
Abstract
Background:
Hurricane Irma, a catastrophic Category 4 storm, made landfall in Florida on September 10, 2017. Nemours CareConnect (NCC) offered direct-to-consumer (DTC) pediatric telemedicine during Hurricane Irma.
Introduction:
Although other programs have examined disaster response and postdisaster recovery by using telemedicine, no studies report use of a pediatric-specific, DTC platform during all three phases of disaster management.
Materials and Methods:
This IRB-approved study is a retrospective analysis of NCC's audio-visual telemedicine encounters performed on September 8–16, 2017.
Results:
From September 8 to 16, 2017, NCC recorded 262 completed telemedicine visits. The mean wait time was 12.23 ± 14.4 min. The mean length of the telemedicine encounter was 10.12 ± 4.42 min. Most telemedicine visits occurred on the day before the storm (27.9%), followed by the day after the storm (19.5%). Most common chief complaints were upper respiratory symptoms (33.6%), skin-related concerns (19.1%), fever (16.8%), and gastrointestinal concerns (6.5%). Patient satisfaction remained high during the storm, for the provider as well as the platform.
Discussion:
During Hurricane Irma, NCC offered accessible and efficient care to families who were impacted by the storm throughout Florida. Results suggest a differential pattern of use before the storm's arrival, during, and immediately after the storm, which may be informative to other telemedicine providers.
Conclusion:
Further research is needed on the integration of telemedicine into the disaster preparedness plans at a local, state, and national level to ensure maximum support for those families in need.
Introduction
Telemedicine serves millions of patients and has the potential to assist those in need of health care during natural disasters. Hurricane Irma, which peaked as a catastrophic Category 5 on the Saffir-Simpson Scale, was the strongest hurricane in the Atlantic since Wilma in 2005. 1 Irma made landfall as a Category 4 hurricane, striking near Cudjoe Key, Florida, on September 10, 2017, followed by a second landfall as a Category 3 hurricane on Marco Island. Irma's sustained winds, which were in excess of 130 miles per hour, left 6.2 million Florida homes and 60% of the state without electrical power 2 and disrupted access to local health care facilities.
New studies have examined the use of telemedicine for the purpose of disaster relief. However, no studies report the use of pediatric, direct-to-consumer (DTC) platforms during all three phases (predisaster, during the disaster, and postdisaster) of emergency management. 3 –6 Of particular concern, children are often not considered in disaster planning. 7 Thus, there is a need to establish programs and develop frameworks that may bring aid to areas when disasters strike, particularly for children.
In 2015, Nemours Children's Health System, a pediatric health system of hospitals and clinics, launched a telemedicine initiative. The initiative began with Nemours CareConnect (NCC), which offers DTC, synchronous, 24 h per day, 7 days per week, urgent care to families with children from birth to 18 years of age. NCC's DTC board-certified pediatricians are licensed to provide pediatric health care to children residing in multiple states across the United States. Currently, Nemours has expanded their telemedicine services by incorporating the use of their sub-specialists and hospital teams to provide improved access to the children they serve.
In this retrospective analysis, we describe attributes of NCC functioning during Hurricane Irma. We examined pediatric medical needs, including frequency of accessing NCC during the three phases of disaster management, chief complaints, visit experience, and patient satisfaction of NCC users, over a 9-day timeframe as the storm advanced through Florida.
Materials and Methods
This study was approved by the Nemours Institutional Review Board.
Pediatricians
Six board-certified pediatricians covered the NCC platform during the study's timeframe. Three pediatricians were located in Northern Florida and three were located in the Delaware Valley.
Platform
NCC's equipment meets the criteria and complies with the current organizational and technological requirements. Specifically, NCC equipment is H.323 compliant with a live video resolution of 4 × Common Intermediate Format (CIF), and it has bidirectional connection at a minimum of 384 kilobits per second running 4 CIF at 30 frames per second. 8 To ensure secure data transmission and to protect patient information, all the video, audio, and electronic medical record components are encrypted from beginning to end.
Procedure
During Hurricane Irma's impact on Florida, NCC provided free audio-visual telemedicine visits through use of a coupon code, IRMA, offered on social networking sites such as the Nemours Facebook page. Access to the service otherwise was consistent with the standard operation of NCC. 9
To begin a typical telemedicine visit on the NCC platform during the hurricane, a parent downloaded the free NCC application onto their computer, laptop, tablet, or cell phone. The parent then entered their child's demographic and pharmacy information along with the Hurricane Irma coupon code, IRMA. After the selection of a provider, the patient and parent entered a virtual waiting room. The provider was notified and accepted the connection. While the parent provided the history, the provider assessed whether the visit was appropriate for telemedicine. Patients with complaints that warranted an in-person medical evaluation (e.g., dysuria, suspected strep throat, or ear pain) were referred to the nearest open facility. Once the provider deemed the visit appropriate for telemedicine, the provider guided the patient, with the parent's assistance, through a virtual physical exam. Peripheral devices were not used. After the physical exam, the provider discussed the assessment and treatment with the family. Before disconnecting, the provider confirmed the parent's understanding of the diagnosis and treatment. Once the visit was completed, the parent rated the provider and the platform by using a 5 Star rating system, whereby a rating of 1 reflected a poor patient experience, and a rating of 5 reflected the best.
Once the provider disconnected from the NCC platform, they logged into the electronic medical database (Epic Systems Corporation, Verona, WI) to document the telemedicine visit, electronically send medication orders to the pharmacy, and create an after visit summary (AVS). The AVS was added by the provider to the NCC platform. Parents were able to access the AVS from the NCC application at their convenience. For patients who entered data for their primary care provider, a copy of the encounter or progress note was sent through the Epic database to their pediatrician to maintain integrity of the medical home. To provide seamless service, the pediatricians in the Delaware Valley covered the platform when the pediatricians in Florida lost power.
For this study, data were obtained from the NCC database (patient gender, age, wait time, engagement time, and 5 Star rating for provider and platform) and Nemours' Epic database (chief complaint) inclusive of the service dates most impacted by the hurricane (September 8–16, 2017). In addition, we compared patient experiences during Irma and NCC's standard, business-as-usual (BAU) operation 9 to illustrate changes across several key variables during the storm's passing.
Results
Of the 369 families who requested an NCC visit during the target timeframe, 262 resided in a hurricane-affected region (Florida or Georgia), had a completed NCC visit, and were included in the study. Patients ranged in age from 1 week to 17 years, 11 months, and 51.5% were female. Most participating families (77.1%) received the NCC visit at no cost to them through use of the IRMA coupon code; 10 additional families received a discount on the standard cost of a visit through the use of another coupon being offered for follow-up care.
Chief Complaints
Chief complaints were consistent with conditions treated during typical NCC administration. The most common concerns prompting a telemedicine visit during the storm were upper respiratory symptoms (33.6%), skin-related symptoms (19.1%), and fever (16.8%). Chief complaints reported during Hurricane Irma are presented in Table 1.
Chief Complaints of Patients Seen by Nemours CareConnect During Hurricane Irma
Includes all other chief complaints that do not fall into the categories just cited.
ER, Emergency Room; GI, Gastrointestinal.
Patient Volume
As expected, patient volume increased considerably during the storm. The 262 telemedicine visits completed during the hurricane in September 2017 demonstrated a sharp increase from the 18 completed visits during the same 9-day timeframe in the prior year, resulting in a 1,355% increase in NCC visits. During Irma, the highest volume of visits occurred on September 9, 2017, 1 day before the storm's landfall. The NCC's actual patient volume during the storm in relation to the same timeframe in 2016 is presented in Figure 1.
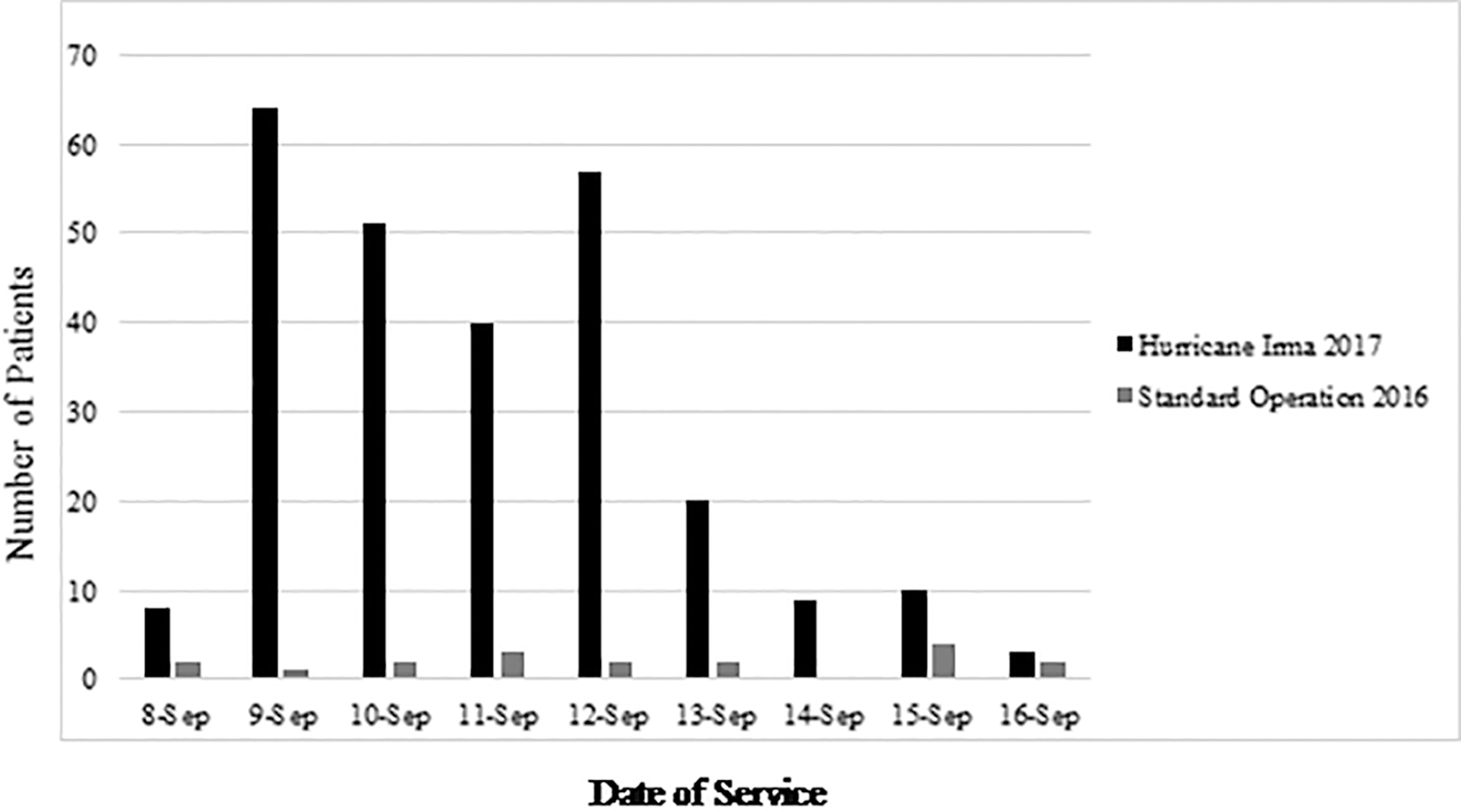
NCC Actual Patient Volume is shown during September 8–16, across two consecutive years. Hurricane Irma had a substantial impact on NCC's standard volume during the timeframe in 2017. NCC, Nemours CareConnect.
Wait Time, Length of Engagement, and Patient Satisfaction
The average wait time for a patient to be seen by a pediatrician during the storm was 12.23 min, ∼9 min longer than BAU. 9 In relation to BAU operation, patients waited significantly longer to begin their telemedicine visit during Hurricane Irma (F[1,1241] = 276.46, p < 0.001; η 2 p = 0.182). On average, visits during Irma were ∼3 min shorter than during BAU operation (F[1,1253] = 41.15, p < 0.001; η 2 p = 0.032). The provider was busy on request for services for 62.2% of calls. However, despite the longer wait times during the storm, patient satisfaction remained high—approaching 5 stars for both the provider and platform, an indication that patients and their families were appreciative of their ability to access care during the severe weather. A comparison of key attributes during Hurricane Irma versus standard operation is provided in Table 2.
Use of Nemours CareConnect During Hurricane Irma Versus Standard Operation
Means (standard deviations) presented, except where otherwise indicated. Wait time available for 98% of total patients. Engagement data available for 99% of total patients. Patient satisfaction data available for 69% of total respondents.
Patient data reported in Vyas et al. 9
Groups differ significantly, p < 0.001, two-tailed.
Discussion
NCC successfully met the increased demand for pediatric health services and was operational throughout all three phases of emergency management: predisaster, during the disaster, and postdisaster. When local conditions worsened, NCC redirected the demand to pediatricians in unaffected regions of the country and continued providing care. The NCC platform required no additional training, no manuals to review, and no new devices to implement, allowing for a seamless transition into “disaster mode.”
Families utilized NCC the most when preparing for Hurricane Irma's impact. When comparing the three phases of emergency management, the highest volume of visits occurred in the predisaster phase. The peak volume before the storm's onset suggests that many parents and caregivers may have anticipated a need for services for which they otherwise might not have had access, given the approaching threat of severe weather.
Upper respiratory symptoms were reported as the chief complaint for one-third of the Irma study sample, which was relatively higher than the 17.5% of respiratory complaints reported during BAU. 9 With this one exception, the frequency and nature of the chief complaints managed during the study period were similar to those managed during standard operations. 9 This finding is consistent with other published research that evaluated use of a DTC platform during a hurricane. 10 Hurricanes bring about a higher demand for services, but the type of care may remain routine. It may not be the acuity of the illness that differs but the heightened need for parents to prepare for the impact that is a critical component of disaster preparedness.
Despite longer wait times, patient satisfaction remained high as NCC pediatricians provided around-the-clock access to care to a greater volume of patients than typically observed. The use of a free visit coupon code available via social media sites during the storm meant that most parents could access the service with minimal financial concern.
Although telemedicine was first used for disaster relief more than 30 years ago, it remains limited and underutilized in disaster preparedness plans today. 11,12 Most disaster plans that are only functional when a disaster strikes require cumbersome changes such as re-learning a particular technology, or reviewing a disaster manual for updated guidelines. 13 However, DTC platforms are uniquely poised to convert “business as usual” to “emergency ready.” With the availability of wireless broadband technology, telemedicine programs continue to have a virtual presence even when parts of the hard-wired system go down during disasters. 13 This growing technological reliability coupled with the inherent accessibility to health care make DTC telemedicine a necessary part of any disaster relief plan.
Despite increasing awareness, resources dedicated to the pediatric population continue to be limited in addressing the needs of families during emergency medical response. 7 Our results indicate that pediatric DTC platforms have a unique advantage when providing care to children during emergency situations. Having access to a telemedicine pediatrician with whom to consult before a natural disaster may alleviate parental anxiety and prove beneficial when designing a family's disaster preparedness plan.
Limitations
The current analysis is limited to one platform and one weather event. Additional research is needed to further understand the benefits and challenges of having access to pediatricians via telemedicine during weather events and other emergency situations. Unlike tsunamis and earthquakes, hurricanes generally allow for preparation time. Studying prehurricane data will help pediatricians better address the needs of patients as a natural disaster approaches. Understanding the capabilities of pediatric telemedicine for disaster relief will be critical for the incorporation and implementation of telemedicine into local, regional, and national disaster preparedness plans.
Despite potential benefits during natural disasters, DTC telemedicine faces limitations. Liability, technical support, financial responsibility, and organizational culture are obstacles. 4 Providers who practice across state lines or internationally, and without access to a patient's medical record face complex regulatory and medical-legal barriers. Technical connections are often interrupted during the disaster. Existing telemedicine systems may need backup power or access to a satellite network when the current system is damaged. Having a knowledgeable technical team, when poor Wi-Fi or insufficient bandwidth prevents proper data transmission, is essential. Financial responsibility, whether taken by the central government or private payers, has not been clearly defined. Disaster response is currently governed by emergency management teams that have an organizational culture in place that guides allocation of resources and deployment of safety personnel. The incorporation of a DTC telemedicine team into the emergency response system requires financial support, time, and training. Though telemedicine is a promising resource in disaster preparedness, it remains marginalized. Addressing these barriers may assist with the integration of DTC telemedicine into future disaster relief plans nationally as well as internationally.
Conclusion
Our study suggests that pediatricians using DTC telemedicine platforms can deliver efficient health care to children in need of services during the course of extreme weather events. Importantly, use of the DTC platform facilitated a seamless transition from “business as usual” to “emergency ready” operations, due to 24/7 access and the engagement of physicians who delivered patient care from unaffected regions of the country. Patient needs for care were routinely met by the pediatricians on the DTC platform, despite extraordinary environmental conditions. Pediatric DTC telemedicine platforms should be considered and incorporated into local, regional, and national disaster preparedness plans as alternatives for patients who may not have access to their medical homes. Further research is needed on the integration of telemedicine into disaster preparedness plans to ensure maximum support to the families in need.
Footnotes
Acknowledgments
The authors acknowledge the contributions of the telemedicine pediatricians Rene Chalom, MD, Tatiana Zeballos, MD, and Wayne Ho, MD; as well as the technology team, and the operational support provided during Hurricane Irma.
Disclosure Statement
Dr. Murren-Boezem is employed by Nemours Children's Health System. She has no other conflict of interest to disclose. Dr. Solo-Josephson is employed by Nemours Children's Health System. She has no other conflict of interest to disclose. Dr. Zettler-Greeley is employed by Nemours Children's Health System. She has no other conflict of interest to disclose.
Funding Information
The research was funded by the Nemours Foundation.