
Abstract
Background:
Despite advancements in treatment for inflammatory bowel disease (IBD), surgery remains inevitable for patients and IBD management is costly.
Introduction:
Frequent postoperative monitoring is needed for early detection of both short-term complications and long-term disease recurrence. We developed a care pathway for postoperative home monitoring of IBD patients using telehealth applications.
Materials and Methods:
We performed a retrospective cohort study with a matched control group to assess the efficacy of the Tight Control Surgery Scenario (TCSS), a 4-week postoperative care pathway. IBD patients aged 18 or older who underwent an IBD-related intestinal operation between October 2013 and December 2015 were eligible. Enrolled participants submitted postsurgical questionnaires and wound photos through e-mail. We measured patient satisfaction with the care pathway and assessed its impact on 30-day postoperative hospital readmission rates, emergency department (ED) visits, and gastroenterologist (GI)-related office visits.
Results:
Sixty-four (n) cases were enrolled in TCSS and matched to 64 historic controls. Patients who completed the additional evaluation survey expressed overall satisfaction. Readmissions, 30-day ED rates, and GI visits were numerically higher in cases compared with controls, but this difference was not statistically significant.
Discussion:
TCSS demonstrates the feasibility of implementing a telehealth care coordination platform for postsurgery IBD management. Patients with more complications may have sent in more photos due to greater concern for maintaining their health.
Conclusions:
Implementation of TCSS for easy home monitoring is feasible. While we did not see reductions in ED visits, GI follow-up visits, or readmissions, patient satisfaction was high, thus demonstrating its feasibility for telehealth applications.
Introduction
Despite advancements in medical pharmaceuticals for inflammatory bowel disease (IBD), 1 up to 15% of ulcerative colitis (UC) patients will undergo surgery within 20 years of diagnosis and nearly 50% of Crohn's disease (CD) patients within 10 years of diagnosis. 2,3 Unfortunately, surgery is not always curative, but rather ameliorates symptoms. Up to 30% of CD patients will require additional bowel resections within 10 years. 1 Recurrence of CD postsurgical resection has also been shown to be at a rate of 55% 5 years postsurgery and 76% 7 years postsurgery, 4 demonstrating the high prevalence of disease recurrence. Additionally, postoperative morbidity remains high following intestinal surgery in CD with 30-day infectious complications and intra-abdominal sepsis as high as 30%. 5
IBD management is also costly due to excess utilization of health care services. Kappelman et al. found that the mean number of excess emergency department (ED) visits per 100 CD patients, compared with their non-IBD controls matched by gender, age, and geographic region, is 20.1; the mean number of excess ED visits per 100 UC patients was 10.3 when compared with controls. 6 In addition, it has been shown that the frequency of IBD-related ED visits has increased by ∼51% over the last decade 7 and the cumulative nationwide cost of IBD-related ED visits has increased by over 200% in the past decade. 7 The most costly cases included IBD patients who had a surgical stay. 8
Readmission after colorectal surgery is common, with rates ranging from 6% to 25% often due to bowel obstruction, surgical site infection, or abscesses. 9 Bliss et al. found that 14.7% of IBD patients were readmitted within 30 days after a colectomy. 10 Hospital readmissions after surgery are a significant driving factor of financial costs. One study found that 13% of patients readmitted after receiving a hospital resection required resources from the intensive care unit and 6% required a reoperation. The combined median direct cost was over twice as high for readmitted patients than for non-readmitted ones. 11 High costs associated with managing IBD after surgery underscore the need for more effective postoperative care management.
Given the complexity of IBD and risk of disease progression after surgery, frequent monitoring is needed for early detection of recurrence and complications. Telemonitoring has been shown to be effective in managing chronic diseases, including chronic obstructive pulmonary disease, 12 cardiovascular disease, 13,14 and IBD. 15 In IBD, a study on home telemonitoring in teenagers found that telemonitoring can decrease outpatient visits and costs of care compared with conventional follow-up. 16 In addition, the home automated telemanagement in ulcerative colitis (UC HAT) system showed gains in quality of life for patients using UC HAT compared with those receiving the best available care. 17 However, no significant improvements were found in medication adherence or disease activity, suggesting the need for further research in the effectiveness of telemedicine for IBD. 18 While there have been some conflicting findings, electronic health (e-health) interventions for IBD have overall been shown to improve quality of life, disease activity, and reduce health care costs. 19 To our knowledge, there has not yet been a published study conducted on telemanagement specifically for postoperative IBD care.
To address the high costs and complications of postsurgery maintenance, the University of California, Los Angeles (UCLA), Center for IBDs developed a care pathway for IBD-related surgery, designed to tightly monitor patients at home after discharge using telemonitoring tools to improve the experience. According to the 2011 Annual excHangE on the ADvances in Inflammatory Bowel Disease (IBD Ahead) educational program, robust monitoring should involve different clinical measurements. 18 Our pathway included postoperative symptom assessments, including endoscopic evaluations and self-reported patient outcomes. We hypothesized that frequent and proactive monitoring of IBD patients would improve the patient experience and could reduce postoperative complications and IBD-related hospital readmissions, thus improving postoperative management.
Materials and Methods
Design and Outcomes
After institutional review board approval (IRB no. 16-000263), we performed a retrospective cohort study with a matched control group to assess the effects of an electronic postoperative care pathway on patient experience and resource utilization. Enrolled patients followed a 4-week reporting schedule that culminated in a follow-up visit with a gastroenterologist (GI). Participants filled out daily to weekly online questionnaires about symptoms and wound healing and uploaded wound photos. Participants also had direct e-mail access to a specialized, surgical IBD nurse for questions.
We assessed the impact of the pathway during 30-day postdischarge on (1) hospital readmission rates, (2) ED visits, and (3) GI office visits. Secondarily, the number of wound photos submitted per case was measured to estimate Tight Control Surgery Scenario (TCSS) adherence.
Population
Patients aged 18 or older, who had an IBD diagnosis confirmed by endoscopy or radiological evaluation and underwent IBD-related intestinal surgery performed by a single IBD surgeon, were eligible for study inclusion.
Between October 2013 and December 2015, a research nurse identified cases from a surgical list and explained the TCSS study to patients by phone. Participants were then consented by the research nurse at their preoperative clinical visit. Patients who underwent surgery during that same time frame and were not assigned to the scenario were selected as controls (Fig. 1). We used a custom matching algorithm to make accurate, representative case–control matches based on age, gender, disease type, and type of surgery.

Flowchart of study design.
The Care Pathway: TCSS
TCSS is a 4-week program monitoring the recovery of IBD patients after surgery. All enrolled patients filled out a postsurgery questionnaire through e-mail for 4 weeks after discharge (Fig. 2). In week 1, they filled out the questionnaire and uploaded a picture of their abdominal surgery wound(s) every day. In week 2, they did so on days 2, 4, and 7. In weeks 3 and 4, patients filled out the questionnaire and uploaded a picture on day 7. A total of 12 questionnaires were collected over the course of 4 weeks. Pain was measured with a 0–10 Likert scale; wound healing was assessed through submission of wound photos; and bowel function was evaluated using ostomy output and stool frequency.
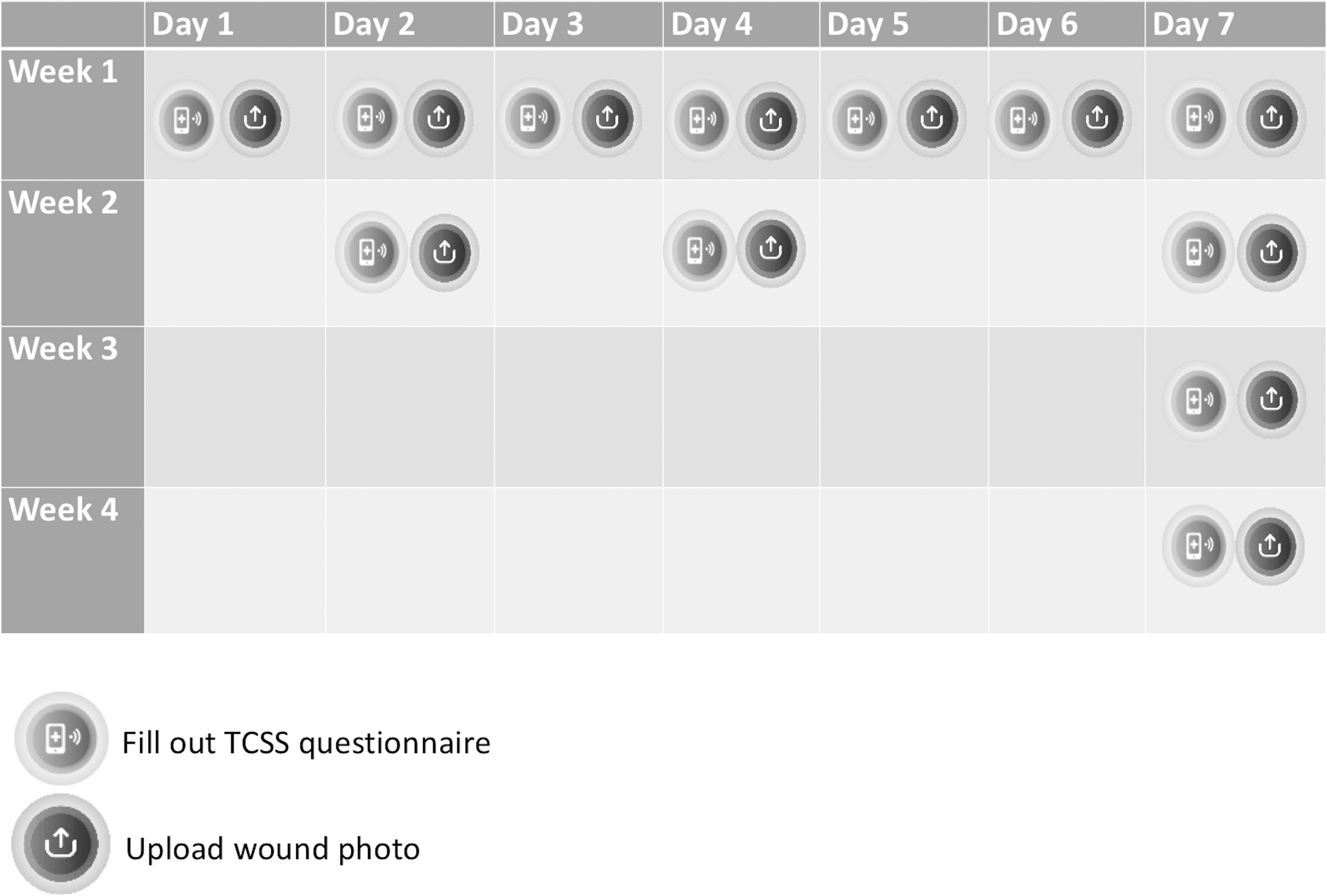
Calendar of the 4-week TCSS program. TCSS, Tight Control Surgery Scenario.
All questionnaires and wound photo uploads were completed by patients and sent by e-mail to a dedicated research nurse who also checked information and pictures daily to help monitor patients. After the 4 weeks, patients had a clinic visit with their GI, who closed this surgical scenario and decided with the patient the next steps for care.
Questionnaires and Definitions
Postsurgery TCSS questionnaire and picture uploads
Questions in the TCSS questionnaire (Table 1) were developed to identify abnormalities and to assess pain, weight, temperature, diet, and wound information. When patients responded with certain red flag answers, the surgical nurse would discuss the patient with the surgeon for appropriate actions. These red flags included certain answers that would be detected by nurses, including fever over 100°F; pain increase (visual analog scale) equal to or more than two points in 24 hours; ileostomy output lower than 500 mL or more than 1,000 mL; and bowel movements of 0 in patients without an ostomy.
Tight Control Surgery Scenario Surgery Questionnaire Form
An optional TCSS evaluation survey was administered to all cases 1 week after the end of the TCSS through e-mail. It contained questions gathering patient feedback on their experience in the TCSS.
Data Collection and Statistical Analysis
Data on the three measured outcomes (GI follow-up visits, ED visits, and hospital readmission) were collected from electronic medical records and clinic visit summaries for both cases and matched controls. Data on ostomy output, wounds, and physiological conditions (temperature and diet, etc.) were collected from patient-reported outcomes (PROs) through the TCSS for the cases only.
TCSS participants and matched controls were compared to assess the effect of the TCSS on GI follow-up visits, ED visits, and hospital readmissions. We matched each of the 64 TCSS cases to a control patient based on patient characteristics (age, gender, disease type, and type of surgery).
Cases were matched to controls by calculating the matching distance between every case and every potential control based on age, gender disease type, and type of surgery. The closer the match between case and control in features (age and gender, etc.), the smaller the distance and more appropriate the match. The algorithm matches every case to the closest control, but if a later case is found to be a closer match to a control that has already been assigned, it is subsequently assigned to the later case. This leaves some unmatched cases at the end of the first iteration. The algorithm goes through those that are still unmatched until all 64 matches are made.
For statistical purposes, we considered the matched case and control to be the same subject with two different sets of outcomes, one in which they use the telemonitoring (TCSS) and one in which they did not. We used a McNemar test to compare proportions between cases and controls. We used a two-proportion z-test to compare outcomes between low (0–3 photos) and high (≥4) numbers of wound photos.
Results
Sample Characteristics
In total, 64 cases were enrolled in the TCSS pathway. Of 108 historic controls identified in the patient population who did not choose to participate in the TCSS, we matched 64 with our cases based on age, diagnosis, and surgery characteristics (Table 2). Our case and control samples were both predominantly Caucasian (76.5% and 71.9%, respectively) and had never smoked (70.3% and 68.8%, respectively). Median age of cases was 35 years and 48% were male. Median age of controls was 33.5 years and 60.9% were male. A greater number of cases than controls used biological therapies, antibiotics, and 5ASA. In the cases, 50% (n = 32) of the surgeries were for CD, 44% (n = 28) were for UC, and 6.3% (n = 4) were for indeterminate colitis. Case surgeries included bowel resection, colectomy, ileostomy, and stomas. The 64 matched historic controls had a median age of 33.5 and 61% were male. Of the controls, 50% of surgeries were for CD (n = 32) and 50% were for UC (n = 32).
Patient Demographics
5-ASA, 5-aminosalicyclic acid; COPD, chronic obstructive pulmonary disease.
Mean number of wound photos sent was 3.8 (median of 3 wound photos). Average daily stool frequency was 6 in patients without ileostomy; patients with an ileostomy had an average ileostomy output of 930 mL; an initial pain score of greater than or equal to 5 was reported in 34% of patients, and an average 2-point decrease was observed during the program.
Patient Experience
Sixteen patients (25%) enrolled in the TCSS pathway opted to complete the postsurgical care survey (Table 3). Patients expressed overall satisfaction with the program, with 81% describing their experience as excellent and 94% describing the amount of TCSS questions as reasonable. Patients reported that without participation in the TCSS pathway, they would most likely have used a phone call to the doctor's office as a resource for care (94%). Additionally, 56% of patients felt their recovery would have had a different result without participation in the TCSS program.
Patient Experience
Questions of the postsurgical care survey with proportion of respondents (n = 16) who answered. Question no. 5 was open-ended, allowing participants to list suggestions for change. Many opted to highlight positive aspects of the program for this question.
ER, emergency room.
In the postsurgical care survey, patients were also able to provide optional comments on their experience in the TCSS program. Two (13%) patients indicated that they would not change the program when asked what they suggest could be improved. Three (19%) expressed feeling comforted that they were receiving personalized follow-up care. Five (31%) patients expressed positive satisfaction with the ease of accessibility to the care team. One patient stated, “I loved knowing that someone was always checking up on me and my recovery through the e-mails. It was nice knowing that I could ask any questions I had at any time. I probably would have felt a little lost, on my own, and stressed out without the program.” Another patient expressed, “I just knew I had expert help just a click away to someone who knew me.”
Other patients gave feedback on ways to improve the program. One participant suggested having a more personal follow-up process in addition to e-mails, such as having a care coordinator check in with phone calls. A notable comment from another participant was that they would have liked to receive feedback from staff about the wound photos patients sent in.
Clinical Outcomes (ED Visits, Readmissions, and 30-Day GI Follow-Up Visits)
Readmissions, 30-day ED rates, and GI visits were numerically higher in cases compared with controls, but this difference was not statistically significant (Table 4). ED rates were 20% in the control group and 25% in cases (p = 0.677); readmission rates were 22% in the control group and 22% in cases (p = 1.00); and finally, GI follow-up rates were 47% in controls and 58% in cases (p = 0.265).
Summary of Results
ED, emergency department; GI, gastroenterologist; IBD, inflammatory bowel disease; SD, standard deviation; TCSS, Tight Control Surgery Scenario.
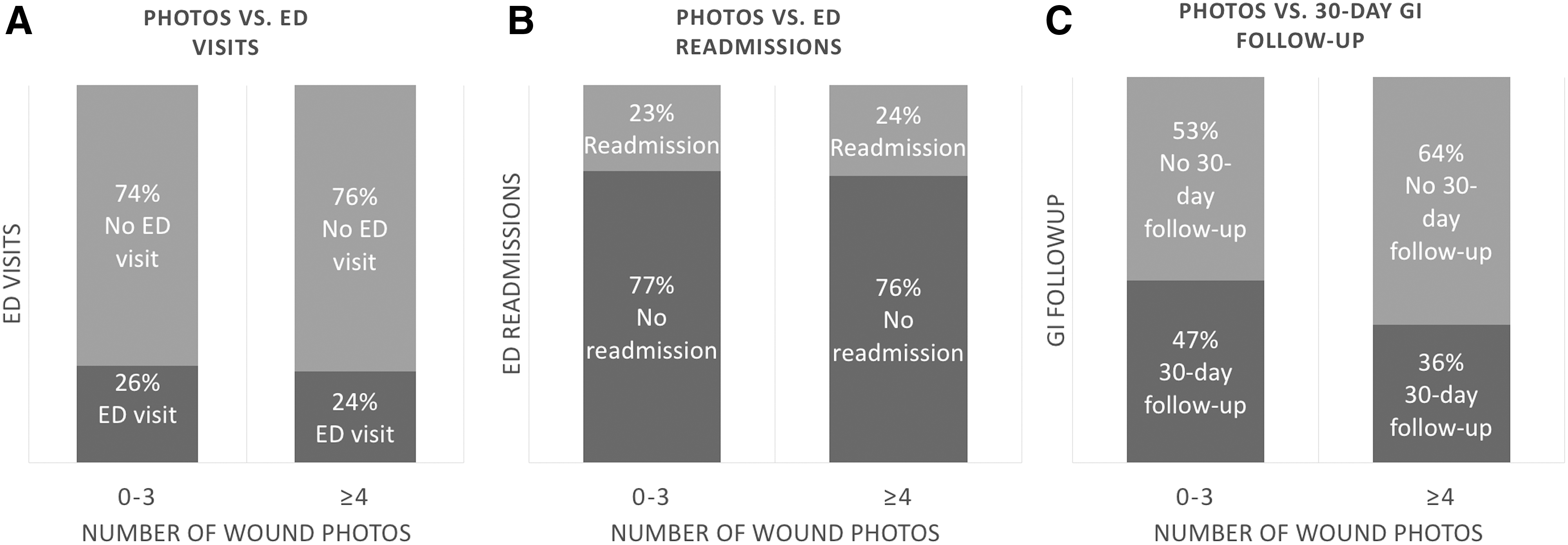
Patients who sent in four or more wound photos (more adherent to the care pathway) were more likely to have a 30-day GI follow-up visit (not significant; Fig. 3). There was no difference in the number of ED visits or readmission rates between patients who submitted greater than four wound photos and those who submitted fewer.
Discussion
We developed and investigated the feasibility and efficacy of a telehealth pathway in reducing 30-day readmission rates, ED rates, and GI follow-up visits. Our TCSS pathway demonstrates the feasibility of implementing a telehealth care coordination platform for postsurgery IBD management. By having patients fill out frequent questionnaires after hospital discharge, we were able to monitor PROs and identify complications. For instance, if a patient reported that their abdominal pain increased, the patient was called for triage by a surgical nurse who consulted with the IBD surgeon. If it was deemed necessary by the care team, the patient would be called in for a clinic visit or change of medication. The acceptability of the pathway was high, with 81% (13/16) rating their experience as excellent.
As indicated by our postsurgical care survey results, patients felt that they were cared for and comforted during their participation. They particularly appeared to be reassured by the ease with which they could access their care providers, suggesting the importance of increased accessibility to care teams in e-health applications. A majority of those who responded chose to answer the open-ended question about suggested improvements with either positive feedback or no suggested changes. Those who did suggest changes seemed to call for more involvement and communication from the care team, further highlighting the importance of accessibility to the care team. Despite the relatively small sample size of respondents to this survey, overall patient satisfaction showcases the potential of this telehealth intervention to enhance patient experience.
Our adherence rates also indicate that patients were active participants in the pathway. This in line with a previous study conducted by Con et al. who found that a majority of IBD patients have internet access and feel confident entering information into a computer or phone. 20 Despite the relatively small sample size (n = 86), their study demonstrates the willingness of patients to participate in telehealth solutions for disease management. In addition, previous studies assessing care coordination through the use of mobile technologies have shown efficacy in cancer, 21 HIV, 22 and diabetes. 23 Such complex chronic diseases, including IBD, should strive to involve more patient engagement in their care.
One of the aims of the TCSS was to increase the likelihood that patients would attend a follow-up visit with a GI to restart or optimize medical management postoperatively. Indeed, we found that numerically more TCSS patients had a postoperative GI visit. We also found that patients who sent in four or more wound photos were more likely to have a GI follow-up visit. We hypothesize that patients with more complications may have sent in more photos due to greater concern for maintaining their health and seeing their GI physician more frequently. Alternatively, GI patients who sent in more photos seemed to demonstrate higher adherence to our program.
This study has some limitations. Despite our best efforts to match patients to similar controls, a selection bias might have occurred; it is possible that patients who opted in to the TCSS were at higher risk for complications compared with their matched controls. This is supported by the observation that patients included in the TCSS had a higher rate of biologic use then the control group (Table 2), potentially reflecting more severe disease. Our study might also suffer from measurement bias; it is possible that we observed more ED visits, hospitalizations, and complications in our TCSS group because TCSS patients were more likely to return to our hospital as we followed-up with them more closely, while controls might have been more likely to go to an outside hospital. This is consistent with findings in other telemonitoring programs such as Constant Care, in which higher relapse rates were found in the intervention group, likely due to a higher detection rate. 24 As our sample population was predominantly Caucasian and treated by a single surgeon, our findings may not be representative of the general IBD population based on geographical or racial identities. The relatively small sample size could have affected the significance of our results, limiting the generalizability of our findings. Similarly, our small sample size of 16 respondents to the postsurgical care survey limits how representative our findings are.
Still, the use of telemedicine interventions in a postoperative setting has shown potential for enhancing clinical outcomes. Williams et al. found that complication rates for certain elective low-risk procedures were not statistically different from traditional clinical follow-ups. 25 Clinical outcomes from telemedicine use are therefore comparable with that of traditional clinic follow-ups. Additionally, Gunter et al. conducted a systematic review of 21 articles on the use of telemedicine in postdischarge surgical care. Similar to our study, they found high patient satisfaction rates and significant patient-reported savings of time, travel, and distance; one study reported savings in the health system due to an increased availability of clinic slots for new patients. 26 No studies have reported statistically higher complication rates in telemedicine interventions for postsurgical care compared with traditional follow-up visits. 25,26
Although we did not find statistical significance in the three main outcomes assessed (30-day ED visits, readmission, and GI follow-up visits), future studies should evaluate other health care utilization outcomes in addition to these, such as visits to walk-in clinics for pain or consultations with nontraditional providers. In addition, previous studies have demonstrated the financial burden of resource utilization and care management for IBD patients, particularly those undergoing surgery. 11,27 While our study did not assess reduced costs associated with increased self-management through the use of telemedicine, future studies should also include cost analyses to determine the optimal cost-effective method for postsurgery maintenance.
To our knowledge, this is the first study assessing a telehealth intervention involving both patient and provider aspects for postsurgery IBD management. This module aimed to make patients feel safe, prevent complications from happening, and intervene earlier in case of disease complications. TCSS is one pathway that has the potential to allow for monitoring and detection of postsurgery complications. It was well received by enrolled patients, supporting the use and acceptability of a telehealth intervention for patient care.
Authors' Contributions
A.Z. and D.H. were involved in study concept and design; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis; and study supervision. A.N. was involved in study concept and design; acquisition of data; drafting of the manuscript; and critical revision of the manuscript for important intellectual content. Z.S. was involved in analysis and interpretation of data and statistical analysis. W.D., A.L., R.J., and J.S. were involved in study concept and design and critical revision of the manuscript for important intellectual content. A.P. and S.R. were involved in acquisition of data and administrative, technical, or material support. E.K. was involved in acquisition of data; administrative, technical, or material support; and critical revision of the manuscript for important intellectual content.
Footnotes
Disclosure Statement
For A.Z., A.N., Z.S., A.P., R.J., S.R., E.K., J.S., and D.H., no competing financial interests or conflicts of interest exist. W.D. has received speaker fees from Ferring. A.L. has worked as a consultant for Takeda.
Funding Information
No funding was received for this article.