
Abstract
Background:
Telemedicine and point-of-care ultrasound have merged to create a field known as teleultrasound (TUS). Real-time TUS involves the transmission of bedside ultrasound (US) images with direct feedback from an US expert. In this review, we summarize the current uses of real-time TUS and discuss its potential future uses.
Methods:
We performed a literature search (PubMed and EMBase) to assess articles related to real-time TUS. Data were extracted using a standardized collection form, and relevant articles were separated into feasibility or clinical studies.
Results:
Our search yielded 45 articles, with most of the reports taking place in resource-constrained settings. A large portion of the studies discussed the use of the focused assessment with sonography in trauma exam. Others included musculoskeletal, vascular, and echocardiography.
Conclusion:
Real-time TUS allows for rapid access to diagnostic imaging in various clinical settings. This technology is poised to expand with many uses on the horizon.
Introduction
At the start of the 21st century, telemedicine and point-of-care ultrasound (POCUS) merged to create a field known as teleultrasound (TUS). TUS involves the transmission of ultrasound (US) images from one location to another for interpretation. Image transmission can occur synchronously, so that a nonexpert sonographer performing an US study on a patient can receive feedback in real time from an expert on how to optimize the images and interpret them. 1,2 Images can also be transmitted asynchronously, that is, a sonographer performs an US study and then transmits the images to an expert for review. 1,3 Although both forms of TUS expand access to expert consultation from various medical disciplines, little is known about its overall utility. The purpose of this review is to summarize the current uses of real-time TUS and discuss its future uses.
Methods
For this review, we searched the PubMed and Embase databases for all relevant studies published before September 1, 2018. For the PubMed database, we used the Mesh terms ((((“Telemedicine/utilization”[Mesh]) OR “Remote Consultation”[Mesh]) OR “Teleradiology”[Mesh] OR telemedicine[tiab])) AND (“Ultrasonography/utilization”[Mesh] OR ultrasound[tiab]). For the Embase database, we used the terms (“ultrasound”/exp AND “telemedicine”/exp).
Studies were deemed relevant to our systematic review if they met the following criteria: (1) described live TUS performed in patients older than 17 years, (2) did not involve the use of augmented reality or robotics, (3) conducted in a clinical medicine setting, and (4) were written in English. Studies that included patients younger than 17 years, that did not describe live TUS, that were used in obstetrics and gynecology settings, or that included augmented reality or robotics were excluded. The citations were reviewed for relevancy to this project by two of the authors; if they disagreed, the articles were discussed until consensus was reached.
The characteristics and results of the selected studies were reviewed, and data were extracted using a standardized data collection form. Studies were separated into feasibility or clinical studies and the following data were collected from each study: author, year of publication, original journal of publication, setting, and type of US examinations performed. The studies were deemed “clinical” if the study involved patients in a clinical setting and helped in medical decision-making. We were primarily interested in how live TUS is used in clinical practice and in which settings it is used.
Results
The flow diagram illustrates the selection process for our review (Fig. 1). The search terms identified a total of 431 articles, posters, abstracts, and reviews. The 35 duplicate entries were eliminated. We excluded 184 studies that did not involve live TUS on humans. We excluded 13 studies that were not in English, 25 that used robotics or augmented reality, and 46 that were abstracts, posters, reviews, or brief reports. We excluded another 63 studies pertaining to obstetrics and 20 pertaining to pediatrics. This culling left 45 studies for review. There were 33 feasibility studies and 12 clinical cases ( Tables 1 and 2 ).
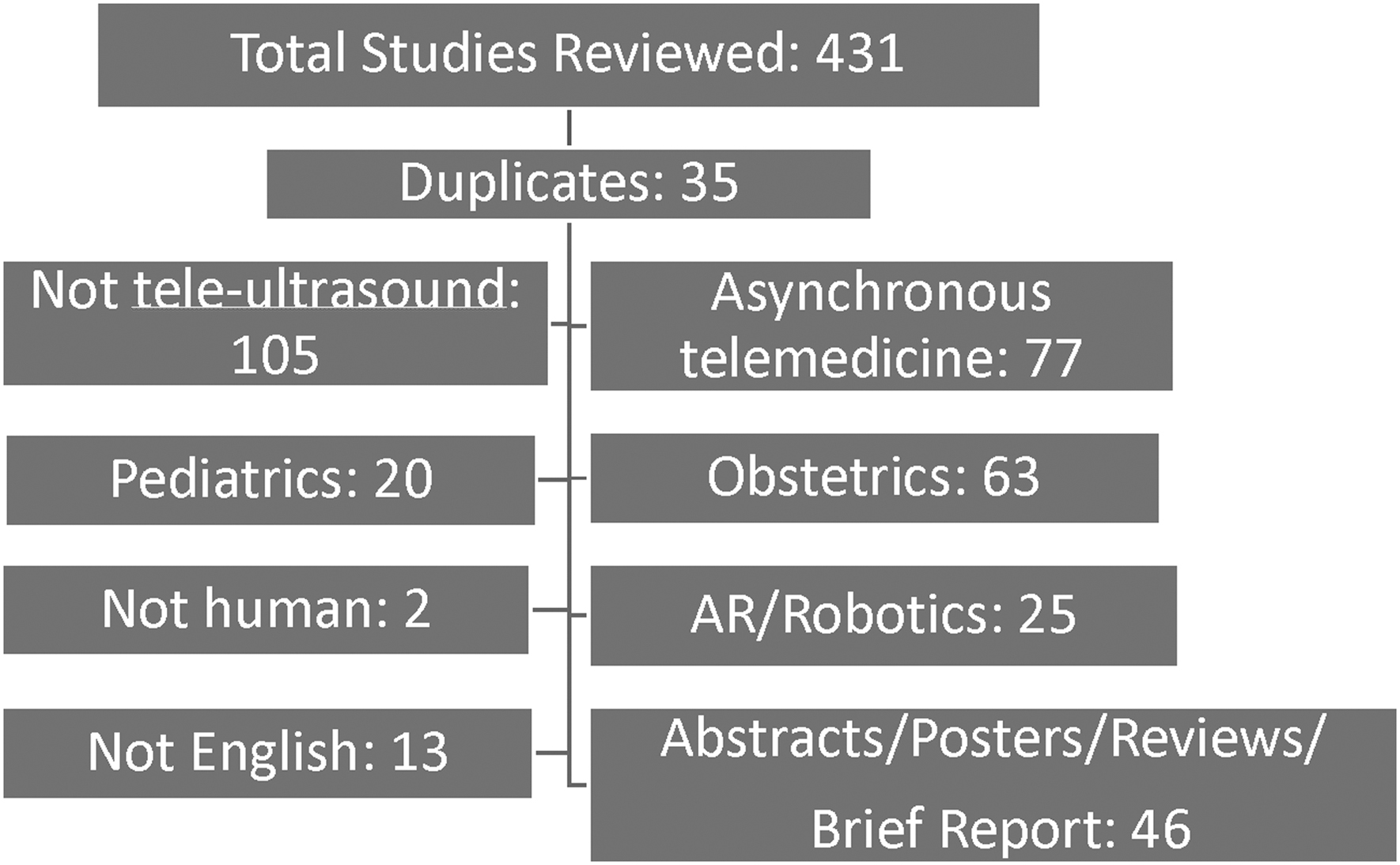
Systematic review of the articles identified and eliminated.
Feasibility Studies with Live Teleultrasound
Indicates same patients in study.
FAST, focused assessment with sonography in trauma; ICU, intensive care unit; MSK, musculoskeletal; US, ultrasound.
Clinical Studies with Live Teleultrasound
Indicates same patients in study.
FASH, Focused Assessment with Sonography for HIV-associated tuberculosis; HIV, human immunodeficiency virus.
Live TUS was used primarily at critical access points. It was also used in austere environments, such as in space and on mountain tops. One article described live TUS use at a sporting event. A large portion of the US examinations performed were focused assessment with sonography in trauma (FAST) and extended FAST (eFAST) examinations. Others were for cardiac, genitourinary, musculoskeletal, and transcranial/carotid Doppler assessments. Unfortunately, many of the studies did not report the total number of examinations performed or the total number of patients assessed; therefore, we were unable to further analyze these data sets.
Discussion
Current Clinical Uses
In resource-constrained settings, US may be one of the only imaging modalities available to patients, but health care providers in these settings might not have expertise in its use. 4 TUS attempts to address this challenge, but certain fundamental concepts underscore the successful implementation of a TUS system.
First, the necessary technology needs to be in place, including a platform from which to send the images to an expert. A comprehensive telemedicine system can be cost-prohibitive in resource-constrained settings. Therefore, some clinicians have attempted to find alternatives to traditional systems, such as using mobile computing devices. 4 In 2015, Levine et al. demonstrated that TUS images acquired by Philips VISICU monitoring software were of similar quality to those on the US machine itself. 2 The group then showed that images could be transmitted internationally through Apple FaceTime without degradation of quality. 3
TUS also requires a communication system. There needs to be someone at the bedside who can acquire images that can be interpreted accurately by an expert, who then reports back to local care providers. In 2017, Robertson et al. described how nonphysician health care workers can obtain images suitable for diagnosis with remote FaceTime guidance. 3 In this study, nine Haitian nonphysician health care workers received 20 min of training on basic US technique. Afterward, they performed lung, heart, bladder, and right internal jugular vein US studies with the remote guidance of an intensivist. An US-trained intensivist evaluated these images and found 89% of them suitable for making clinical decisions. 3 In 2018, Olivieri et al. demonstrated that nurses were able to perform examinations on critically ill patients through remote telementored guidance, yielding results similar to those of POCUS images obtained by critical care fellows. After brief training, the nurses felt comfortable incorporating US into teleintensive care unit (ICU) care. 5,6
Rural Hospitals and Clinics
The ability of the internet to connect geographically separated sonographers to expert consultants has facilitated the adoption of TUS in many low-resource areas. TUS in these settings is convenient for patients and decreases both the cost and, most importantly, the time to diagnosis. 7 –11 This prompt diagnostic access is especially important in settings where the nearest tertiary hospitals may be many hours away. Half of the studies in our review described the use of TUS in geographically isolated communities.
In the late 1990s, clinics in isolated settings, such as on the Greek island of Tilos, would perform US studies on patients, send the images to experts on the mainland, and receive information within hours. 12 Since the turn of the century, internet technology has greatly improved allowing many of these clinics to perform live TUS. For example, Otto et al. described the use of live TUS at an Antarctic base station with one US technologist, one emergency physician, and one internist. 13,14 Most of the time, they performed US studies and sent the images to a radiologist; however, the need for four time-critical evaluations over the course of their stay at the base station prompted the implementation of live TUS, allowing direct feedback from a radiologist. 14 One such study evaluated a patient with a pericardial effusion, in whom cardiac tamponade was a consideration. 13
In 2015, Kolbe et al. described the use of telemedicine in a rural village in Las Salinas, Nicaragua, where the closest major hospital was more than 7 h away by car. Local health care providers received expert training in the use of US for abdominal, cardiac, and lung evaluations and for vascular access, followed by 3 months of live remote guidance using a telecommunication system. Point-of-care TUS changed the management of 61% of patients (95% confidence interval, 52%–71%). 15
Specialty Clinics
As the capabilities of TUS expanded, it began to be used in specialty clinics to guide diagnostic decisions. In 2013, Janssen et al. described the use of TUS in a human immunodeficiency virus (HIV) clinic in Gabon. The local health care provider performed the Focused Assessment with Sonography for HIV-associated tuberculosis (FASH) examination with guidance from an infectious disease specialist in Germany. 16 The FASH protocol identifies pathologic body cavity effusions in patients with the HIV, which, in the right setting, are highly suggestive of extrapulmonary tuberculosis. 17 In this study, 10 patients were scanned for various reasons. The protocol supported the diagnosis of extrapulmonary tuberculosis in four of these patients. 16
In 2018, Carbone's group described the feasibility of using TUS to aid in the evaluation of 12 patients requiring a vascular US examination in a remote hospital in the Tuscan Apennines of Italy. 18 Expert clinicians were able to guide local clinicians through seven cerebro-afferent vessel studies and five arterial Doppler evaluations of the lower limbs.
Clinics have also performed transcranial and carotid Doppler US in the evaluation of stroke patients. 19,20 These tests screen for major steno-occlusive disease and their results can influence clinical decisions. We found two studies that discussed the feasibility of teleneurosonography. Both found that complete examinations could be performed with low-cost equipment. 19,20 In the future, teleneurosonography may be used to monitor patients in institutions without access to around-the-clock expert sonographers. 20
Intensive Care Unit
Because of a shortage in the intensivist workforce, TUS has found a role in ICUs. We found four articles that describe the use of TUS in the ICU setting. Previously, we discussed studies that laid the scientific foundation for widespread adoption of TUS in various settings, including the ICU. Pilot data from the Robertson et al. and Levine et al. studies suggested that images obtained by US-naive nonphysicians are of adequate quality for accurate interpretation. 3,4 Olivieri et al. demonstrated concordance between telementored US results and POCUS, as well as standard transthoracic echocardiography or computed tomography results. 5 In 2017, Becker et al. published representative actual clinical case scenarios involving four patients for whom live TUS allowed diagnosis and led to changes in management. 21 The teleintensivist was able to assess fluid responsiveness on cardiac examination and diagnose pulmonary edema based on the presence of B-lines. In addition, a malpositioned urinary catheter was identified as causing bladder distention. 21
Austere Environments
Many of the early reports of live TUS discussed its use by astronauts aboard the International Space Station (ISS) or at NASA training facilities. 22 Astronauts have performed both emergent and screening US examinations on the eye, spine, breast, and genitourinary tract as well as FAST with remote guidance from specialists. 23 –27 In our review, 11% of the articles addressing TUS were performed on the ISS or at a NASA training facility.
In 2014, Marshburn et al. described the first US screening of the cervical and lumbar spine performed in the ISS using a POCUS protocol. 25 Previous reports had documented crew members' experience of back pain during and after flights, caused by spinal changes induced by weak gravity forces in space. Marshburn's group collected high-quality US images with telemedicine guidance, which were used to quantify and characterize spinal changes and attempt to find solutions to counter them. 25
Other studies discussed the feasibility of telemedicine during space missions. For example, in 2010, Otto's group described TUS training on Devon Island, simulating the environment on Mars. 28 In this simulation, telementored US was performed on a woman's lower abdomen, allowing visualization of her ovaries, uterus, and appendix. The team also simulated a telementored laparoscopic appendectomy. 28
Wilderness medicine groups have also adopted TUS for use in low-resource areas. Our review revealed four feasibility articles that describe the use of live TUS in the wilderness. In 2009, Otto et al. described the use of US by nonexpert operators to detect signs of high-altitude pulmonary edema while climbing Mt. Everest. 29 The operators received audio and video assistance from experts at the base station. The study showed the feasibility of using TUS equipment at such high altitudes as experts could identify B-lines and signs of lung sliding without difficulty. In 2011, McBeth et al. also described the use of TUS in the mountains of Canada and Italy. A surgical resident and an intensive care nurse performed FAST and eFAST on a healthy individual and received direct feedback from an expert located miles away. 30
Fast Examination
By far the most common examination performed with TUS is the FAST/eFAST. The FAST was performed in 11 of the 45 studies in this review. It was used in various settings, including prehospital, wilderness locations, and critical-access-point hospitals.
In 2009, Al-Kadi et al. described the use of the FAST and eFAST at a remote Canadian hospital located near a national park. 31 Twenty of the examinations were performed during trauma activations. With the help of direct TUS mentoring, the resuscitation leader delegated responsibility for the US examination to a trainee, facilitating a more rapid evaluation of the trauma patient.
Ten percent of the articles in our review described the feasibility of prehospital care providers performing the FAST examination with TUS guidance. In 2011, Boniface et al. had 51 paramedics perform a FAST examination on a model patient with remote direction from an experienced emergency physician. 32 All of the paramedics completed the FAST with adequate images in <5 min. 32 In 2013, Song et al. described experimentation with TUS in the back of ambulances in Korea. 33 An emergency medicine technician obtained the US images and transmitted them to an emergency physician at a hospital. The study confirmed the diagnostic accuracy of the emergency physician's image interpretation at varying distances from the hospital and while the ambulance was in transit. 33 In 2013, McBeth et al. discussed the use of the FAST by emergency medicine technicians, members of a ski patrol, and nurses on a healthy volunteer and a US phantom. 34 Expert reviewers deemed 82.7% of the views of the healthy volunteer's Morrison's pouch to be adequate for diagnosis and 95 of 98 positive Morrison's pouch views on the phantom to be adequate for diagnosis. In 2016, Kirkpatrick et al. described the use of the FAST examination by 101 US-naive firefighters on a US phantom with remote guidance from trauma surgeons, intensivists, and emergency physicians in Alberta, Tennessee, and British Columbia. 35 The group achieved 97% accuracy in predicting free fluid.
Musculoskeletal
TUS is also helping clinicians on sports fields and with remote follow-up of patients with musculoskeletal injuries. Our review identified two articles that discuss the use of live TUS in musculoskeletal examinations. In 2007, Kwon et al. discussed the use of live TUS during hockey games. 36 Athletes underwent groin, knee, ankle, elbow, and shoulder US examinations to look for signs of injury. All of the real-time US video streams and still image captures could be interpreted by a remote expert. In 2013, Kirkpatrick et al. described a patient aboard a mission ship in West Africa. 37 With remote US guidance, physicians were able to diagnosis and follow up on the patient's torn adductor muscle.
Future Uses
TUS is a burgeoning field rife with possibility. Access to this technology is poised to expand with improvements in portability, increased storage capacity, enhanced resolution, lower bandwidth requirements for data transfer, and decreasing costs. Given that novices can obtain basic echocardiograms under remote expert supervision using a 4G network and a video chat application on a mobile phone, 38 it is not inconceivable that laypersons will eventually learn to acquire US images.
On the Horizon
In the prehospital and military environments, first responders face the challenge of making time-sensitive diagnoses and implementing therapeutic interventions. The performance of FAST examinations and thoracic US by physicians and nonphysicians during helicopter transport has been demonstrated as feasible. 39 –42 The next step is the application of TUS to connect transport teams with US experts. Due to the limited supply of medical instructors and the high rate of personnel turnover in Special Operations forces, TUS may assist with telesupervision and remote teaching. 43
Other potential areas of exploration include TUS use aboard moving planes and ships. For example, cruise ships are often hours from the nearest shoreline. TUS could help the cruise physician in diagnosing and triaging patients. Similarly, with the spread of internet connectivity on commercial flights, TUS will likely become an adjunct during commercial in-flight emergencies.
Since US has become more portable, you may also see a rise in its use within large national parks or with large organized outdoor experiences. For example, if a climber were to fall, medical staff could assess for signs of pneumothorax, internal bleeding, or even long bone fracture to activate the appropriate treatment teams and transportation earlier.
With the growth in telemedicine services for long-term care facilities, TUS is likely to have a role in mitigating costs and improving access to care. As previously described, nonphysician novices can perform basic US examinations under real-time guidance. 4 It is reasonable to expect that this capability could extend to nursing homes and home care settings.
The advent of telerobotics suggests interesting innovations in the applications of TUS. By using of a teleoperated robotic arm attached to a probe, a remote sonographer with a joystick has performed prenatal and general abdominal examinations. 44,45 In fact, autonomous imaging, in which a controller and tracking system orient a mechanical arm and probe in space, is being done for breast US. 46 With the continued evolution of artificial intelligence (AI), novices and even machines will eventually be able to acquire diagnostic information independently and remotely from experts.
Some of the most exciting prospects for TUS lie in the realm of AI and machine learning. With the growth of big data and expansion of computing power, AI continues to gain traction in medical fields that are based on visual interpretation, such as radiology and dermatology, 47,48 and computer-assisted interpretation of US images will likely become the norm. With expanding access to health technology and increasing portability of POCUS machines, a time will come when the limiting factor to using POCUS in austere environments will be the availability of expert image interpretation. Current barriers to this advance include the following: the need for a large, shared data set of images to be analyzed; secure, protected cloud storage of health information; quality assurance responsibility; a billing model; and medicolegal protection. Nevertheless, patients themselves, in a way similar to how they currently utilize a home glucometer, may eventually follow the automated stepwise guidance of an US machine to scan their own bodies, acquire images, and receive medical guidance from a remote expert.
Limitations
A large portion of the studies in the review were feasibility trials (73%). These studies lay the foundation for future studies. There are no large standardized trials that show the efficacy of TUS. Also, the results of the feasibility studies may be biased as most of the studies are not experimental data but rather statements from participants or authors that the study was successful. As TUS becomes more widespread, it would be important to see the results of large patient studies and to evaluate the usefulness of TUS with higher level evidence such as experimental control studies.
Conclusions
TUS is useful for performing a wide range of US examinations, with little to no prior experience needed by the individual scanning the patient, especially if the image is acquired under the direction of one trained in obtaining US images. With the inevitable growth of TUS, rapid access to diagnostic imaging is likely to expand to all levels of health care across the world.
Footnotes
Acknowledgment
The article was copyedited by Linda J. Kesselring, MS, ELS.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.