
Abstract
Aim:
To investigate whether there is a correlation between age and satisfaction with the use of videoconferences (VCs) and whether the number of video sessions had an impact on satisfaction.
Methods:
This study was a subanalysis of the joint European project, MasterMind, and participants were recruited from15 pilot studies in 11 different countries. The Client Satisfaction Questionnaire 8 (CSQ 8) was used as assessment tool, and scores were summed to give total scores.
Results:
Participants were included if they had filled out the CSQ 8 questionnaire and demographic data were available. This resulted in a total of 199 participants. We found that the total score was not significantly correlated with age (Spearman's rho = −0.0415, p = 0.563) and gender (Wilcoxon W = 5,066, p = 0.409). There was a significant positive correlation between number of sessions attended (Spearman's rho = 0.5777, p < 0.001) and total score after adjusting for age, gender, region, symptoms score, and education level in a multiple linear regression model (coefficient = 0.170, SE = 0.059, p = 0.004). Excluded responders were significantly younger than included responders, had lower symptoms score, attended fewer sessions, had a higher education, and were more likely to be employed.
Conclusions:
VC satisfaction scores in patients with unipolar depression do not depend on age but increase with experience in all age groups.
Introduction
Satisfaction with the use of videoconferences (VCs) has been investigated in a number of studies in heterogeneous populations with different diagnoses and a wide age range. 1 –3 Depression in older adults is a major challenge. The prevalence of depression in this group varies between 10% and 20% all over the world, and depression is predicted to be the leading cause of disease burden among older people in 2020. 4,5 Although effective treatment exists, treatment rates remain low, with a treatment rate of 56% reported for 2010. 6 A number of challenges prevent older adults from getting treatment. 7,8 Great distances to treatment centers, immobility, and negative attitudes such as stigma and shame may lead people to deny symptoms and delay treatment, especially older adults. 6 –8 These challenges make it relevant to consider innovative approaches such as VCs for delivering mental health service to older adults by providing an option for increased access to evidence-based care at a distance. 3,8,9
There is an increased interest in the use of telemedicine solutions in health care. VCs play an important role in telemedicine initiatives 10 and have been widely used for more than half a century. 3 VCs are a viable option in the delivery of psychiatric care, 11,12 and there is evidence that VCs produce the same results as face-to-face (FTF) treatment of depressed patients. 13 Despite potential benefits, there are still challenges to their widespread use. 3 In general, there seems to be barriers 14 and a large gap between the research evidence and the use of telepsychiatry in routine health care. 3 Progression of telemedicine services from “trial” status to routine health services must be supported by improved research into patients' satisfaction with telemedicine, 2 adequate satisfaction being a prerequisite for implementation. 9
Older patients, in general, do not embrace change, 1 but some recent studies have identified a generational acceptance of technology and e-health 1 even in older people and patients with chronic conditions. 15,16 Despite older populations tending to be less comfortable with technology than younger people, telemedicine receives positive satisfaction scores in some studies, perhaps because of the ease of access to medical care. 16 However, other studies find that patients aged 20 through 49 years had much higher acceptance rates than those younger than 20 or older than 49 years. 17 Studies also show improvement in satisfaction as the number of telehomecare interventions increases, 18 especially older patients tended to report increased comfort with the sessions over time 17 but studies in this area are sparse.
Acceptability and appropriateness refer to the perception among patients that the treatment is satisfactory and perceived fit to address the mental disorder. 19 By comparing satisfaction scores between older and younger patients, research may help to identify whether VCs may be an option for a patient group not accustomed to modern electronic technology. More factors determine patient satisfaction, including type of disorder, 3 and none of the existing studies focused on depression and whether satisfaction score depends on age. Another interesting focus area where research is sparse 17 is the question of whether experience gives higher satisfaction scores. Knowledge within this area would be especially valuable with regard to future use in clinical practice and the planning of VC implementation strategies. Several methodological limitations characterize existing studies in the use of VCs and more studies are needed for which patients and type of disorder VCs are most suitable. 2,3,20 The aim of this study was to investigate whether there is a correlation between age and satisfaction with the use of VCs and whether the number of video sessions has an impact on satisfaction. This study is based on data from MasterMind, a large scale joint European multisite project. 21
Methods
Design and Participants
This study is a subanalysis of the MasterMind project. MasterMind is a multilevel and mixed method project using a process and pretest–post-test study design. Participants in the project were recruited from 15 pilot studies in 11 different countries 22 and were included from 2013 to 2017. MasterMind was designed to make high-quality treatment for depression more widely available for adults through the use of communication technology. The goal was to assess the impact of computerized cognitive behavioral therapy (cCBT) and the use of videoconferencing facilitating collaborative care (ccVC) in the treatment of depression to identify barriers and success factors in different contexts to allow implementation on a large scale. 21 Inclusion criteria for the project were patients >18 years treated for mild-to-moderate depression. Participants were informed about the aim of the study, that anonymity would be preserved, and that they could withdraw from the study at any time. Verbal and written consent were obtained from each participant.
Ethics
Ethical approval for conducting the MasterMind study was obtained in each participating country in conformity with existing local clinical guidelines and legislation. Ethical standards and guidelines have been applied in line with the latest version of the Declaration of Helsinki and the relevant EU legislation on data protection. Sharing data between participating countries has conformed to the regulations of each host country. To protect information, all partners followed all the relevant advanced encryption standard procedures for personal password use and data encryption. Electronic data have been password protected and accessed by only authorized personnel. 22
Assessment of VCs
The evaluation was structured according to the validated model for assessment of telemedicine (MAST) 23 as described in the MasterMind protocol. 21 MAST was developed in 2009 for a multidisciplinary assessment of telemedicine applications. 23 Patient perspectives and satisfaction with the use of new technology are an integral part of MAST and data collection in the MasterMind study. The primary outcome of this study was satisfaction with the service among patients. The Client Satisfaction Questionnaire 8 (CSQ 8) is designed to measure general client satisfaction with services and consists of an eight-item self-report measure. Participants were asked to rate satisfaction on a 4-point scale, with a possible range of 8–32, with higher scores indicating greater satisfaction. 24 Internal consistency and construct validity have been established, and the measure is widely used in research. The CSQ 8 scale was administered at the end of treatment or on termination not later than 6 months after inclusion. The questionnaire was in the local language, and when no translation was available, local implementation teams translated the questionnaire by the forward–backward method. Demographic data, number of video sessions, and symptom score are obtained from all participants. 22
Intervention
This subanalysis is based on the ccVC part of MasterMind. CcVC refers to the technical infrastructure, security measures, procedures, guidelines, and competences needed to operate and utilize the VC technology for the benefit of patients with depressive disorders. 21 The intention was to improve collaborative care between health care professionals, to facilitate sharing of competence between health care workers, and to make access to treatment easier for patients in their own homes.
Based on the Cochrane definition of collaborative care, 25 the services were classified into four different interventions depending on their focus (Table 1). 22 In some pilot studies, several different solutions were implemented. Furthermore, it was possible to combine VCs with FTF treatment and to use VCs as a follow-up to cCBT. Hence the individual course of treatment and use of VCs including the number of video contacts differed among the participating centers. Only applications in which the patients participated or VCs were used as a follow-up to cCBT were included. The date of inclusion in the evaluation study was defined as the date the patient commenced treatment and termination was defined as the date treatment was completed and not later than 6 months after inclusion.
Description of Videoconferencing Facilitating Collaborative Care Interventions
cCBT, computerized cognitive behavioral therapy; GP, general practitioner; VC, videoconference.
Data Analysis
The CSQ 8 scores were summed to give the total scores, and nonparametric tests (Spearman's rho, Wilcoxon W, and Kruskal–Wallis) were used in the analysis. All analyses were done in R 3.5.1. Older patients were defined as patients >65 years.
Results
Data from 723 patients were uploaded in the MasterMind project. The procedure of including participants from MasterMind in this subanalysis can be seen in the flow diagram in Figure 1. Participants in this analysis were included if they had filled out the CSQ 8 questionnaire and demographic data (age, gender, education, occupation status, and sessions attended) were not missing from the data set. This resulted in 199 participants, and an overview of the demographic characteristics of the patients is given in Table 2.

Flow diagram of the patients from the MasterMind project included in this subanalysis.
An Overview of the Demographic Characteristics of the Patients Included in This Analysis
SD, standard deviation.
The CSQ 8 scores were summed to give the total scores, which were right skewed and not normally distributed (Shapiro–Wilk p < 0.001, Fig. 2). For this reason, nonparametric tests were used in the analysis.
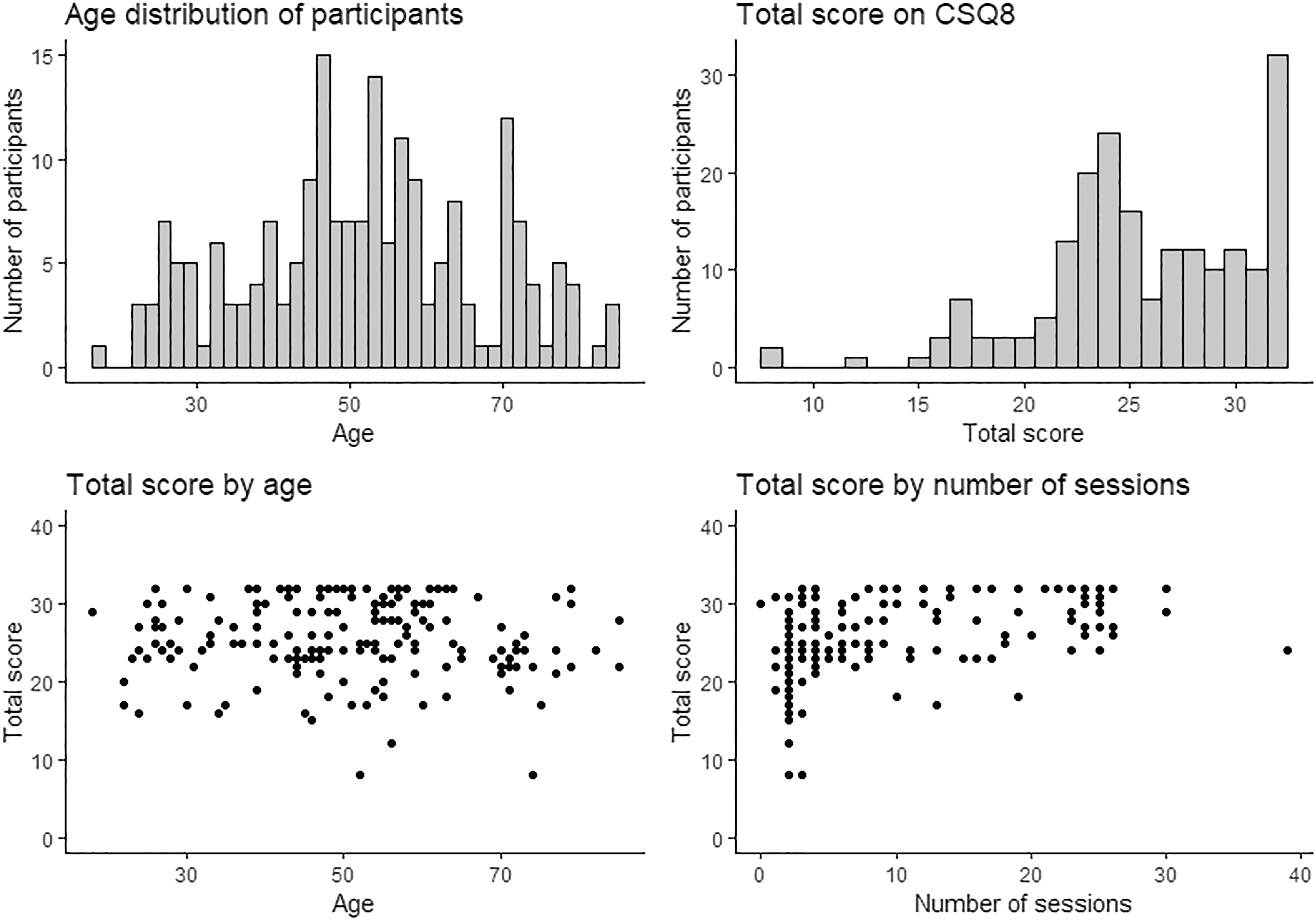
Histograms and point plots of participant scores and characteristics.
The results demonstrated that the total score was not significantly correlated with age (Spearman's rho = −0.0415, p = 0.563) and gender (Wilcoxon W = 5,066, p = 0.409). However, total scores varied significantly between regions (Kruskal–Wallis chi-squared = 53,203, df = 6, p < 0.001) as given in Table 3.
Mean Client Satisfaction Questionnaire Score for Each Region
95% CI, 95% confidence interval.
There was a significant positive correlation between number of sessions attended (Spearman's rho = 0.5777, p < 0.001) and total score. This correlation persisted after adjusting for age, gender, region, symptoms score, and education level in a multiple linear regression model (coefficient = 0.170, SE = 0.059, p = 0.004). The coefficients of the covariates were not significant at p < 0.05 with the exception of one region, Germany (coefficient = 2.98, SE = 1.39, p = 0.033).
Since demographic data were available for some of the participants excluded due to missing data, differences between included responders (n = 199) and excluded responders due to missing data (n = 255) were explored (Table 4). Patients excluded due to missing data were significantly younger than responders, had lower symptoms scores, attended fewer sessions, had a higher education, and were more likely to be employed ( Fig. 2).
Nonparticipants Analysis
Discussion
In this study, there was no significant difference in satisfaction score between older and younger patients. The results indicated that the total satisfaction score was not significantly correlated with age and gender, but scores varied significantly between regions. However, the results demonstrated that there was a significant positive correlation between number of sessions and total satisfaction score regardless of age, gender, and region.
Tools based on communication technologies are increasingly being used by both young and older persons. 11,26 –28 Age and gender are mentioned as the most important candidates as covariates that may contribute variance in satisfaction studies. 29 However, this study demonstrated that satisfaction with the use of VCs does not vary with age and that VCs can be used for health-related issues with equal satisfaction in different age groups. An interesting finding was that differences between regions could indicate that satisfaction may depend on how VCs are used in the treatment of depression. As given in Table 3, participants from Germany and The Netherlands score relatively higher than participants in the other countries. An explanation for this may be that VCs in these countries were used as follow-up and combined with cCBT.
The study also demonstrated that satisfaction increased with the number of sessions a patient took part in and that experience is of importance with respect to satisfaction. It cannot be ruled out that patients who were not satisfied dropped out of treatment with VCs, but the correlation between number of sessions and satisfaction score is also supported by other studies. 17 Other studies indicate that patients who had experienced 5–10 telepsychiatry sessions were more likely than patients who had experienced <5 telepsychiatry sessions. 17 The results of this study also show that satisfaction scores are lower for five sessions, Figure 2. In addition, older patients were more likely to report increased comfort with the sessions and technology over time than the younger patients. 17 When the number of sessions is related to satisfaction, one explanation could be that patients feel more secure when they become familiar with the use of VCs. Technical difficulties and lack of technological support are known barriers to the use of VCs. 3,9,20,30 Typically, the younger patients are more experienced and at ease with the use of technology, and older patients, in general, do not embrace change. 1,17 However, recent studies and our study have indicated acceptance of modern technology and e-health in general. 1,16,17
The results of this study and other studies focusing on older adults 1 do not indicate a difference between satisfaction score and age. The reason may be that VCs are often used in combination with FTF, and that it might differ from a situation in which VCs are used as a replacement for FTF care. However, this study indicates that VCs can be an alternative or a supplement to FTF treatment, also in older depressed patients. Other studies showed that especially older patients need to be introduced and supported in the use of the technical solutions. 28,31 Clients who actively engage in becoming familiar with the new technology overcome their initial reluctance because those who actually experienced the system had more positive feedback than a control group. 18 A strength of this study is that a clinically homogeneous patient population reported their satisfaction with this new technology, but it is important to keep in mind that the study was performed in a variety of settings and with different interventions. Being a multisite and implementation study that included multiple cases, this study is limited in a number of ways. In the interventions, patients received a combination of FTF and VCs. VCs may have been considered an “additional” service, 2 making it appear a more rapid option and that treatment would have been slower if VCs had not been used. The combination of FTF and VCs can make it difficult to distinguish the extent to which the satisfaction score is related to the actual treatment or use of the technology. As a consequence, caution must be exercised in generalizing our findings. 2 However, it is not possible to identify where use of VCs is best because different countries used different interventions.
Patient satisfaction may not always imply patient preference. 3 There was no control group, and an RCT study is required to compare satisfaction scores between FTF treatment and use of VCs owing to performance bias. An important consideration with regard to validity is to obtain high response rates to minimize selection bias. As a consequence, patient satisfaction data could be biased due to self-selection because those who are “less satisfied” are more likely to drop out. 2 This limitation is partly taken into account by comparing the demographic data in the included population with that in the missing data group. In this study, the nonparticipants were significantly younger than the responders, had lower symptoms scores, attended fewer sessions, had a higher education, and were more likely to be employed. There may be several explanations for this difference. The difficulty of getting to treatment centers may be greater in the younger patients, and patients who chose to use VCs may in general be more ill and need more contacts. Another explanation may be that that the younger patients do not opt out of video but drop out of treatment because they are less ill. However, when the reasons why the patients did not answer the questionnaire are unknown, it limits the generalizability of the findings.
CSQ 8 uses broad questions and is primarily intended to be used at a macrolevel. It tends to be less focused on specific features than multidimensional scales like SSS-30. 29 The scale provides a good overall measure of satisfaction at a macrolevel, but it is not designed to reveal the patients' experiences in detail and what they specifically liked or did not like regarding the use of VCs. Use of VCs is new to many users, and the newness of the experience could lead patients to provide positive answers because of the uniqueness of the encounter. 16
Future Research
There is a need for both quantitative and qualitative research regarding use of VCs. This includes RCT studies that take into account selection bias and qualitative studies that identify the reasons for the ratings. In general, studies around satisfaction need to be more focused on specific areas for identifying which type of consultation is suitable for the use of VCs for implementation on a larger scale. In this study, VCs were often used in combination with FTF treatment. Only a few studies have evaluated the significance of combining the two techniques. An important variable in telepsychiatry is the ability to establish a therapeutic alliance with patients through VCs. 3 Some studies concluded that relationship building appeared possible through VCs, but also that there could be difficulties associated with VCs, whereas other studies have reached different conclusions. 3 In one study, more patients chose inperson care for initial and follow-up appointments. 32 However, only a few studies have evaluated the significance of combining the two techniques. More studies investigating the combination of methods are needed to determine whether the combination of VCs and FTF treatment has an impact on therapeutic alliance, satisfaction, and clinical outcome.
Footnotes
Acknowledgments
The authors thank Edwin Stanton Spencer, MD, Associated Professor, for English review.
Disclosure Statement
L.F.C. collected data for MasterMind and M.M.S. was employed as scientific coordinator in the ccVC part of MasterMind. The other authors have not been associated with MasterMind and have no conflicts of interest to declare.
Funding Information
The authors thank The Psychiatric Research Fund in the Region of Southern Denmark, The MasterMind Project, Helsefonden (14-B-0156), Jascha Fonden, and Beckett Fonden for funding the study.