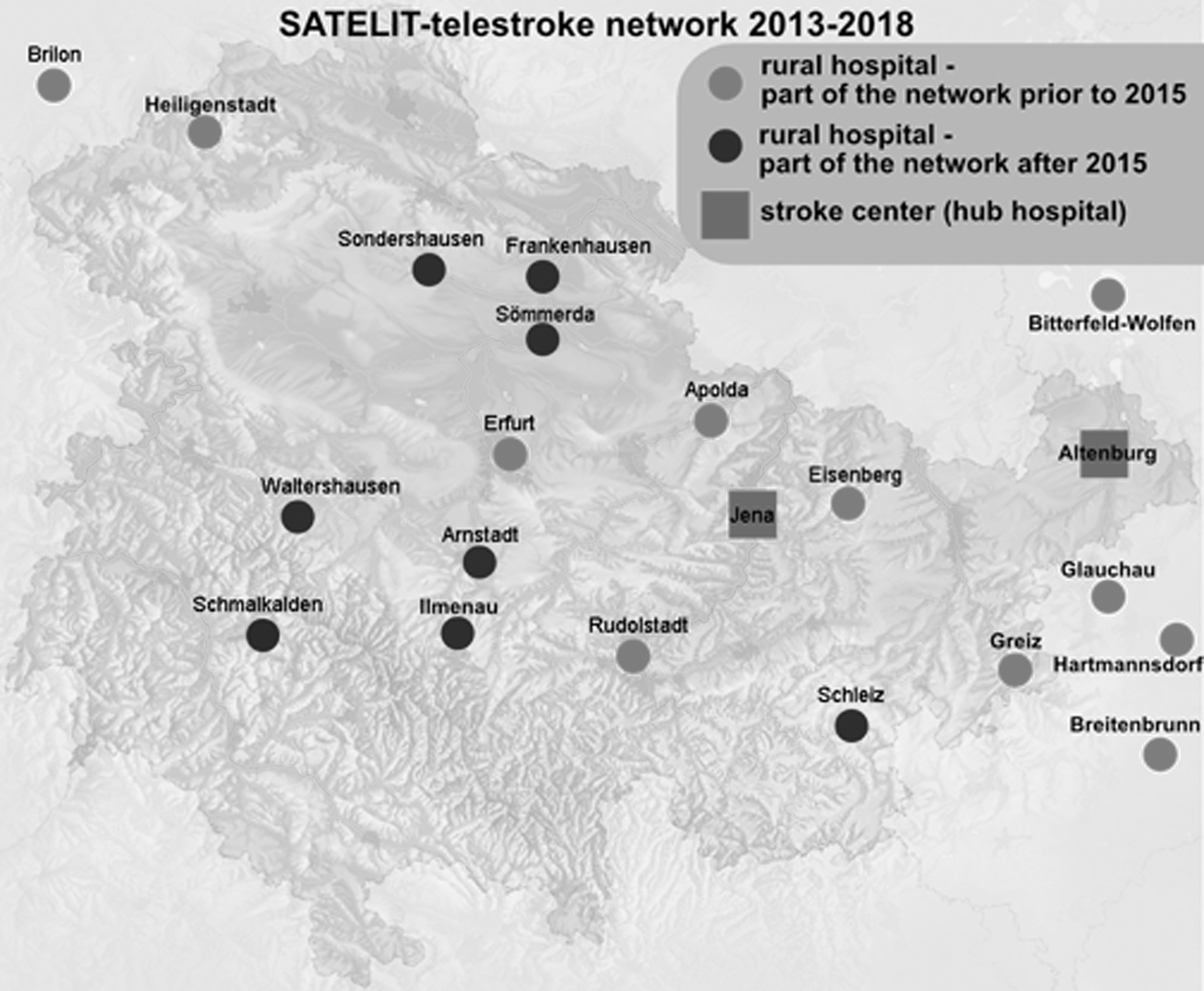
Schematic outline of the SATELIT telestroke network. The two hub facilities are illustrated as rectangles. The spoke facilities are shown as circles (grey if they entered the SATELIT network before 2015 or black if they entered after 2015). SATELIT, stroke telemedicine network in Thuringia.
Study Population
Data for this study were collected from the SATELIT telestroke network registry. We included all written telemedicine consultations that occurred between January 2013 and December 2017. In this time frame, 12,048 consultations were performed. All of these written telemedicine consultations are included in the current analysis.
Technical Implementation of the Telestroke Network
The telestroke network uses the technical implementation of one vendor (MeyTec GmbH Medizinsysteme, Werneuchen, Germany). The telestroke equipment includes a high-definition camera, audio, and a visual display that allows the stroke expert to perform a virtual full-clinical assessment. In addition, the available brain imaging can be reviewed. Data transfer is realized by a secure high-speed internet connection.
Procedure for a Telestroke Consultation
Every rural hospital that is part of the telestroke network (spoke hospital) can have a telemedicine consultation with a stroke expert at any time (24/7). These consultations are primarily designed for the acute treatment of stroke patients. A telemedicine consultation can be initiated by delivering written information about the patient (name, age, current symptoms, relevant medical history, and current medication). The consulting stroke expert will be informed and will review the request along with the available brain imaging of the patient. Patient questioning and examination are performed by the stroke expert using a two-way interactive video conference. In every telestroke examination, the National Institutes of Health Stroke Scale (NIHSS) is used to quantify the clinical severity of symptoms. After patient examination and review of the available brain imaging, the stroke expert and the rural physician discuss the case by phone, and a written consultation is delivered.
Data Management and Statistical Analysis
All data that were recorded during telestroke consultations between January 2013 and December 2017 were included in the current analysis. These data were transferred from an SQL® database to MATLAB® (MathWorks) and SPSS®25.0 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.) for further analysis. To investigate the decision-making process for transfer and further intervention for patients, we extracted the following information from the written teleconsultations: Patient age NIHSS Time between symptom onset and telestroke consultation Imaging modality (CT or MRI) Availability of angiographic information Vessel occlusion Was thrombolysis with tPA suggested and performed? Was the patient transferred to the hub hospital? Was an emergent endovascular intracranial thrombectomy performed after transfer?
Statistical tests were performed using Student's t tests, contingency analysis, and logistic regression analysis. Owing to the potential correlation of factors, we performed an additional logistic regression analysis to identify factors that independently influenced the decision-making process.
Results
During the first survey (January 2013–May 2015), 4,564 written teleconsultations were performed for 11 rural hospitals in Thuringia (Fig. 1). We excluded all patients with nonstroke diagnoses from further analysis (798, 17.5%). The remaining 3,766 patients (mean age 74.7 ± 12.7 years) constituted study group 1 (consultations before May 2015). During the second part of the survey (May 2015–January 2018), 7,484 written teleconsultations were performed for 19 rural hospitals in Thuringia (Fig. 1). Again, we excluded all patients with nonstroke diagnoses from further analysis (1,313, 17.5%). The remaining 6,171 patients (mean age 74.2 ± 13.0 years) constituted study group 2 (consultations after May 2015, see Table 1 ).
Differences in the Characteristics of Stroke Patients of the Two Investigated Time Windows
Group differences were tested for statistical significance using a single logistic regression analysis.
CT, computed tomography; MR, magnetic resonance; MRI, magnetic resonance imaging; NIHSS, National Institutes of Health Stroke Scale.
In group 1 (January 2013–May 2015), at the time of consultation (before potential thrombolysis), the mean NIHSS was 5.1 ± 6.3. Of the 3,766 stroke patients, 331 patients (8.8%) were thrombolyzed with tPA. Of these 331 thrombolyzed patients, a transfer to the hub hospital was suggested for 43 cases (13.0%). Of all the 3,766 stroke patients, 164 (4.35%) were transferred to a stroke center. The time between symptom onset and telestroke consultation was known in 1,081 cases, with a mean of 182.5 ± 108.5 min. Imaging was performed by CT in 85.5% (3,220) of patients, and MRI data were collected in 14.5% (546) of patients. Angiographic information (CT or magnetic resonance [MR] angiography) was available for 572 patients (15.2%). In cases for which angiographic information was available, occlusion of an intracranial vessel was found in 68 patients (11.9%, overall 1.8%).
In group 2 (May 2015–January 2018), at the time of consultation (before potential thrombolysis), the mean NIHSS was 4.7 ± 6.1. Of the 6,171 stroke patients, 654 patients (10.6%) were thrombolyzed with tPA. Of these 654 thrombolyzed patients, a transfer to the hub hospital was suggested for 89 cases (13.6%). Of the 6,171 stroke patients, 241 (3.9%) were transferred to a stroke center. The time between symptom onset and telestroke consultation was known in 2,339 cases, with a mean of 206.9 ± 138.5 min. Imaging was performed by CT in 87.1% (5,375) of patients, and MRI data were collected in 12.9% (796) of patients. Angiographic information (CT or MR angiography) was available for 1,216 patients (19.7%). In cases for which angiographic information was available, occlusion of an intracranial vessel was found in 290 patients (23.9%, overall 4.7%).
We compared these parameters between both groups by using logistic regression analysis. We found significant differences between groups for all parameters except thrombolysis and age. In group 2, there was more angiographic information available, and there were more diagnosed proximal intracranial vessel occlusions, whereas the general probability of patient transfer decreased.
According to the primary hypothesis of this study, we analyzed which factors influenced the decision to transfer the patients using logistic regression analysis to account for the possible correlations of factors.
We found a significant influence on the probability to transfer patients for the following parameters in both groups: performed thrombolysis (p < 0.01), age (p < 0.001), and proximal intracranial vessel occlusion (p < 0.000001). We tested for a difference between these parameters between groups. The influence of age on the probability to transfer patients did not significantly change. However, we found a significant increase in group 2 compared with group 1 concerning the influence of both the availability of angiographic information and the knowledge of a proximal intracranial vessel occlusion (Table 2). The availability of angiographic information was a significant factor influencing the transfer of patients in group 2, but not in group 1. The finding of a proximal intracranial vessel occlusion was significantly higher in transferred patients of group 2 than transferred patients of group 1 (50.4% vs. 18.1%, p = 0.004). Table 2 shows the important parameters of both groups in relation to whether the patients were transferred to the hub hospital or stayed at the spoke hospital.
Differences in the Characteristics of Patients Who Were Transferred Until 2015 Compared with Patients Who Were Transferred After 06/2015
Group differences were tested for statistical significance using a single logistic regression analysis.
CT, computed tomography; MR, magnetic resonance; MRI, magnetic resonance imaging.
We further analyzed whether the effectiveness of patient transfer changed between groups, that is, whether the proportion of transferred patients who received a thrombectomy changed. However, for this analysis, we only had access to data from our hospital, and not all patients were transferred to our hospital.
In group 1, 105 patients were transferred to our hub hospital, and 8 (7.6%) of them received an acute endovascular thrombectomy. As a subgroup of these 105 patients, we analyzed all patients with a known proximal intracranial vessel occlusion (n = 26, 13 basilar artery occlusions, 13 middle cerebral artery occlusion). Of the 26 patients transferred with a known intracranial vessel occlusion, an endovascular thrombectomy was performed in 7 patients (5 basilar artery occlusion, 2 middle cerebral artery occlusion). In the other patients, no endovascular thrombectomy was performed for the following reasons: vessel recanalization during transport in 11 patients; the combination of minor mismatch, duration of symptoms, and severity of clinical symptoms in 7 patients; and an additional internal carotid artery (ICA) occlusion in 1 patient.
In group 2, 107 patients were transferred to our hub hospital, and 22 (20.6%) of them received an acute endovascular thrombectomy. As a subgroup of these 107 patients, we again analyzed all patients with a known proximal intracranial vessel occlusion (n = 40, 10 basilar artery occlusions, 30 middle cerebral artery occlusion). Of the 40 patients transferred who had a known intracranial vessel occlusion, an endovascular thrombectomy was performed in 22 of them (4 basilar artery occlusion, 18 middle cerebral artery occlusion). In the other patients, no endovascular thrombectomy was performed for the following reasons: vessel recanalization during transport in nine patients; the combination of minor mismatch, duration of symptoms, and severity of clinical symptoms in seven patients; and an additional ACI occlusion in two patients.
Although there is a strong negative correlation between patient age and the probability of transfer, for those patients who were transferred, we did not find a correlation between the patient's age and the probability that an endovascular thrombectomy was performed.
Discussion
In this study, we investigated changes in the decision-making process of transferring patients within a telestroke network. We compared telestroke consultations before and after the publication of major thrombectomy studies in 2015. We found that the main factor that changed in the decision-making process was the knowledge about a proximal intracranial vessel occlusion. This factor showed a strong increase in its influence on the decision-making process for consultations after the publication of the thrombectomy studies in 2015 and had become the major influencing factor for patient transfer within our telestroke network. This strong influence is quite understandable, as a proximal intracranial vessel occlusion is the prerequisite for the performance of an endovascular thrombectomy.
A further factor that significantly influenced the decision-making process for shipment is the age of the patient. We found a strong negative correlation between the age of patients and the probability of transfer in both groups without significant changes over time. After arrival at the hub hospital, the probability that a patient would undergo an endovascular thrombectomy was not correlated with patient age. This suggests that the age of patients was overemphasized in the decision-making process in both groups, particularly as a positive treatment effect of endovascular thrombectomy has also been shown for elderly patients (>80 years). 3 It is possible that the age dependence of the decision-making process is affected by the aforementioned studies, demonstrating an inverse correlation between a good functional outcome after an endovascular thrombectomy and the age of the patient. 12,13
Another important factor in the decision-making process is the time window between symptom onset and consultation. Data from the randomized trials of endovascular thrombectomy 3,4,5 –7 suggest that not only the finding of a proximal intracranial vessel occlusion but also the combination of this finding with a short time window between symptom onset and intervention is important for patient outcomes and should have affected the decision-making process. However, although the time from symptom onset to consultation changed from 176 min (before 2015) to 153 min (after 2015), this decrease was not a statistically significant factor of influence in the decision-making process. As a possible explanation for the small impact of the time window on the decision-making process, we suggest the option to perform endovascular thrombectomy beyond the classical time windows based on perfusion imaging to promote the shipment of patients with prolonged time windows. 10
It is, for example, tempting to transfer a severely impaired young patient without angiographic information and a contraindication for the use of tPA (for example, because of the prolonged time window) when the endovascular thrombectomy is the only remaining therapeutic option for reperfusion, even if the probability that the patient is eligible is low. Decisions that are based on this way of thinking explain both the strong negative correlation between the probability to be transferred and patient age and the lack of correlation between the probability to be transferred and the time window of symptom onset until consultation.
The pattern of the strong importance of a proximal intracranial vessel occlusion together with the importance of young age and the lack of importance of clinical severity and time window of patients suggests a specific aim in the decision-making process. The decision-making process does not seem to be optimized to select those patients with the highest probability of undergoing a thrombectomy (patients with a proximal intracranial vessel occlusion, short time window, and severe clinical symptoms, independent of age), and it is not optimized to select those patients who are difficult to treat (the oldest and most severely affected). Instead, the decision-making process seems to be aimed at the selection of patients who would avoid a long-lasting impairment by endovascular thrombectomy. Or to put it in other words, the aim is to save the most lifetime and life quality.
In conclusion, this study demonstrates that after the publication of the thrombectomy studies, decisions to transfer patients are more strongly influenced by the presence or absence of proximal intracranial vessel occlusion. If we consider the performance of an endovascular thrombectomy as a target, then the decision-making process has become more efficient. However, the decision-making process is not optimized as symptom severity and elapsed time since symptom onset seems to be underestimated, whereas the age of patients remains an important factor that is overemphasized.
Footnotes
Acknowledgments
The authors received research grants from Bundesministerium für Bildung und Forschung BMBF (JenAge, 0315581), BMBF (Irestra, 16SV7209), Deutsche Forschungsgemeinschaft DFG (HHDP, FO 1738, WI 830/10-2, and WI 830/11-1/OrganAge and RTG1715), Else Kröner Foundation (AntiAge and Jena School for Ageing Research), and TMWWDG (ProExellenz, RegenerAging-FSU-I-03/14).
Disclosure Statement
No competing financial interests exist.