
Abstract
Introduction:
There are few studies showing results about telemedicine strategies in traumatology and orthopedics. We present a new tele-orthopedic strategy started in 2017 at the Reloncaví Health Service in Chile. Our objective was to evaluate its efficiency and impact on the orthopedic surgery specialty care waiting times of the inhabitants of the Calbuco area.
Methods:
We selected two general practitioners from the Calbuco Hospital who evaluated patients on the waiting list of the specialty. Synchronous connections were made between them and one orthopedic surgeon staff at the referral hospital. Connections were conducted every 2 weeks. Four to eight cases were analyzed in each session.
Results:
Two hundred ninety-three (n = 293) attentions were performed between June 2017 and July 2018. Highly rural patients constituted 30%. After the first evaluation by the physicians of the Calbuco Hospital, 69.6% (204/293) of the patients' consultations were resolved. The remaining 30.4% (89 patients) were presented to the specialist by telemedicine, from which 69.7% (62) required one or more follow-up connections through tele-orthopedic and 30.3% (27) were referred for on-site assessment by a subspecialist. The waiting times of the referrals decreased on average from 201 to 40 days.
Discussion:
This new strategy had a significant impact on the population of Calbuco, especially for the rural population. It has been possible to significantly reduce waiting list times and optimize travel times and expenditures. Only a small percentage of patients required on-site attention by a specialist after the videoconference, exhibiting the efficiency of this strategy.
Introduction
Telemedicine is a branch of telehealth defined as the exchange of medical information between two actors not located at the same space, through some channel of electronic communication, to improve the health status of a patient. 1 There are very few studies showing results of telemedicine strategies in traumatology and orthopedics worldwide. 2 –4 This article presents a new tele-orthopedic strategy started in 2017 between two hospitals of the Reloncaví Health Service network in Chile.
The Chilean territory is divided into 15 regions. The National Health Service gives health care attention through 29 different health services to its population. 5 Our public health system has three levels of care: primary, secondary, and tertiary. The primary level consists of rural posts and urban clinics or hospitals. It intends to give maximum coverage at low complexity. It does not contemplate medical specialists' attention. The secondary level consists of different reference centers that give medical attention through medical specialists in an outpatient management setting. Last, the tertiary level, which goal is to address high complexity cases, is made up of hospitals with different levels of complexity.
In our region (Los Lagos), the Reloncaví Health Service provides attention to an extensive and geographically challenging territory, which poses a major hindrance for patient access to the tertiary level of health care. In consequence, patients do not often have prompt access to health care attention by some medical specialists. Limited access from rural locations due to poor connectivity, long travel times, and elevated transportation costs contributes to this problem. Due to the above, plenty of medical appointments are currently lost, causing significant inefficiencies in our health system.
To address this situation in Chile, there is an important number of physicians working as general practitioners widespread around the country, through what is called the Destination and Training cycle. 6 Through this initiative, general practitioners are destined to rural areas for a period lasting from 3 to 6 years and, on completion of this period, they are granted residency positions. These physicians manage to grant adequate health care coverage to the population living in areas of greater rurality. Calbuco Hospital, where we started this initiative, forms part of the primary level of health care, 7 having only this type of physicians. It has an assigned population of 33,985 inhabitants, 8 including the urban and rural areas around the city and the 14 islands that form the Calbuco Archipelago. Starting a few years back, this hospital has had variable access (on-site and by telemedicine) to certain specialty care units such as adult psychiatry, pediatrics, internal medicine, child neurology, and gynecology. However, as mentioned above, there was no easy access to care by specialists in traumatology and orthopedics until the starting date of this tele-orthopedic strategy. Orthopedic surgeons from the Reloncaví Health Service only work at the Puerto Montt Regional Hospital, the main tertiary health care level hospital in our health service. Therefore, this was a great need, as reflected in the elevated number of patients in the waiting list.
To improve the resolving capacity and the suitability of the referrals, we developed a novel tele-orthopedic strategy at the Calbuco Hospital, connecting local physicians with orthopedic surgeons from the Puerto Montt Regional Hospital. Telemedicine has well-known advantages for patients not only in terms of faster diagnoses and treatments, reduced displacements, and out-of-pocket expenses related to medical attention 9 but also keeping high-quality attention standards as perceived by patients 10 and reduced health system expenses. 11 Besides, telemedicine generates a better knowledge transfer and adds experience in the management of some health conditions to the primary care medical team.
Our objective was to evaluate the results of implementing this strategy in terms of the average waiting times of the inhabitants of the Calbuco area before medical attention and the effectiveness of the consultations achieved by this channel. Also, we sought to evaluate the behavior of the referrals from the primary care physicians under the premise that, after implementation of the strategy, there would be an improvement of the case-related knowledge transfer for the general practitioners who took part in this initiative.
The relevance of this study is that, given positive results, this model may be replicated in areas where geographic conditions, connectivity issues, or lack of specialists result in limited access to health care. This is, to our knowledge, the first synchronic telemedicine strategy in traumatology and orthopedics in Latin America to date.
Materials and Methods
Before the implementation of the new tele-orthopedic program, we prepared a protocol to clarify the types of pathology and expected outcomes for this initiative. We prepared a protocol specifying the necessary radiological projections to be obtained by the Calbuco Hospital radiology technologist. In addition, the technical reliability of the connections and image access between both hospitals involved in the study was verified. The protocol was signed by the authorities of Puerto Montt Regional Hospital and Calbuco Hospital, as well as the Reloncaví Health Service. On-site training and inspection visits were carried out with the radiology technologist at the Calbuco Hospital.
We selected two general practitioners interested in the area of traumatology and orthopedics. These physicians were tasked with evaluating patients from the waiting list of the specialty. After initial evaluation, these physicians either resolved the cases in the primary care setting or scheduled them to be presented to the specialist on a videoconference.
X-rays were viewed using the online software SYNAPSE® TELERADIOLOGY in both institutions. Videoconferences were conducted using Polycom® CMA desktop software.
Synchronous (real-time)1 connections were made between a Calbuco Hospital physician and one of the Puerto Montt Regional Hospital orthopedic surgeon's staff (the senior author). Connections were scheduled every 2 weeks, each one lasting between 60 and 90 min. Usually, four to eight orthopedic referrals chosen from the waiting list were analyzed in each meeting. Cases were ordered from oldest to newest and categorized by severity as indicated in our waiting list system. Some additional cases were included: patients derived from the Calbuco Hospital emergency room (ER) and patients referred from the Puerto Montt Regional Hospital ER to the specialty polyclinic, who were part of the Calbuco Hospital assigned population.
Consultations were recorded simultaneously by the consultant specialist and the consulting physician using the digital clinical record systems of the Puerto Montt Regional Hospital and the Calbuco Hospital, respectively.
After evaluation, the referrals from the waiting list were withdrawn from the list if and when the cases were resolved. If the case was resolved after presentation of the case to the specialist, the assigned resolution cause was “telemedicine,” whereas cases resolved by the physicians at a previous consultation were either discharged from the list due to “not pertinent” cause or “change in clinical condition,” according to the physicians' criteria.
Calbuco Hospital physicians were required to e-mail a PowerPoint presentation summarizing the clinical case to the orthopedic surgeon, with at least 1 day in advance to the videoconference, following a previously prepared format specific to this purpose.
As stated previously, all the patients included in the tele-orthopedic program were evaluated initially by one of the two physicians (coauthors) from the Calbuco Hospital. After initial evaluation, relevant examinations were requested (mostly X-ray projections according to protocol and clinical suspicion). In some cases, treatments were indicated and follow-up appointments scheduled according to the attending physician's criteria. These patients were discharged without the need of follow-up by the specialist.
Patients were also stratified according to the distance from their residence to the Calbuco Hospital. (1) An urban zone was defined as a 2 km radius from the center of the Calbuco Island (communal capital and where the Calbuco Hospital is located); (2) low rurality zone was defined when the patient was located within a 2–4 km radius; and (3) high rurality zone when the distance was over 4 km. This classification was created owing that expedited and affordable public transportation is only available within the urban radius. Over this limit, it is neither continuous nor affordable.
The program started in June 2017 and is currently in effect.
Results
In this analysis, we considered 293 attentions performed throughout the first year of implementing this new strategy, in a period between June 2017 and July 2018.
Forty percent of the total number of consultations corresponded to patients from the traumatology and orthopedic referral waiting list of the Puerto Montt Regional Hospital. The remaining 60% of the cases were patient follow-up appointments/referrals either from Calbuco Hospital or Puerto Montt Regional Hospital ER. Thirty percent of total cases came from areas categorized as highly rural (Fig. 1).
Patients' home location distribution.
Before the strategy began, the Puerto Montt Regional Hospital waiting list comprised 102 patients. The number of patients by subspecialty was as follows: 68 knee, 22 foot and ankle, 6 hand and wrist, 2 shoulder and elbow, and 4 general orthopedics (Fig. 2). The average waiting time to consultation before the strategy started was of 201.4 days (95% confidence interval [CI] 144–258.8). The average waiting times by orthopedic subspecialty (Fig. 3) were 310.6 days (95% CI 164.6–456.6) for the knee team, 231.4 days (95% CI 127.6–335.1) for the shoulder and elbow team, 176.4 days (95% CI 88.8–264) for the hand and wrist team, 48 days (95% CI 20.1–75.9) for the foot and ankle team, and 120 days (95% CI 21.2–218.9) for general orthopedic referrals (includes orthopedic oncology and others at our center).

Number of patients on the waiting list by subspecialty.
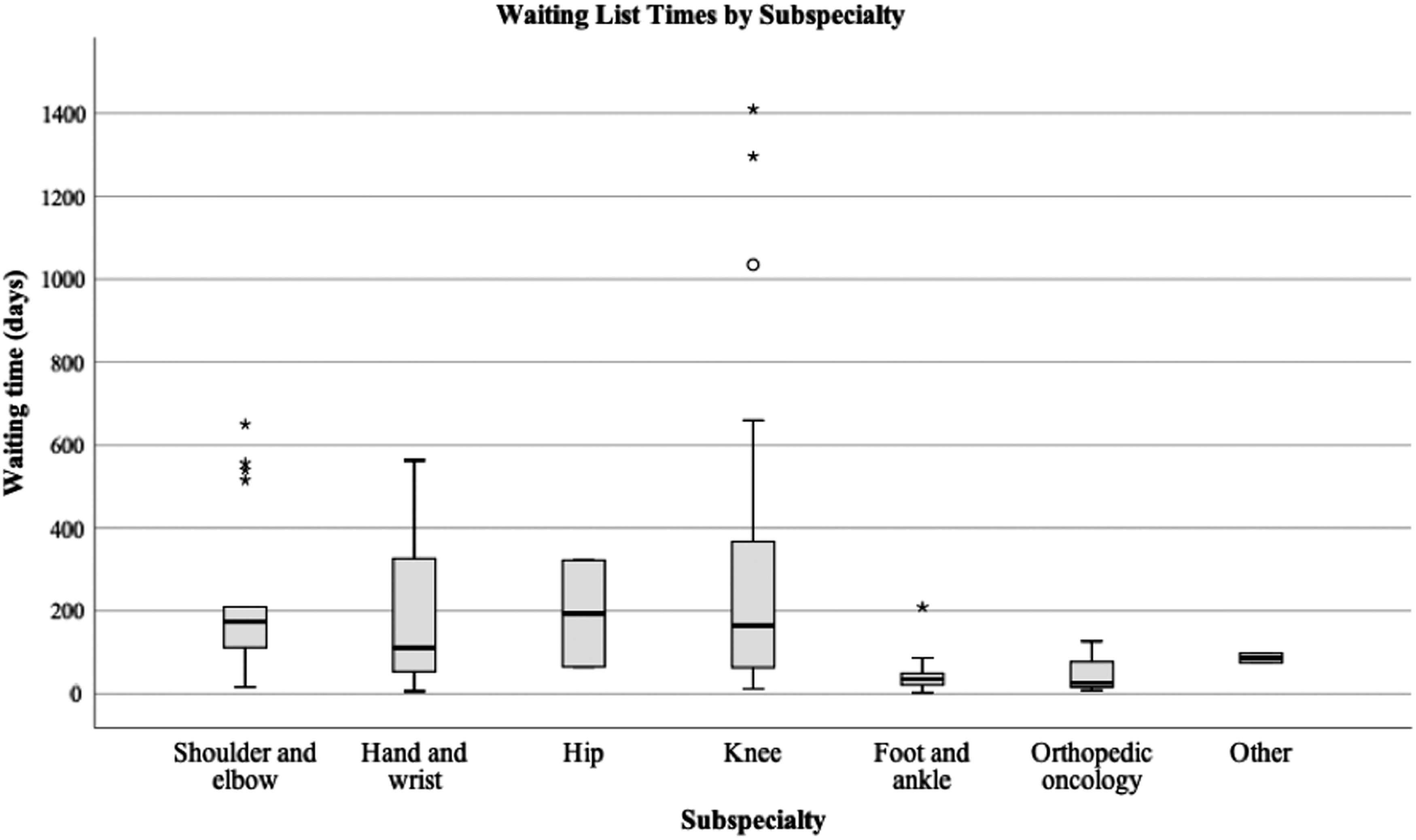
Waiting list times by subspecialty. *extreme outlier (value more than 3 times the interuqartile range). °represents an outlier with values between 1.5 and 3 box lengths from the upper or lower edge of the box plot.
After the first evaluation, physicians of the Calbuco Hospital were able to resolve 69.6% (204/293) of the cases. The remaining 30.4% (89 patients) were presented in a scheduled teleconference with the specialist. Of these patients, 57.1% were males and 42.9% females. Age in both groups was normally distributed and means did not show any significant difference between males (50.5 years, 95% CI 44.9–56.0) and females (51.8 years, 95% CI 45.3–58.4). Most of these consultations were related with knee problems (30.3%). Distribution of teleconferences by subspecialty is detailed in Figure 4.
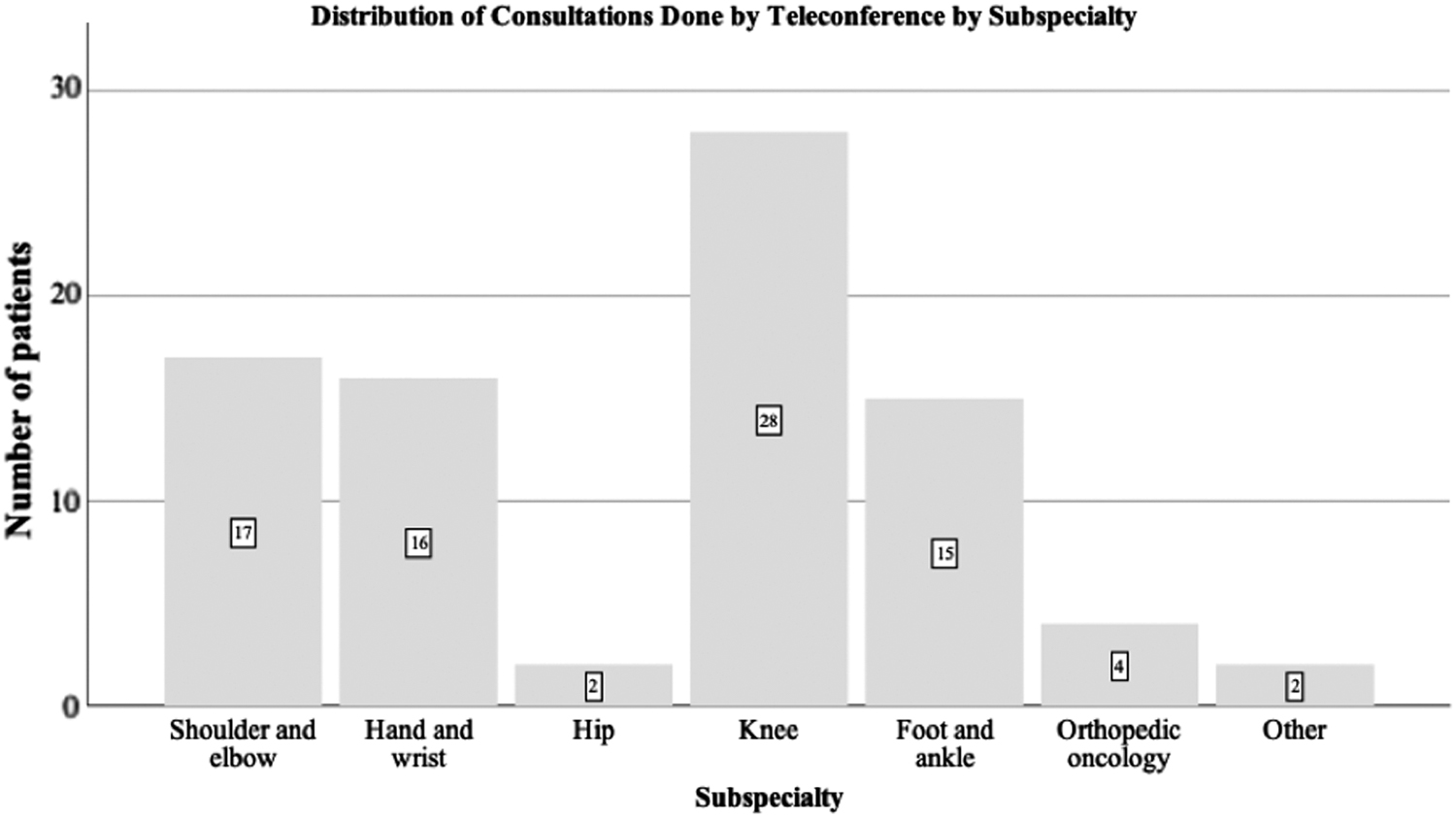
Distribution of consultations done by teleconference by subspecialty.
Of the universe of 89 patients evaluated by videoconference, 69.7% (62) required one or more follow-up sessions through tele-orthopedic and 30.3% (27) were referred for an on-site evaluation by an orthopedic subspecialist. The median number of consultations until achieving resolution was 2.0 (interquartile range 2.0–3.0).
The consultations by videoconference were mostly performed with the patient present synchronously (88.8%, 79/89 patients). In this instance, it was possible to have a conversation allowing to clarify or deepen on anamnestic aspects, speak about the diagnosis or therapeutic plans, and answer the patients' doubts and inquire into their expectations. On specific occasions, (11.2%, 10/89 patients), the clinical case and patient's examinations were presented synchronously, but without the patient during the connections. In these cases, the patients were subsequently cited by the physicians of the program to explain the diagnostic and therapeutic instructions that were given by the specialist. This modality was used for selected cases, including patients with challenging access possibilities due to inclement weather conditions and as long as there was no doubt regarding the physical examination or the clinical case itself.
The waiting list times of the referrals after the implementation of the strategy decreased on average from 201.4 to 40 days. Since the first assessment, the mean time until the cases were resolved was 46.9 days (95% CI 34.0–56.9).
Discussion
There is a collective recognition of the value of digital technologies to advances in universal health coverage, but there is also an urgent need to assess the use of digital technologies in health under normative and evidence-based guidance. As the Consensus Statement of the World Health Organization highlights: “to improve health and reduce health inequalities, rigorous evaluation of eHealth is necessary to generate evidence and promote the appropriate integration and use of technologies.” 12
There is available evidence that confirms these strategies can reduce the health care-associated costs of these patients being not only cost-effective but also convenient and accessible. 11,13 –15 It also improves the overall health care experience for rural patients who must undergo a surgical procedure. 16
To our knowledge, the implementation of this strategy under this format has not been widely explored in traumatology and orthopedics. There are some reports of tele-orthopedic programs in the United States, Australia, and some Nordic countries in Europe, 2,3,17 which showed promising results but with different operating modalities. Thus, this modality seems to be a new and effective way of implementing this tool.
Since there has been an increase of different telemedicine strategies in our health service, we wanted to measure the impact of implementing this new tele-orthopedic initiative on our health system and on the population's well-being. We understand that there are limitations to our work, but this is the first attempt to assess its benefits, harms, and feasibility and we want to set an example for all developing countries to systematize the work we do in the e-health field. It is also noteworthy that every digital health intervention has to be applied in its own local context. Therefore, we wanted to highlight the reality of our own target population, which is very different compared with other regions of Chile, while very similar to many remote areas in our country and the world.
Considering the concepts from Tanahasi framework 18 and the determinant layers of universal health coverage, 19 our work strengthens (1) the “supply” layer, as it guarantees access to qualified health workers with our available equipment; (2) the “demand” layer, as it allows for continuous follow-up of complex cases and allows the general practitioners from Calbuco to prioritize patients at higher clinical needs; and (3) the “affordability-cost,” as allowing local treatment for most of the patients significantly reduces their expenses. On the contrary, we recognize the need to improve the “accountability” and “quality” of the program, making it accessible to other rural populations in our region and guaranteeing better access to high-resolution images, as well as continuous training of doctors in terms of better physical examination.
In relation to this last statement, an important limitation for implementing a telemedicine strategy in traumatology and orthopedics is the need for specific physical examination skills to obtain proper information. In our experience, only a small percentage of patients required on-site attention by an orthopedic surgeon specialist after the videoconference, knocking down our initial concerns about this issue. Likewise, although lower quality images were expected of the Calbuco Hospital compared with images from the reference center (Puerto Montt Regional Hospital), this did not (according to the specialist appraisal) limit the efficiency of this strategy.
Physiotherapeutic support is an essential pillar in the treatment and rehabilitation process of traumatology and orthopedic patients. It is crucial to have this therapeutic tool available to achieve optimal results while developing this kind of initiative.
The improvements seen in the traumatology and orthopedic skills of the primary care physicians allowed for a better management of patients with musculoskeletal problems seen at that level and generated more attentive referrals. We observed they were able to verify the pertinence of the referrals made by other primary physicians and resolved the majority of them without the need of presenting the cases in tele-orthopedic videoconferences. Also, as previously reported, the strategy seems to enhance the primary physicians' competencies through continuous learning of new capabilities from interactions with the specialist. 20
As future challenges, we plan to extend this strategy to all the dependent districts of the Reloncaví Health Service with technical availability. The primary care physicians in charge of presenting the clinical cases will receive continuous training, ensuring the continuity of the strategy and its sustainability over time. Another challenge will be to measure patient's satisfaction and perceived benefits comparing this telemedicine strategy against the traditional on-site consultations.
A limitation of our project was that we did not enforce the use of patient satisfaction surveys to evaluate their experience with the initiative. We decided to implement this in the future as a way to incorporate this fundamental aspect of the evaluation process and improve the overall consistency of the results. The decision to replicate and spread the strategy warrants consideration of this central element, the evaluation by the recipient of the care strategy: the patient.
Finally, we will also measure the efficiency of this strategy in the medium and long term by evaluating whether training of primary care physicians has generated a decrease in the nonsurgical referrals in traumatology and orthopedics over a longer time span. This tele-orthopedic strategy has become a major asset to our rural population, and we hope to be able to increase its presence to achieve faster and more affordable ways of attending the inhabitants of geographically isolated places.
Footnotes
Acknowledgments
The authors acknowledge the local authorities for their support to this initiative. They also acknowledge Ignacio Wichmann for his help during the preparation of the article.
Disclosure Statement
No competing financial interests exist.