
Abstract
Background:
Patient decision aids (PDAs) facilitate shared decision-making (SDM) and are delivered in a variety of formats, including printed material or instructional videos, and, more recently, web-based tools. Barriers such as time constraints and disruption to clinical workflow are reported to impede usage in routine practice.
Introduction:
This pragmatic study examines use of PDAs integrated (iPDAs) into the electronic health record (EHR) over an 8-year period.
Methods:
A suite of iPDAs that personalize decision-making was integrated into an academic health system EHR. Clinician use was tracked using patient and clinician encrypted information, enabling identification of clinician types and unique uses for an 8-year period. Clinician feedback was obtained through survey.
Results:
Over 8 years, 1,209 identifiable clinicians used the iPDAs at least once (“aware”). Use increased over time, with 2,415 unique uses in 2010, and 23,456 in 2017. Clinicians who used an iPDA with at least 5 patients (“adopters”), increased by 82 clinicians each year (range 56–108); of clinicians who used the tool once, 54.3% became adopters. Of 261 primary care clinicians, 93.5% were aware, 86.2% were adopters, and 80.5% used the tools in the last 90 days. Clinicians perceived the iPDAs to be convenient, efficient, and encouraging of SDM.
Discussion:
We demonstrate that use of decision aids integrated into the EHR result in repeated use among clinicians over time and have the potential to overcome barriers to implementation. We noted a high degree of clinician satisfaction, without a sense of increase in visit time.
Conclusion:
Integration of PDAs into the EHR results in sustained use. Further research is needed to assess the impact of iPDAs on decisional quality.
Introduction
Patient decision aids (PDAs) are used by clinicians and patients to facilitate shared decision-making (SDM) and increase patient knowledge and lower decisional conflict. 1 They are delivered in a variety of formats, including printed material or instructional videos, and, more recently, web-based tools. 2 Randomized trials of PDAs to date fail to demonstrate usage in routine practice due to reported barriers such as time constraints, lack of skill sets and disruption to clinical workflow. 3 –6 There is consistent literature identifying a gap in tools for decision-making in the clinical encounter and a new approach is needed to offer clinicians and patients access to PDAs within the clinical workflow. 7 The electronic health record (EHR) is the hub of the modern office visit, and represents a natural focal point for integration of PDAs. Prior work using the EHR to document risk scores are published, and yet challenges remain to connect these efforts with SDM at the point of care with the patient. 8,9 This study examines use of a suite of PDAs integrated (iPDAs) into the EHR for an 8-year period.
Methods
DECISION AID DEVELOPMENT
A suite of iPDAs developed by clinicians (HealthDecision, Madison, WI) calculate and display personalized risk estimates by connecting data existing within a patient's EHR to evidence-based risk calculators in an automated manner. The first iPDA of the suite was launched in 2010 (CV [cardiovascular] risk tool) after an iterative development process. Discrete data in the EHR informed the risk calculator variables. Data such as age and gender were easily identified; defining other variables, such as history of congestive heart failure (CHF), required input from a group of stakeholders. When possible, predefined variables within the EHR (e.g., CHF used in hospital-wide quality improvement initiatives) were leveraged.
A usability study of the CV risk iPDA was performed in 2010 using standardized patients in primary care clinics in collaboration with human factors and health systems engineering. 10 Four additional iPDAs were added between 2014 and 2017, covering stroke prevention for atrial fibrillation, fracture prevention in osteoporosis, and breast and lung cancer screening (Supplementary Data). The evidence-based risk calculators are reviewed monthly to ensure relevance. Graphical representations of the calculated risks and benefits are viewed by the patient and clinician together and documentation of the SDM process is automated. Patients and clinicians view the PDA on the computer during the visit, and a printout is generated for patients to take home, displaying the results of their final decision-making (Fig. 1). A highlight of this iPDA's design is its approach to displaying percentages and statistics by utilizing colored figures of individuals to help patients better visualize their risk (Fig. 2).

Use of an iPDA into the EHR in the clinical encounter. EHR, electronic health record; iPDA, patient decision aid integrated. Published with permission of the participant.

Example of an iPDA into the EHR for choices around stroke prevention in atrial fibrillation. The point-of-care iPDA can be launched from a commonly used EHR during the clinical encounter. The user selects the “HealthDecision” tab, launching a separate linked application in which relevant patient demographics and laboratory information are autopopulated. The user can select various drug or device choices and, in real time, present a graphical interface to inform the patients regarding the risks and benefits of individual choices. This may assist in prompting elicitation of patient preferences, leading to a shared decision-making process. This iPDA also can return text and graphical data into the progress note and take-home materials for the patient.
Measuring Clinician use of Decision AID
Data were transmitted from the EHR to HealthDecision, including patient and clinician encrypted information, such as clinical data for risk calculation. The EHR enabled identification of clinician categories, including physicians, advanced practice providers (APPs), or other clinically active staff who as a group used the tools with at least 10 unique patients; clinician types were reidentified for analysis. Multiple uses of the same tool by the same patient–clinician pair within 6 months were considered one use. Clinician use was classified into two categories: (1) “awareness,” meaning use of the iPDA with one patient and (2) “adoption,” meaning use with at least five patients.
Clinician Survey
Clinician adopters were asked to participate in a voluntary survey through e-mail. Using Microsoft Excel, frequencies and proportions were calculated. Written responses were reviewed using a thematic analysis approach. Data were collated into groups that had meaning related to the question of clinician attitudes and input on use of the tool with their patients through independent coding. Final themes were developed independently by two coauthors (M.C. and M.E.F.), and then reviewed to select overlapping themes by consensus.
This pragmatic study was designated as a quality improvement initiative under the guidance of University of Wisconsin Institutional Review Board.
Results
Clinician use of Decision AID Over Time
Data collection included all iPDA uses between February 2, 2010 and December 31, 2017. For the 8-year analysis period, 1,209 identifiable clinicians demonstrated awareness of the iPDAs by using the tools with 57,116 unique patients, comprising a total of 81,728 visits. Of the clinicians, 76% were physicians, 16% were APPs, and 8% were other clinicians. There were 2,607 unique patient–clinician uses in 2010, which grew to 7,966 in 2014, and accelerated to 24,384 in 2017 (Fig. 3). There was an average increase of 151 new clinicians per year (range 99–302).

Unique patient–clinician pairs using iPDAs annually.
ADOPTION RATES OF DECISION AID
Adoption, defined as clinician use of the tool with at least five unique patients, was achieved by 657 clinicians for the 8-year period. On average, 82 new clinicians adopted the iPDAs each year (range 56–108), and 54.3% of clinicians who were aware of the tools became adopters. We selected five uses as the adoption threshold as the likelihood that clinicians would use the tool again increased with each use, beginning at 70.4% after the first use to 96.9% after five uses. The denominator of all clinicians at the institution was not available given the varying staffing for the study period. Thus, adoption rates for the entire hospital system were only calculated among aware clinicians.
In an effort to describe rates of recent use, we examined use in the last 90 days before the end of the study among primary care providers (PCPs) in active practice. A total of 261 clinicians (MDs, DOs, and APPs), excluding trainees, were listed as current PCPs as of the time of the evaluation. Within this select group, 244 (93.5%) were aware of the tools, 225 (86.2%) were adopters, and 210 (80.5%) had used the tool during that time period. For the adopters, mean usage was 227 patients, median 166 (range 5–1501).
Results of Clinician Survey
In 2016, 333 clinicians volunteered to participate in a survey on iPDA use and 109 (32.7%) completed the survey. The clinicians had used the tool at least five times (range 5–719, mean 90 unique patients) and thus represented a sample of adopters. To focus analysis on a class effect, qualitative responses were not separated by iPDA type. Many clinicians perceived that the iPDAs helped patients understand the benefits and harms of the choices (98.1% agree or strongly agree). In addition, 93.5% of clinicians felt the iPDAs improved decisional quality by leading to greater congruence of decisions with patient values. Patient satisfaction was perceived by clinicians to be higher when an iPDA was used (82.6% agree or strongly agree). Finally, 73.8% of clinicians said that they felt visits with an iPDA took a similar amount of time, or were more efficient, than usual care (Fig. 4
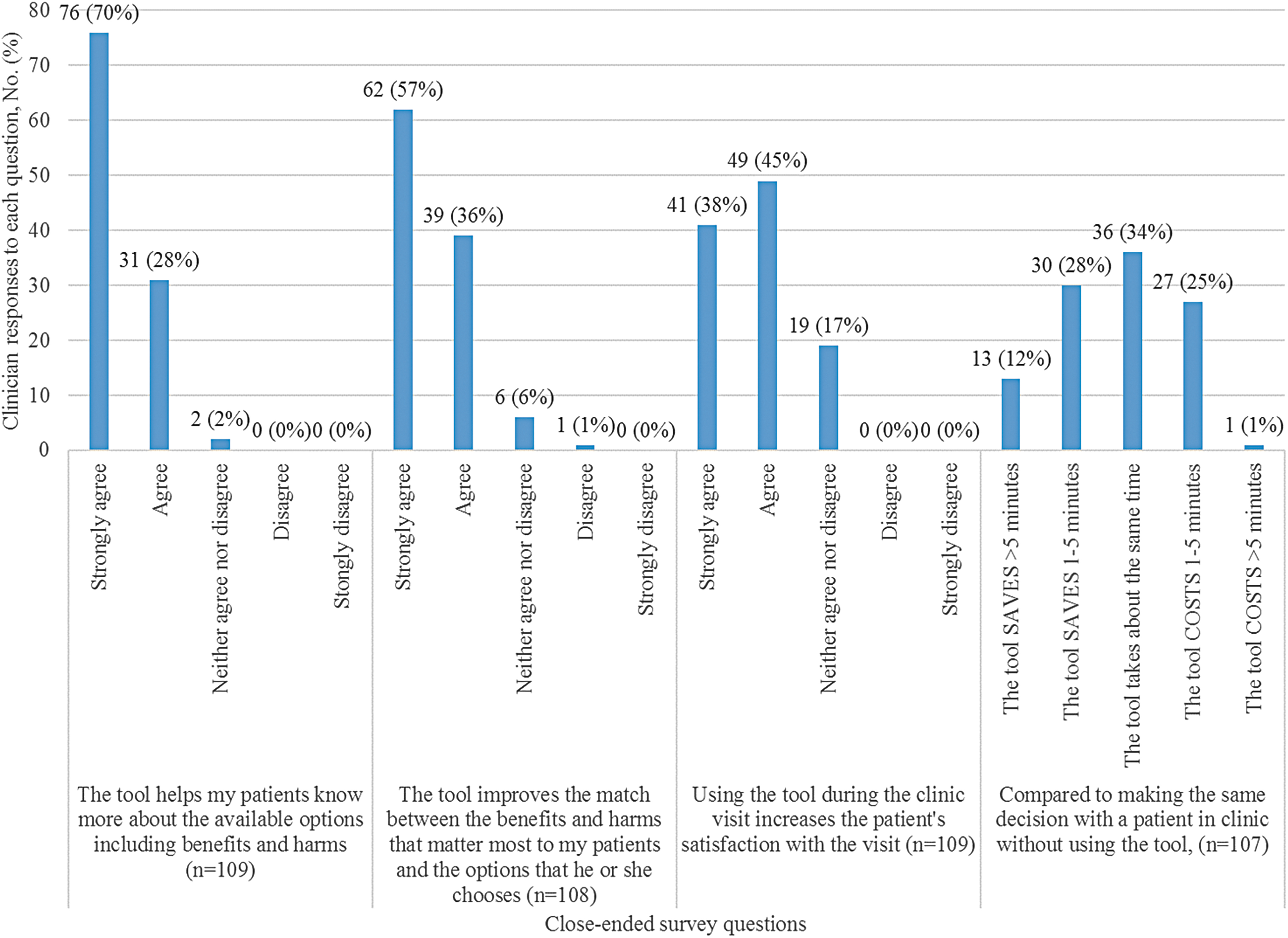
Clinician responses to close-ended survey questions regarding a suite of iPDAs into the EHR (described as “the tool” in the survey).
Discussion
We demonstrate that use of decision aids integrated into the EHR results in repeated use among clinicians over time. A high rate of sustained implementation is seen after fifth use. The delivery of the iPDA within the clinical workflow through the EHR has the potential to overcome barriers to implementation, including perceived lack of time and disruption to usual care. We noted a high degree of clinician and perceived patient satisfaction, without a sense of increase in visit time.
It is noteworthy that data were collected for a long period, with information on unique patient–clinician pairs using the tool in real-world practice. Few previous studies examine real-world use of iPDAs over the course of years and outside of a research protocol. In addition, many web-based PDAs that track usage patterns are prone to estimates of overuse because they do not allow specific user and patient identifiers.
Prior research focused on attempts to facilitate SDM processes by using PDAs that patients review before the visit (e.g., booklets, video, and websites). 11,12 Recent literature highlights the barriers at the system level: time constraints, lack of incentives, and clinician attitudes. 5,13,14 There is growing evidence that the integration of PDAs into the clinical workflow may offer clinician benefits such as automated risk prediction and improved documentation of SDM, although challenges remain to complete all tasks in the brief clinical encounter. A recent randomized trial of a point-of-care device for CV risk assessment demonstrated that clinicians used it for risk prediction, but not to assist in patient education or discussions regarding options available. 8 Finally, documentation of use of PDAs and SDM continues to be a focus of implementation in light of recent mandates for SDM from payers and professional societies; best practices for meeting these requirements are not well defined. 15 –17
Limitations
There are a number of limitations to our study. Use of the tool was not randomized and there was not a control arm; thus, the benefit over usual care cannot be estimated beyond qualitative review of clinician feedback. We were also unable to provide data on the presence of SDM or assess patient outcomes. Therefore, it is outside the scope of this study to assess whether the quality of care improved after adoption of the iPDAs.
The qualitative review is limited by the low response rate. This population of adopters was likely more enthusiastic about the tool than other clinicians, highlighting a response bias. It is noted, however, that clinician decisions to use the tool sustainably were driven by their own impressions of the usefulness in their patient encounters, without hard stops or prompts in the EHR. The study also did not include patient feedback on the usefulness of the tool. Although clinicians were asked about their perceptions of the patient experience, prior literature suggests that physicians are poor measures of patient satisfaction, and struggle to accurately self-assess the quality of the clinical encounter. 18 –20
Conclusions
Integration of a PDA (iPDA) into the EHR led to repeated use by clinicians over time. Clinicians report satisfaction with the iPDA both in terms of its clinical usefulness and efficiency. Further studies are needed to assess whether iPDAs lead to improved patient-centered outcomes and SDM.
Footnotes
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure Statement
Dr. M.C. has received honoraria from Boston Scientific, Edwards LifeSciences and W.C Gore. Dr. J.G.K. is the Founder of HealthDecision, Inc., The remainder of authors have no conflicts to report.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.