
Abstract
Background:
There are inequities in the provision of oral health care, and a large proportion of the population face challenges in accessing public dental health care options.
Introduction:
Teledentistry (TD), a new branch of telemedicine dedicated to dentistry, is a potential approach that can be used to overcome these challenges. Therefore, the purpose of this integrative review was to collect information regarding the inclusion of the application of TD tools in the public dental health services.
Methods:
Five electronic databases (PubMed/Medline, Virtual Health Library, CINAHL, Scopus, and Web of Science) were searched for relevant articles if they reported on original data related to the use of TD in public dental health services.
Results/Discussion:
Twenty-four studies met the inclusion criteria and were, consequently, included in the review. Our key findings indicated that TD can be used for training and continuing education of professionals, for remote patient care, to exchange information among health professionals, and orientation. It increases the access to dental care and enables general practitioners to interact with specialties. The benefits include cost-effective health equity services, improve dental knowledge, and reduce consultation waiting time. However, despite the advances made with the use of this technology, there are still some obstacles to overcome, such as limited infrastructure, low levels of motivation and the lack of compliance, professional resistance, and legal and security issues.
Conclusion:
TD may be very a useful tool for dental public health increasing the quality of the care by improving access, professional education, and patient satisfaction.
Introduction
Oral health is an essential component of good health, which is a fundamental human right. 1 However, the inequities in the provision 2 of oral health care and difficulties in accessing oral health services still are major public health challenges. 3,4 Some of these problems are related to the following concerns that are usually observed around the world, especially in developing countries and in those that have hard-to-access remote areas, 5 –8 the lack of access to oral health care, high or unaffordable costs of dental treatments, growing and aging populations, workforce migration, long distances from specialists, and shortage of dental professionals.
In circumstances such as these, every effort made to improve the access to oral health services is welcome. This is the case with the new information and communication technologies (ICTs), such as teledentistry (TD) that are being developed to help decrease the inequities observed in the provision of oral health services and to improve their quality. 6 –8
TD is a new branch of telemedicine that is dedicated to dentistry. It makes use of ICTs, especially of the internet, to exchange clinical information and associated images 9,10 to provide consultation services among professionals and health care providers 11 over long distances.
To the extent of our knowledge, no integrative literature review articles have been published regarding the inclusion of the use of TD in dental public health services that have demonstrated its various applications and benefits. In this case, the authors considered “public health” as defined by MeSH Terms, as those programs or actions enacted at a community, state, or federal level. Therefore, the purpose of this integrative review was to collect the available information on the methods through which TD is implemented in this context.
Methods
This review followed the five-stage integrative review process that involves the following steps: (1) problem identification, (2) literature search, (3) data evaluation, (4) data analysis, and (5) presentation and interpretation of the results. 12
LITERATURE SEARCH PROCESS
Searches were conducted on five electronic databases (PubMed/Medline, Virtual Health Library, CINAHL, Scopus, and Web of Science) using both medical subject headings (MeSH terms) and keywords. The following terms were used for the literature search: “Public Health Dentistry” OR “Community Dentistry” OR “Dental Health Services” OR “Oral Health Services” OR “Dental Care” OR “Dental Public Health” combined with “Teledentistry” OR “Telemedicine” OR “Mobile Health” OR “E-health” (Table 1).
Search Terms and Their Structure
INCLUSION CRITERIA
The inclusion criteria were studies reporting on original data related to the inclusion of TD applications in dental public health services, including dental health programs or dental health-related actions taken at a community, state, or federal level. Studies that were published in English, Spanish, and Portuguese from 2007 to June 2019 were included. Three researchers (C.B.C., F.S.P., and A.L.S.F.M.) independently screened titles and abstracts to identify articles that potentially met the inclusion criteria. The full-text articles that were potentially relevant to the subject of the review were retrieved and reviewed independently by the same three authors (C.B.C., F.S.P., and A.L.S.F.M.), and articles were selected for the final review based on a consensus. Additionally, the reference lists of these studies were used to identify further articles.
EXCLUSION CRITERIA
Studies that did not fulfill the eligibility criteria were not considered for the review. Specifically, studies that were not related to TD and its applications in dental public health services and studies that were focused on associated legal issues, available technologies, and the history of TD were excluded. Additionally, editorials, letters, comments, summaries of annals, essays, dossiers, official documents of national and international programs, reports of experiences, theses, dissertations, literature reviews, course articles, epidemiological bulletins, management reports, and books were also excluded.
DATA ITEMS AND DATA COLLECTION PROCESS
One of the author's (C.B.C.) collected the relevant data from the selected studies. The information was then crosschecked by the second and third reviewers (F.S.P. and A.L.S.F.M.). The data collected consisted of the names of the authors, year of publication, country, study design, context, and key findings (Table 2).
Results By Author, Year, Country, Study Design, Context, Key Findings, and Mixed Methods Appraisal Tool Score
ICT, information and communications technology; MMAT, Mixed Methods Appraisal Tool; OHT, oral health therapists; RACFs, residential aged care facilities; TD, teledentistry; VDH, virtual dental home.
QUALITY ASSESSMENT OF INCLUDED STUDIES AND DATA ANALYSIS
Due to the variety of research methods employed in the included studies, the Mixed Methods Appraisal Tool (MMAT) 13 was used to assess their quality (Table 2). The score for each article was calculated by dividing the number of met criteria by four. The calculated scores ranged from 25% (one criterion met) to 100% (four criteria met). 13
A constant comparison method was used to classify the extracted data into groups and subgroups based on themes. Undertaking this approach to perform the data analysis for an integrative review is compatible with researches that involve the use of a variety of data items and diverse methodologies not only in the case of qualitative studies but also of quantitative or mixed-method studies; this is because the approach allows for interactive comparisons across primary data sources. 14
To facilitate the analysis, data were extracted from the studies and organized into an evidence table (Microsoft Excel®). Following this, data were compared item by item, and similar data were grouped and categorized based on themes to answer the research question: How can TD be used in dental public health services? Additionally, relevant quotes from the articles' authors were selected to elucidate each category's content.
Results and Discussion
The initial search yielded 1,269 articles. After excluding the 298 duplicates, the titles and abstracts of the 971 remaining articles were screened. Most of the publications (832) were excluded because they were not related to TD and were presented in the formats of editorials, letters, comments, summaries of annals, essays, dossiers, official documents of national and international programs, theses, dissertations, course articles, epidemiological bulletins, management reports, and books. From the 139 articles whose full texts were assessed for eligibility, 115 articles were excluded because they were not related to public health, only described the history of TD and associated legal issues, or focused on available technologies. After the full-text review, 24 studies were included in the final review (Fig. 1). 15
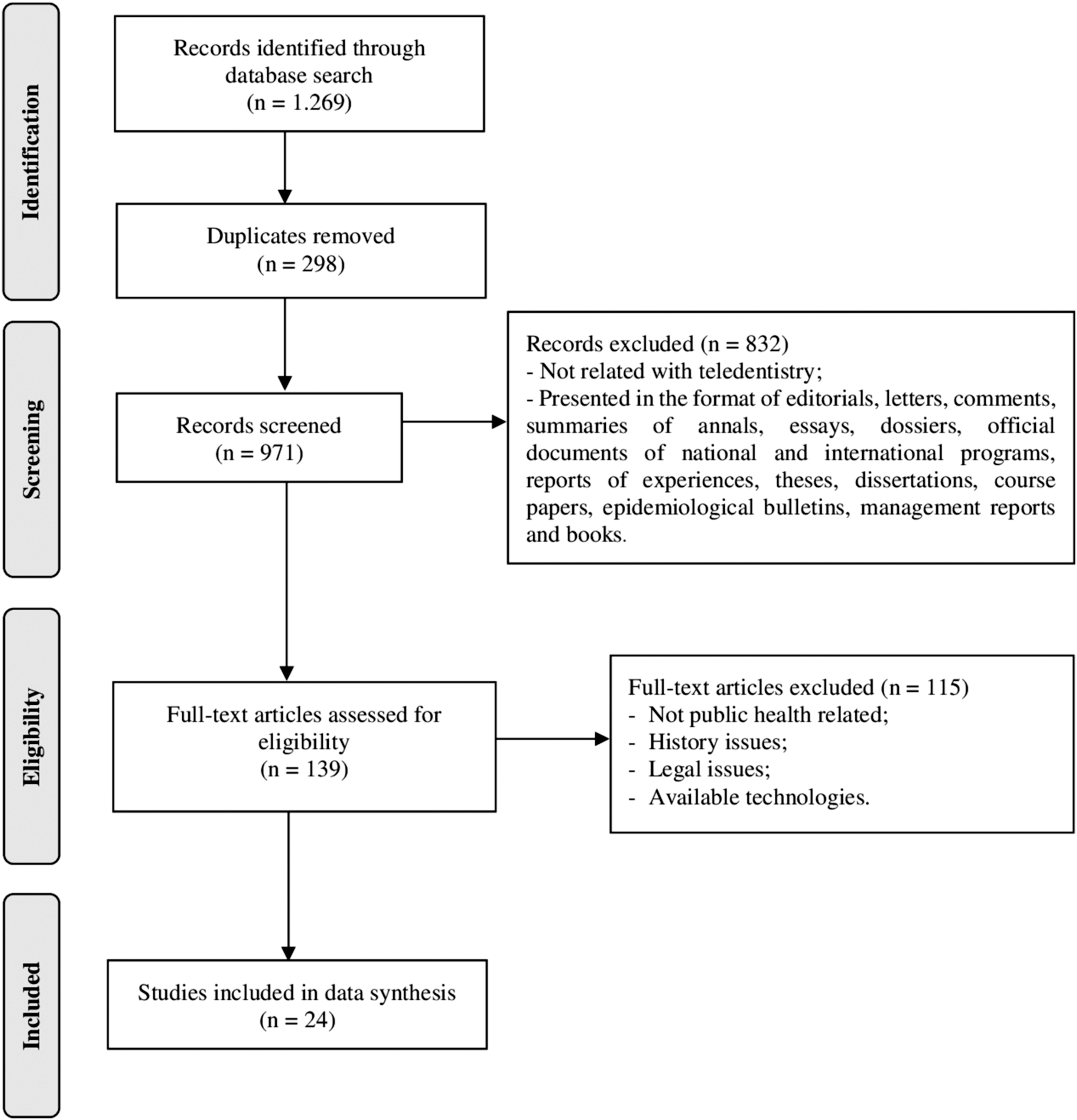
Flowchart adapted from PRISMA. 15
Among the 24 studies that met the eligibility criteria, 7 studies 16 –22 could not be assessed using MMAT because they did not have enough information regarding the methods and criteria that were employed; however, the remaining 17 studies 6 –8,23–36 were assessed by MMAT. Most of them (14 studies) had good-quality scores, meeting 3 or more of the 4 criteria. Furthermore, 3 studies were considered to have moderate-quality scores, meeting only 2 of the 4 criteria (Table 2).
The main findings outlined by the studies were arranged in terms of the issues faced in relation to the use of TD, its advantages, and the obstacles encountered in the application of TD (Table 3). Each of these is elaborated as follows:
Examples of “Quotes” for Data Analysis
A$, Australian dollar; CEA, cost-effectiveness analysis; CL&P, cleft lip and palate; OR, operating room; RCH, Royal Children's Hospital; SEK, Swedish krona.
APPLICATION
In dental public health services, TD is utilized in the field of education (tele-education) and to provide diagnoses and recommend treatments over long distances (teleassistance).
Tele-education and teleassistance can improve the knowledge of professionals to facilitate the early detection of oral diseases, such as caries, cancer, and periodontal disease. By providing remote diagnoses to perform the initial evaluation of a dental condition and to recommend a treatment plan, TD has the potential to help reduce morbidity and mortality through promoting preventive and health promotion practices. It also gives patients the ability to follow up with their dentists online. 6,8,17,18,22,24 –26,29,32,34,37 –39
Latin American countries, such as Brazil, Colombia, and Uruguay, are developing ICT projects as part of dental public health services to improve the continuing education and collaborative research efforts between national and foreign institutions. 31 In Brazil, TD is also used to exchange information among universities and primary health care dentists, thereby adding value to innovative actions taken by professionals and improving the quality of oral health care in this country. 21,24,27
In the developed countries that have been using this technology for a longer time, responses to tele-education projects 19 reveal that this powerful approach was accepted by 80% of students and professors 40 despite some technical problems that may occur during transmission. 19,40
Distance and online courses can improve the knowledge of professionals that is required for the detection of diseases, such as oral cancer, dental caries, and periodontal disease, thereby helping to reduce the occurrence of these diseases by recommending preventive practices and promoting good health in association with the remote diagnosis and its initial investigation. 27,32,39 –43
The applicability of TD has been demonstrated in a wide range of dental patient groups, including pediatric, 25,29 orthodontic, 35 and elderly 26,28 patients, as well as prisoners. 17 It also has potential utility in complex forms of treatment (e.g., long-term management of cleft lip and palate) involving multidisciplinary teams.
BENEFITS
TD is an instrument of democratization, equity, and development, which enables the dynamic dissemination of knowledge in the dental public health field through using its applications such as tele-education and teleassistance. 19,24,25,27,32 The main advantages are related to reducing waiting time, 36 and treatment costs. 6,8,20,23,25
Teleassistance is an innovative method of delivering health services that has the potential to facilitate the timely distribution of information to locally based practitioners to enable better decision making, to provide consulting services in case a second opinion is required, to effectively triage patients who require referrals, and to support locally based treatment centers. 6,41 Most dental practitioners and patients have reported on experiencing optimism and satisfaction regarding TD and its integration into the current dental practices due to the resulting possibilities of saving time and of gaining quicker access to medical case and a recommended treatment plan. 7,22,24
TD systems may be useful in the management of patients with conditions, such as oral mucosal disease (stomatology and oral medicine), 8,22,24,34 periodontitis, 8 malocclusions, orthodontics disorders, 35,36 temporomandibular disorders, and oral pain. 22 It is a low-cost system that enables remote dental examinations when an oral medicine ward is not available, 20,24 especially to assist primary care professionals. 24,27 It allows for an easy access to efficient consultations. Furthermore, it enables the underserved population to seek treatment earlier, which in turn minimizes the burdens faced by the patients who would have to travel long distances to receive a consultation. 6,24,26,28,29
The results of experiments carried out in countries that employed this technique, demonstrated a reduction in costs by ∼30% when compared with those of conventional treatments. The estimated savings were owing to the low salaries received by dental therapists and the travel and accommodation costs avoided by both patients and professionals. 6,8 Time and financial resources saved by TD applications can be redirected to patient populations at higher risks of oral disease. In a context in which limited resources for dental services exist, TD can be a major contributory factor toward the reduction of oral health inequalities 25 by reorienting public health services.
OBSTACLES
In the field of teleassistance, low levels of motivation and the lack of compliance are important obstacles that need to be overcome. 32 Most postgraduates believe that TD has limited application in the case of dental emergencies. 33 Moreover, professionals who are not well versed in the resources of technology may be more resistant when it comes to adopting their use. A substantial number of professionals felt insecure about their information technology skills. 36 Adequate levels of knowledge and awareness regarding TD and a good working relationship among the professionals at both the transmitting and receiving sites is required to establish a reliable network of TD application. 22,33
According to each country's legislation, there are some limitations and legal issues to take into consideration, including licensure, jurisdiction, malpractice, and information security-related issues. 18 Furthermore, a good infrastructure is necessary to meet all the technological requirements needed to provide adequate services and to ensure security in relation to the exchange of patient data. 18,22,35
Some authors have criticized the use of TD as a strategy to increase access to health services, and have suggested that it would offer little benefit when compared with conventional screening and prevention programs performed by dental hygienists in the public service. 16 A significant challenge is the ability of nonoral health professionals (e.g., nursing personnel) to accurately perform evaluations of oral disease. Indeed, a recent study carried out among prisoners to determine the need for emergency dental treatment reported that 63% of diagnoses made by nursing personnel were incorrect. 17
Despite these issues, the interest in TD in the past 2 years has grown substantially, as is evident from the increased number of published articles from 2017 to 2019 (Table 2). The literature search conducted in this study documented only 14 published articles relating to the use of TD in public health services over a period of 10 years (2007–2017), compared with 10 studies in the last 2 years.
Conclusions
In conclusion, TD may be a very useful tool for dental public health professionals, caregivers, and patients. Although it has been in use only since recent times, it presents a great potential for further development.
TD can be used for training and continuing education of professionals, for remote patient care, to exchange information among health professionals, and to provide them with orientations. It results in benefits such as the reduction of waiting time in the case of both general and specialized dental care, avoiding expenses related to displacements, and saving financial resources. In this way, it increases the access to dental care for people who live in remote areas or who do not have specialists in their location. It enables general practitioners to interact with colleagues from different dental specialties, thereby increasing the quality of the care provided and improving patient satisfaction.
TD is a relatively new modality for the delivery of dental health services and has a tremendous potential for continued growth and expansion in the context of public health systems. To achieve this goal, significant governmental support is required, and strategic action plans are needed, which not only increase the technological resources available, but also the acceptance of ICT among the general patient population, caregivers, and health professionals. Additionally, increased training and continuing professional development for ICT use is required for general dental surgeons, specialists, dental auxiliaries, nurses, and others health professionals who deal with oral health issues. Moreover, to facilitate the adoption of TD in public dental services, these strategic actions must form an integral part of the public health policy agenda, which advocates TD as an evidence-based and cost-effective method for improving oral health.
Limitations in this integrative review relate to the search strategy, which only targeted TD applications used in public dental health services in a community context, over a restrictive time period. In addition, only articles published in one of the three languages were included in the review. Furthermore, limited evidence was available for formulating definitive conclusions with regard to the superiority of one type of TD application versus another for fulfilling public health needs. Additional studies, preferably clinical trials, are required to inform stakeholder decisions in the selection of the best evidence-based TD applications for dental public health.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.