
Abstract
This article reviews a systematic approach to implementation of telemedicine services in a large integrated multispecialty health care system. Eight components of operational infrastructure have been identified as essential to effective program deployment and sustainability. These components include (1) dedicated telemedicine staffing infrastructure, (2) functional support partnerships, (3) standardized systems of deployment, (4) refined operational processes and procedures, (5) data analytics, (6) practice partnerships, (7) performance reporting, and (8) provider instruction. Mayo Clinic Center for Connected Care endeavors to share its practice and its learning.
Introduction
According to data collected in 2017, nearly half (47%) of health care organizations surveyed reported still being stuck in various early phases of telemedicine adoption, including contemplating, developing, piloting, and implementing. 1 The majority (59%) of those health care organizations in an implementation phase reported difficulties in implementing telemedicine practices. 1 From the same survey sources, over a third (39%) of U.S. health care providers stated that barriers to effective implementation of telemedicine remained unaddressed. Despite the advantages offered by telemedicine such as access to care, improved quality and satisfaction, and reduced cost, health systems face multiple impediments to effective implementation. The principle challenges include administrative engagement, provider engagement, infrastructure, and ultimately sustainability. Herein, we report the systematic approach developed to effectively and efficiently deliver telemedicine in a large multicenter multistate health care system.
Operational Components
Telemedicine program deployment roadmaps are well documented. 2,3 Less demonstrated is the practical application of these guidelines in a large multispecialty health care organization. In 2014, the Mayo Clinic created its Center for Connected Care and tasked it with overseeing the deployment of its telemedicine program and related services throughout the Mayo Clinic enterprise.
Operational infrastructure is required to manufacture a robust, versatile, and sustainable model that can be used as the basis for developing telemedicine in nearly any location and for nearly any specialty. Critical to success is executing on a systematic approach built upon an underlying foundation of personnel, partnerships, processes, metrics, and education reinforcing efficient and scalable systems of implementation and operational support. We have identified eight essential operational components that when incorporated, provide the greatest opportunity for success (Fig. 1).
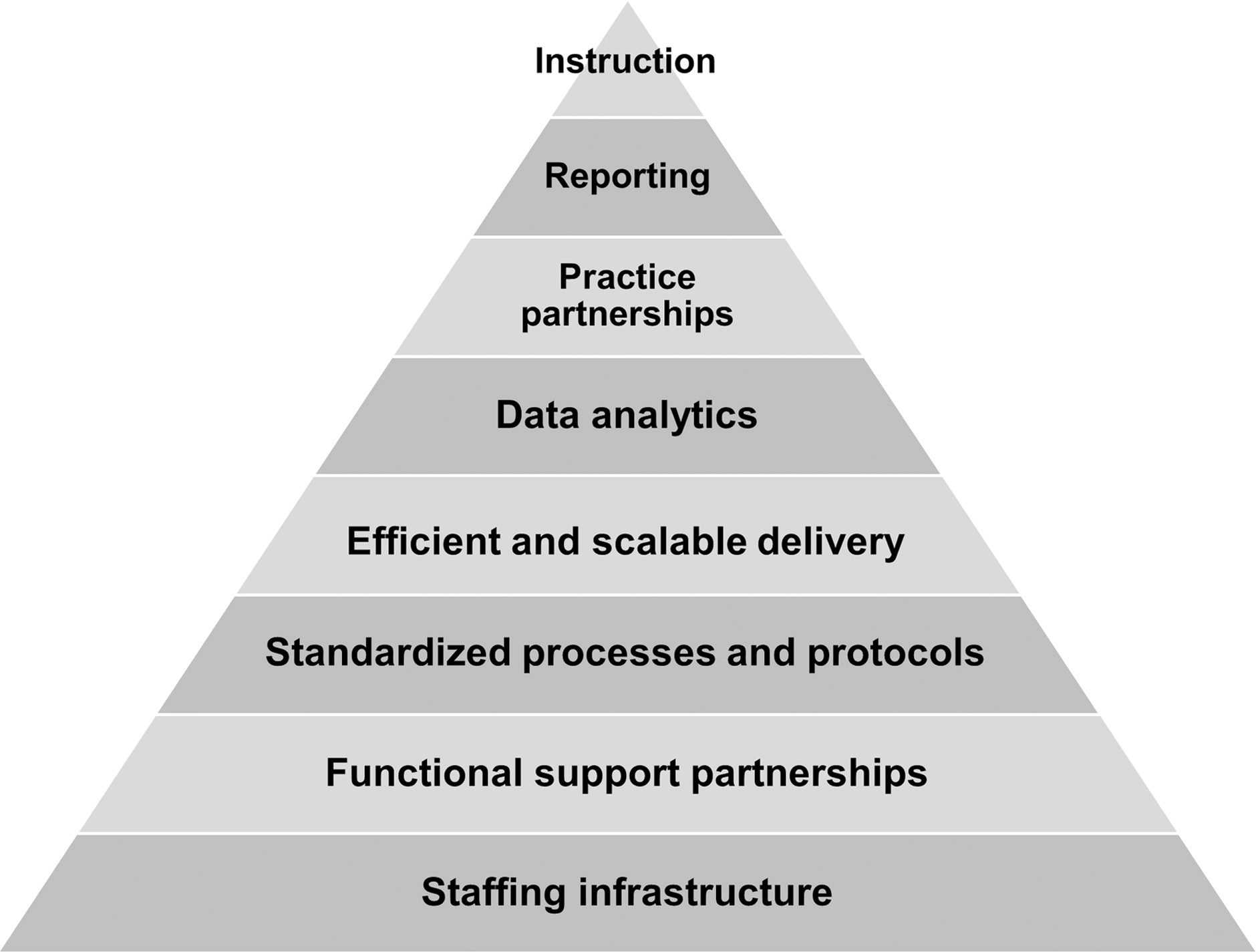
Essential elements of operational infrastructure.
Eight components of a robust telemedicine program: Staffing infrastructure suitable to support a telemedicine program. Functional partnerships critical to create and sustain a telemedicine program. Standardized processes and protocols to enable delivery of telemedicine services. Refined systems of implementation for efficient and scalable deployment of telemedicine services. Data analytics to understand and establish the optimal mix of in-person and telemedicine care. Practice partnerships to facilitate adoption and embed telemedicine as a core care platform. Reporting systems to monitor adoption, build buy-in, and demonstrate patient and institutional value. Curricula to incorporate telemedicine into the instruction of provider education.
Staffing Infrastructure
Identification and integration of key staff are essential to the establishment, implementation, and on-going support of a telemedicine program. Telemedicine, although a new modality in the delivery of health care, comprises many of the same complex clinical workflows associated with in-person patient care. Some of these operational workflows include scheduling, billing, licensing, credentialing, and user and technology support, to name a few. Each of these operational functions can require extensive subject matter expertise and dedicated support personnel. In addition, a successful program requires staffing infrastructure for the implementation of telemedicine services into the clinical practice. Resource requirements are focused on the coordination and facilitation of personnel and tasks. Aligning the proper resource to the appropriate role is important, as the prerequisite staff attributes and experiences will vary significantly between functional activities. The need for implementation and operational support can result in a staffing gap.
Although operational expertise is usually established within the traditional in-person practice, there is most likely a lack of critical resourcing of implementation personnel. This requires organizations to commit to the establishment of a core team or department with dedicated expertise in telemedicine project management, process analysis, workflow design, content creation and management, training, and change management. Roles within the implementation team include staff to coordinate and facilitate service deployment, personnel to oversee and manage product procurement and installation, and implementation and on-going support personnel to provide education and customer service. Implementation teams need to partner closely with established functional groups to design and standardize the processes and protocols required to deliver telemedicine services. Defining the core competencies and responsibilities of functional support partners and the telemedicine implementation team will help to ensure clear roles and expectations in implementation and ongoing support. The Center for Connected Care at Mayo Clinic has identified five core competencies critical for telemedicine programs (Fig. 2).
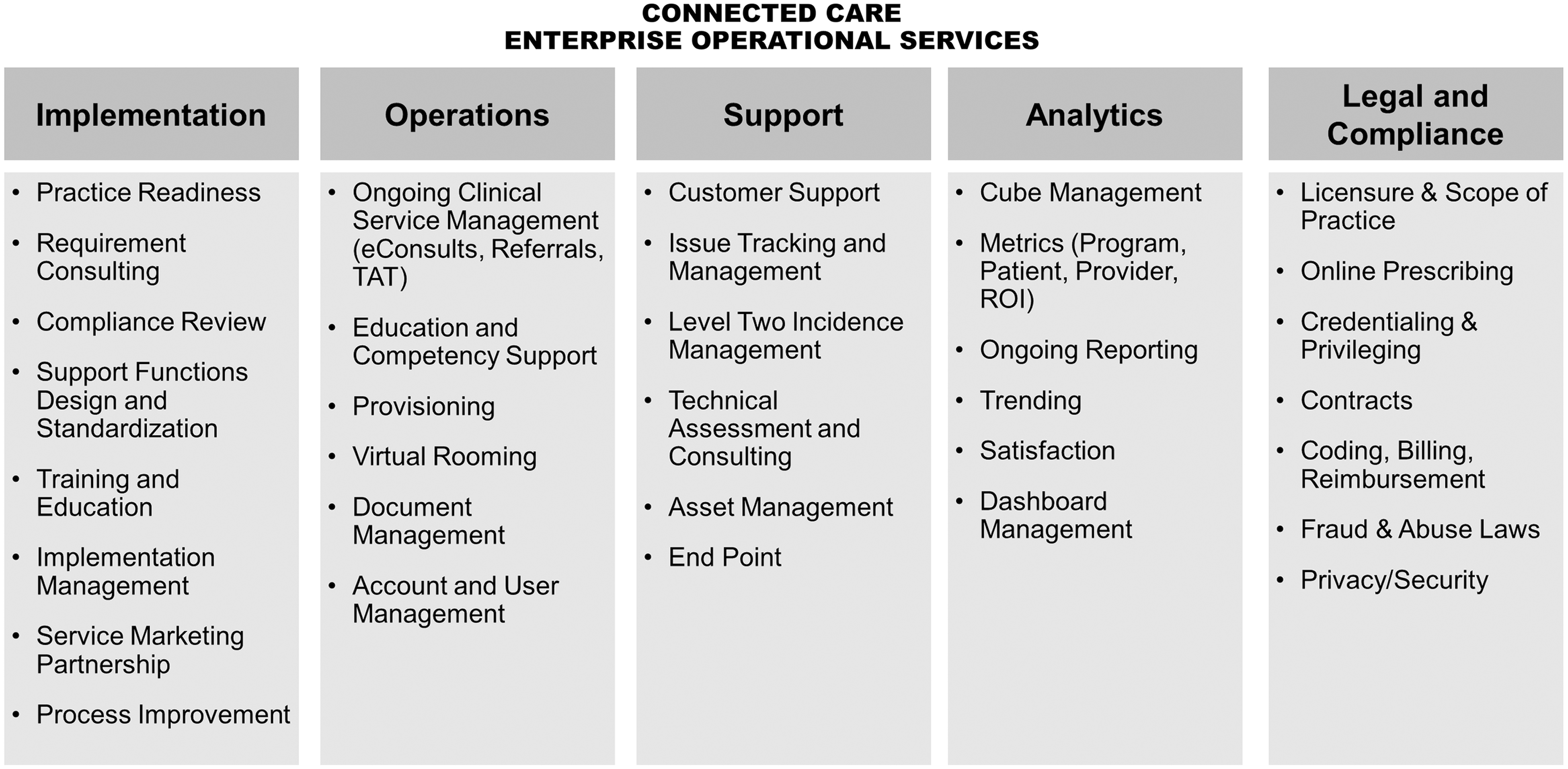
Center for Connected Care core competencies.
These five core competencies include:
Implementation services to evaluate new program requests (value, complexity, and readiness), facilitate and manage the implementation process, and provide training and reference materials.
Operations to support ongoing telemedicine programs including education, content management, provisioning, and placing patients in virtual waiting rooms.
User support that aligns with program needs along with issue management and tracking, and asset management support.
Analytics to assess program utilization, optimal care mix, value, patient and provider satisfaction, and return on investment.
Legal and compliance support to ensure the most up-to-date legal and regulatory telemedicine considerations and needs are implemented.
Functional Support Partnerships
Building integrated partnerships and embedding telemedicine expertise within information technology, scheduling, revenue, legal, compliance, licensing and credentialing, public affairs, government relations, and other core functional areas are vital to the successful deployment of telemedicine services. Without these strong committed partnerships, a small group of telemedicine resources is required to become experts in core functional areas that support clinical delivery.
Rather than replicating these core competencies within the Center for Connected Care, Mayo Clinic took the approach of requiring supporting areas to designate resources within their departments that could build and maintain telemedicine expertise within this rapidly evolving space. Once designated resources were identified, initial assignments involved understanding the telemedicine domain through the lens of their functional domain and how it differed from or was the same than the in-person practice.
In collaborating with the Center for Connected Care, these partners help establish standard operating procedures to support telemedicine use case assessments and implementations. One noted example of the outcome of such a partnership is the collaboration with revenue cycle, legal, and compliance who develop workflows and institutional procedures for validating telemedicine reimbursement and ensuring proper documentation for billing telemedicine services. This effort led to a 40% increase in billing accuracy for telemedicine use cases for a 2-year period.
Standardized Processes and Protocols
Operational systems including processes, procedures, and tools are needed to effectively implement and provide ongoing operational support for telemedicine services. These systems must incorporate standards that reduce variation in implementation methodology and execution between teams and among personnel.
Diffusion toolkits that mimic similar processes and incorporate standard tools for implementation provide implementation teams and functional support partners with a clear and repeatable roadmap. A standard process supporting implementation and adoption ensures that practice areas experience a predictable and consistent approach when faced with integrating telemedicine into their practice. This consistency can foster change management as practice areas learn to trust and rely on their partnership with the implementation team to guide them through a comprehensive process that will prepare them for success to deliver telemedicine. Continuous iterations of these toolkits are imperative to account for lessons learned through previous implementation experiences.
The Center for Connected Care employs a five-phased process for supporting the implementation of telemedicine (Fig. 3). All requests for service begin with a discovery review to understand the needs of the practice partner in an effort to validate fit with the Center for Connected Care services. This process includes a service assessment that examines the scope of service, technical and operational complexity, practice readiness, service value, and legal and compliance implications. Once validated, the service enters a design phase in which clinical and operational workflows are reviewed and adapted to the specific clinical and operational needs of the practice partner. After design, the project enters deployment. During this phase, providers and care teams are trained to the telemedicine workflows and provide reference material to support provider and patient education. Finally, the service is live and enters adoption and optimization as additional providers are on-boarded and operational processes are monitored and refined.

Phases of telemedicine implementation.
Efficient and Scalable Delivery
Once established, the systems of implementation must be optimized to allow for rapid and scalable adoption by the clinical practice. Legacy systems designed to support the traditional in-person practice need to be refined and in some cases redesigned to expedite program integration into the organization. Technology needs to be proactively deployed so that providers are equipped when ready to start offering telemedicine services. Less complex clinical use cases should follow an expedited implementation process flow, allowing for rapid service assessments and compliance reviews. Training procedures should incorporate videos and e-learning so that providers and care teams can perform self-directed onboarding. Best practices and quick reference guides should be made easily available to all practice areas to drive adoption of services. Patient informational materials, such as brochures and videos, should be provided to inform and educate on the ease and benefits of telemedicine. Although not appropriate for all clinic use cases and circumstances, removing barriers to adoption for both the provider and patient is the key to acceptance and rapid incorporation of telemedicine as a standard of care.
Data Analytics
Data can be a powerful tool to gauge opportunities to implement telemedicine strategies and assess the adoption of telemedicine services within a practice area. Converting all care to telemedicine is not appropriate, but understanding the optimal mix of in-person and telemedicine services is essential. To do so, we encourage implementation teams to assess opportunities within practice areas by utilizing the data available to the institution (e.g., admission rates by diagnosis and appointment utilization metrics). An example of this concept is the identification of high readmission rates for a specific patient population within a practice and then identifying telemedicine solutions that can assist in addressing the issue. Telemedicine options could include the implementation of a remote patient monitoring program or a video follow-up appointment option as potential solutions to combat the readmission problem. The goal is to leverage data analytics in a way to introduce the appropriate mix of telemedicine and in-person care, matched to the correct level of health care provider at the right time.
Conceptualizing how telemedicine can be integrated into a practice in this way can be overwhelming. Gathering data and proposing telemedicine solutions that meet the needs of the practice is a way to mitigate practice partners feeling the pressure of having to do so on their own. This approach can ensure the implementation of the most clinically appropriate type of telemedicine solution for the correct patient population that aims to increase efficiencies, cost savings, and resolve the opportunity initially identified through the data.
Practice Partnerships
Building strong partnerships with clinical practice areas can help an organization move from a reactive to a proactive mode of implementation and operations. The Center for Connected Care developed formalized practice partnerships to help align the adoption and implementation of telemedicine services with institutional priorities. Figure 4 shows the process deployed for formal practice engagement.
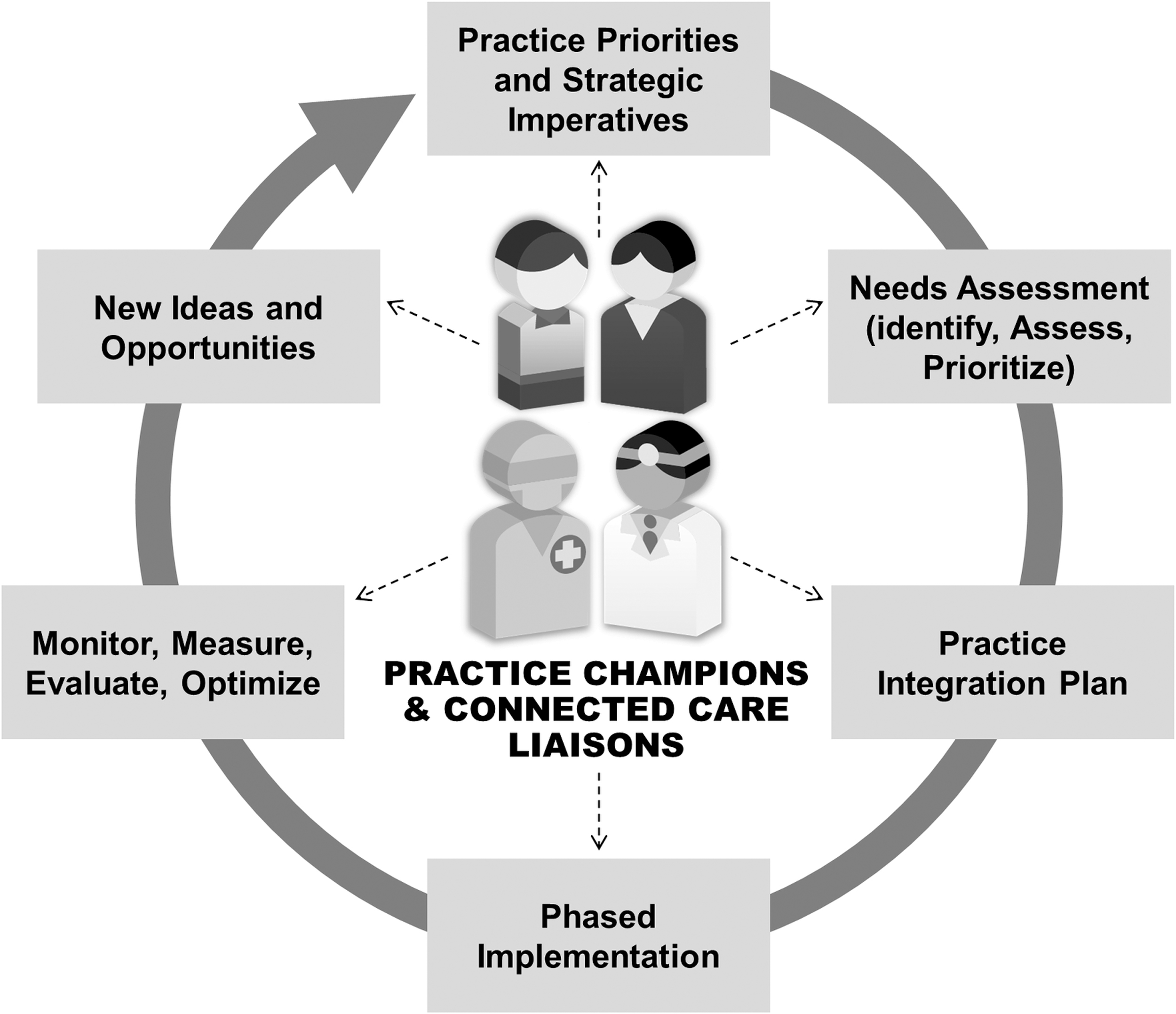
Practice partnership engagement cycle.
The first step in developing a formal partnership is to work with each practice area's leadership to identify key points of contact that can act as telemedicine practice champions and represent their practice area's needs and priorities across all locations. These practice champions should include a mix of physicians, nurses, and administration. Practice champions are partnered with leadership liaisons within the Center for Connected Care who work collaboratively to identify unmet needs and opportunities that can be addressed by telemedicine solutions.
The needs assessment includes identifying existing practice pain points and strategic priorities. Expectation of this combined team is to identify, define, and prioritize opportunities to leverage telemedicine solutions within the practice, develop a working plan for implementation, and monitor outcomes. Monthly meetings are established to monitor, measure, and evaluate progress with formal written status updates provided by the implementation team and quarterly dashboards to track adoption. Any new ideas or opportunities for telemedicine use cases for that practice area are vetted and prioritized by this established group.
Although this text describes the operational approach taken by the Center for Connected Care, it is critical to note that practice partnerships must be built upon a solid foundation of positive relationships formed between telemedicine teams and their clinical and operational partners.
Reporting
Establishing systems for sharing information on program performance, provider and patient measures, and return on investment is important in creating awareness of the value of telemedicine. Initially, organizational leadership, providers, and care teams may be hesitant to invest or adopt telemedicine services. This resistance can be, in part, due to a lack of understanding of the benefit and value of an integrated program. Understanding and demonstrating clinical and program value can be a critical change driver.
Although some financial metrics, such as direct revenue from reimbursement and cost avoidance related to readmissions, can be quantifiably measured, other value-based metrics can be more difficult to understand. Furthermore, not all value directly benefits the health care organization. Patient metrics, such as increased patient access to specialty care and improved clinical outcomes through extended care coordination and management, are critically important if not directly financially beneficial.
Frequent communications on the financial and value-based advantages of telemedicine through practice partnerships and related forums will inform key stakeholders and help to drive investment and adoption. Likewise, metrics should be established to understand operational and technological performance of implemented telemedicine services. Provider and patient measures including satisfaction with telemedicine technologies and clinical workflows can inform on inadequate processes, technology, and training that could result in provider or patient dissatisfaction. Ongoing monitoring and reporting can identify system gaps and provide opportunities for rapid and even proactive interventions that if otherwise unknown could adversely affect the quality and acceptance of telemedicine services.
Instruction
Education for professional health care staff and health care trainees is paramount to the overall telemedicine adoption success in a health care organization. Mayo Clinic elected to develop an education group that is responsible to provide strategic leadership, governance, and direction for the development and maintenance of quality education programs within the Center for Connected Care.
The education group sets the overall direction for the development of education curricula and ensures the delivery of such activities is coordinated and managed appropriately, effectively, and efficiently. The charge of the education group is to review, approve, and monitor execution of education programs that support the essential components of practicing telemedicine, ensuring alignment with educational needs of providers, and supporting health care teams at Mayo Clinic. The group also ensures consistent style, appropriateness, and accuracy of content through standard tools and templates. The education group ensures alignment with accreditation requirements, when applicable, and helps to secure resources needed to support curriculum development.
The members review and endorse changes to the curricular portfolio, and significant changes in direction regarding teaching modalities. Education members conduct periodic course reviews and customer needs assessment to ensure curriculum meets learning objectives and overall continuous improvement of course offerings and develop future education strategies. In this manner, the education group has worked to develop and deliver comprehensive education programs to support the delivery of telemedicine by all Mayo Clinic providers. The education group endeavors to partner with medical schools to develop a telemedicine curriculum for students, beginning with the Mayo Clinic School of Medicine.
The telemedicine curriculum framework will provide students with an opportunity to gain a foundational understanding of the ways that technology can be used to deliver health care and health information by leveraging existing and newly developed modules in the areas of webside manner, legal and regulatory practice considerations, and all forms of telemedicine services (video, remote monitoring, mobile, and store-and-forward). The medical school curriculum will provide students with opportunities to observe and engage with Mayo Clinic physicians as they deliver health care using telemedicine products and services.
Discussion
The complexities of deploying a telemedicine program and resulting services are well known. 4,5 As the demand for these services intensify, health care organizations will be increasingly pressured to adopt telemedicine as a standard of care. Although well-defined frameworks for program deployment exist, there remains a shortage of analysis on the practical applications of these frameworks within large multispecialty health care organizations.
The Mayo Clinic Center for Connected Care has developed a systematic approach to the implementation and maintenance of its telemedicine program. We believe that this approach may be informative to other health care organizations. However, execution of the program at a larger health care institute such as Mayo Clinic presents several advantages and challenges. Mayo Clinic leadership is committed to the integration of telemedicine services and has continued to provide incremental resources to support the development and maintenance of the program. This offers an advantage that smaller organizations most likely lack.
In addition, the Mayo Clinic clinical support infrastructure is well developed, with functional groups supporting scheduling, revenue, licensing, and credentialing, to name a few. This provided advantages in already developed systems to support the in-person practice but required significant effort to design, and in some cases redesign, processes so that they properly supported telemedicine care. Augmenting these efforts was the willingness of our functional partners and their leadership to dedicate staffing resources to support and become subject matter experts in telemedicine services. This again highlights a benefit available to larger organizations with access to a greater amount of resources and subject matter expertise.
Along with successes, the Center for Connected Care has also faced many challenges. Efficient deployment of telemedicine technologies is one example and stemmed from the institution's IT protocols and processes designed to support traditional in-person care. These process and resource constraints resulted in prolonged install turn-around times and required the addition of several layers of administrative oversight. To circumvent this, the Center for Connected Care and its IT partner developed a plan for the proactive deployment of telemedicine technologies—including monitors, web cameras, speakers, and headphones—to the clinical practice. Although still in process, the team's goal is to have proactively equipped 80% of the clinical practice within 12 months of project initiation.
Conclusions
In this article, we reviewed a systematic approach to implementation of telemedicine services in a large integrated multispecialty health care system. In summary, we identified and described the eight most essential components of operational infrastructure for effective telemedicine program deployment and sustainability: (1) dedicated staffing infrastructure, (2) functional support partnerships, (3) standardized systems of deployment, (4) refined operational processes and procedures, (5) data analytics, (6) practice partnerships, (7) performance reporting, and (8) provider instruction. Mayo Clinic Center for Connected Care endeavors to share its telemedicine practice and its learning.
Funding Information
No funding was received for this article.
Footnotes
Disclosure Statement
No competing financial interests exist.