
Abstract
Background:
With increasing demand for neurologists, nontraditional health care delivery mechanisms have been developed to leverage this limited resource.
Introduction:
Telemedicine has emerged as an effective digital solution. Over the past three decades, telemedicine use has steadily grown; however, neurologists often learn on the job, rather than as part of their medical training. The current literature regarding telestroke training during neurology training is sparse, focusing on cerebrovascular fellowship curricula. We sought to enhance telestroke training in our neurology residency by incorporating real-life application.
Materials and Methods:
We implemented a formal educational model for neurology residents to use telemedicine for remote acquisition of the National Institutes of Health Stroke Scale (NIHSS) for patients with suspected acute ischemic stroke (AIS) before arrival at our comprehensive stroke center. This three-phase educational model involved multidisciplinary classroom didactics, simulation exercises, and real-world experience. Training and feedback were provided by neurologists experienced in telemedicine.
Results:
All residents completed formal training in telemedicine prehospital NIHSS acquisition and had the opportunity to participate in additional simulation exercises. Currently, residents are gaining additional experience by performing prehospital NIHSS acquisition for patients in whom AIS is suspected. Our preliminary data indicate that resident video encounters average 10.6 min in duration, thus saving time once patients arrive at our hospital.
Discussion:
To our knowledge, this is the first report of a telestroke-integrated neurology residency program in a comprehensive stroke center resulting in shortened time to treatment in patients with suspected AIS.
Conclusions:
We present a model that can be adopted by other neurology residency programs as it provides real-world telemedicine training critical to future neurologists.
Introduction
“Time is brain” is the mantra for acute ischemic stroke (AIS) treatment, which may consist of administering intravenous (IV) alteplase or endovascular intervention (i.e., mechanical thrombectomy or arterial stenting). The urgency of treatment is based on the estimate that 1.9 million neurons die every minute during an AIS 1 and that shorter time to treatment is associated with better functional outcome. 2,3 Current stroke guidelines recommend a door-to-needle (DTN) time of 60 min or less. 4
Stroke centers around the globe have implemented a variety of modifications to their acute stroke protocols to decrease treatment times with both IV alteplase and endovascular intervention. These modifications range from enhancing personnel notification systems at the treating stroke center 5 to equipping ambulances with computed tomography scanners to allow for radiographic evaluation en route to a stroke center. 6 Financial cost to institutions for implementing these changes varies. The high cost of modifications, such as mobile stroke units with onboard computed tomography scanners, has resulted in questions regarding their cost-effectiveness 7 and has prompted a search for methods that will maximize the quality of health care provided while minimizing monetary burden.
Telehealth is predicted to revolutionize health care and could save up to $300 billion in health care costs. 8 Numerous studies have demonstrated the benefit of telestroke, whereby most often, a neurologist accompanies an emergency department physician through synchronous, two-way video interaction to remotely quantify stroke deficits using the National Institutes of Health Stroke Scale (NIHSS); review pertinent historical, laboratory, and radiographic information; and provide guidance on the best course of treatment. Telestroke has been proven a safe and effective means of bedside evaluation for rapid diagnosis and treatment of AIS patients for IV alteplase administration 9 and has been associated with better functional outcomes for patients. 10 –14
We previously conducted a pilot study in which onboard telemedicine measurement of the NIHSS before a patient's arrival at the Mayo Clinic Emergency Department was feasible and saved, taking an average of 7.5 min. 15 There is a growing focus on resident education to improve the treatment efficiency of AIS, 16,17 and the success of our pilot study led us to make substantial modifications to our residency program. 18 We hypothesize that prehospital NIHSS measurement can be a valuable clinical skill taught to neurology residents and integrated into the existing standard of care brain attack stroke care model to reduce DTN and door-to-interventional radiology (DTIR) times. We expect this to be a cost-effective alternative to more elaborate ambulance modifications, such as onboard computed tomography scanners, while providing residents with a valuable opportunity to develop the critical skills of tomorrow's practicing neurologists.
Materials and Methods
We incorporated telestroke into our adult neurology residency program by providing residents with didactic, simulation, and real-life experiential learning components. By beginning formal training in telestroke earlier, we expect our residents to become more effective in conducting telemedicine acute stroke evaluations. This has been a multiyear implementation as our access to and quality of telestroke have improved. This study was approved by the Mayo Clinic Institutional Review Board.
Prehospital NIHSS Technology Implementation
The Mayo Clinic Center for Connected Care partnered with Century Ambulance Services (Jacksonville, FL) using RXpress® devices (InTouch Health, Santa Barbara, CA) installed in two critical care telemedicine-enabled ambulances for hospital-to-hospital transfers to assess the effects on DTN and DTIR times compared with historical controls treated during the 2 years before implementation (Fig. 1). To make the system continuously operational, all neurology residents (n = 12) were tasked with performing the initial NIHSS evaluation. A multidisciplinary team comprising attending vascular neurologists, neurology residents, and staff from the Mayo Clinic Center for Connected Care, Mayo Clinic Multidisciplinary Simulation Center, InTouch Health, and Century Ambulance Services implemented the three-phase educational model. The implementation model was repeated when Mayo Clinic expanded the service to three additional ambulance units, partnering with St. Johns County Fire Rescue, with 9-1-1 stroke in the field-to-hospital networks for those ambulances bringing patients with suspected AIS to our hospital by standard of care. This increased the total number of emergency medical services (EMS) telestroke-equipped units to 5.

Interior of Ambulance Equipped with the RXpress® System.
Three-Phase Educational Model
Phase I was a didactic briefing of the project rationale, including a workflow model (Fig. 2). Attendees included neurology residents, representatives from InTouch Health, Century Ambulance Services personnel, emergency department staff, and vascular neurologists who participated in the aforementioned pilot study. The multidisciplinary training enabled the group to discuss each step within the workflow. Potential obstacles were discussed and solutions developed. Phase I also included installation of InTouch Health telemedicine devices onboard the ambulances and onsite training for EMS staff before didactic training over 2 days at the Mayo Clinic Multidisciplinary Simulation Center. Phase I training was repeated with EMS personnel from St. Johns County Fire Rescue and Century Ambulance 2 months later, inviting the same neurology staff and residents, EMS staff, and Center for Connected Care stakeholders.
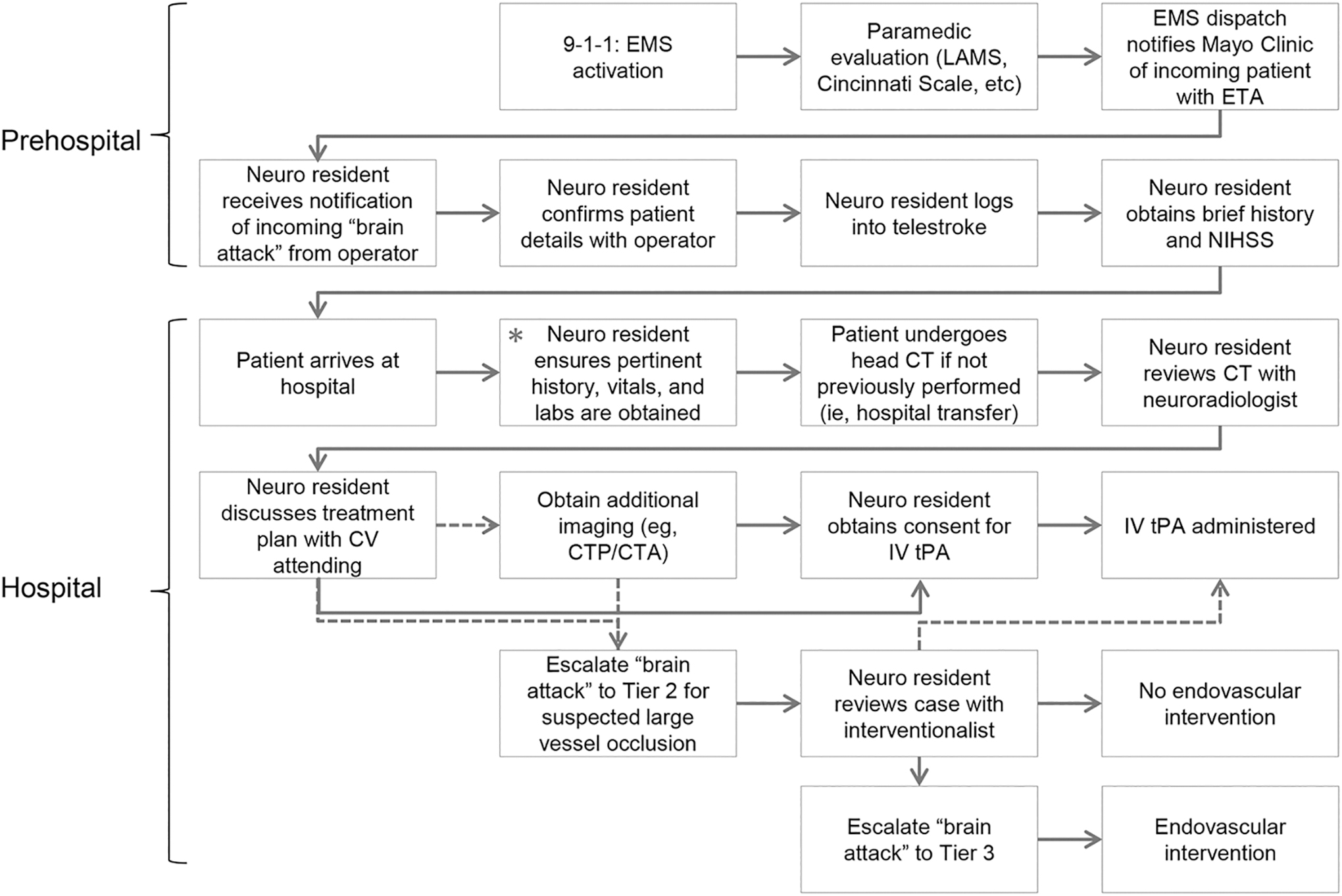
Prehospital NIHSS Acquisition Workflow. The prehospital phase begins with EMS activation and ends with the neurology resident conducting an NIHSS assessment, which was previously conducted during the first steps of the hospital phase, as indicated by the green asterisk. By moving the NIHSS acquisition from hospital to prehospital phase, door-to-needle and door-to-interventional radiology decreased. Dotted line indicates optional. CT, computed tomography; CTA, computed tomography angiogram; CTP, computed tomography perfusion; CV, cerebrovascular; EMS, emergency medical services; ETA, estimated time of arrival; IV, intravenous; LAMS, Los Angeles Motor Scale; Neuro, Neurology; NIHSS, National Institutes of Health Stroke Scale; tPA, tissue plasminogen activator.
Phase II included a live walking tour of the EMS ambulances equipped with the InTouch Health RXpress system. This provided trainees the opportunity to see the limited space in which paramedics work and the positioning of the two cameras from which the provider may view the patient. Residents and all other training staff were able to tour the ambulances to see the cabin space as would be seen during Phase III.
Phase III included a live stroke simulation in a moving ambulance with hands-on InTouch Health interface training for effective NIHSS evaluation in the telestroke environment (Fig. 3). Specifically, they developed methods to adjust the order of the NIHSS elements to minimize the number of transitions that emergency medical technicians must complete to maximize their safety in a moving ambulance. Residents also had the opportunity to learn strategies for efficient zoom–pan–tilt camera control, effective communication with EMS staff, and appreciation of nonorganic artifacts, such as shaking extremities when driving over uneven road surfaces.

Three-phase telestroke implementation model.
Measurement of Time Saved
After each resident successfully completed the three-phase education model, they were authorized to begin administering the NIHSS to live patients en route to the Mayo Clinic Emergency Department. The start and stop times of each video assessment were recorded to determine the duration of each prehospital evaluation, the average of which was defined as the amount of time saved from the evaluation after a patient arrived at our institution.
Results
Among the 12 neurology residents, 11 completed Phase I through III training in the Mayo Clinic Multidisciplinary Simulation Center. One resident was unable to attend these sessions because of on-call responsibility and Accreditation Council for Graduate Medical Education (ACGME) duty hours, but completed training separately with InTouch Health and the Center for Connected Care services' support at a later time. InTouch Health also provided access to a 24/7 online simulation laboratory for all residents to practice the features before a live patient encounter.
Preliminary Results of Prehospital NIHSS Acquisition
The primary aim of our project was to assess the feasibility of this educational approach. Live runs with patients who have suspected AIS began in August 2018 with two ambulances equipped with onboard telemedicine devices. Encounters were initially limited to hospital-to-hospital transfers, where patients who were already diagnosed with stroke (with or without administration of IV alteplase) were transferred to our institution for possible endovascular intervention. Bidirectional feedback from neurology residents and EMS providers was obtained for each encounter to continually improve workflow. Three months after implementation of telemedicine for hospital-to-hospital transfers, we expanded to three additional St. Johns Fire Rescue ambulances and demonstrated feasibility of evaluating patients brought directly from the field to our hospital. This model allowed earlier evaluation of NIHSS with the goal of decreasing DTN and DTIR times in patients who were brought to our hospital by EMS with concern for AIS, while maintaining our standard of care (Fig. 2). To date, we have had no technical issues (e.g., inadequate image or audio quality or loss of signal). Moreover, we have already recorded substantial improvements in time to treatment, with an average of 10.6 min calculated from the first 11 patient encounters (Table 1). Thus far, all of our patients have had neurologic emergencies due to diagnoses other than ischemic stroke. Therefore, DTN and DTIR times are not applicable. Due to variability in transportation time to our hospital, any remaining time after completion of the NIHSS has been used to obtain additional historical information that would otherwise be collected upon the patient's arrival, thus further streamlining the clinical evaluation.
Summary of 11 Prehospital Stroke Evaluations
F, female; F2H, field-to-hospital; H2H, hospital-to-hospital; ICH, intracerebral hemorrhage; M, male; NIHSS, National Institutes of Health Stroke Scale; SAH, subarachnoid hemorrhage.
Discussion
Health care costs associated with AIS are predicted to reach 1.5 trillion U.S. dollars by 2050, reflecting an aging and sicker U.S. population. 19 The Centers for Medicare and Medicaid Services project that health care spending will grow 1.0% faster than the gross domestic product and will represent 19.7% of the entire gross domestic product by 2026. 20 The demand for neurologists continues to increase, and the supply gap is expected to nearly double from 2012, reaching 3,380 by 2025. 21 These figures illustrate the unsustainable trajectory of health care access and expenditures, leading many institutions to implement alternative mechanisms into their health care models.
Telehealth has grown into a large and critical component of health care delivery. In 2017, the American Hospital Association reported that 65% of hospitals in the United States connect with patients and consulting practitioners through the use of video and other technology. 22 The applications of telemedicine are vast and range from a simple videoconference with a patient to conducting a thorough physical examination and administering treatments. Advances in digital examination instruments have the potential to improve the efficiency of patient encounters by enabling practitioners to acquire a greater quality and quantity of clinical information. For instance, stethoscopes capable of wirelessly transmitting audio with illustrative waveforms enable practitioners to conduct essential portions of the physical examination remotely. 23
Some may argue that telemedicine is an inadequate substitute for an in-person provider; however, the past 25 years have seen a growing presence of telehealth in neurology. Telestroke has several benefits, including better access to care for patients, greater efficiency in the delivery of health care, 24 and improved cost-effectiveness. 25,26 Given the national shortage of neurologists 15 and increasing demand for stroke services, telemedicine has been proposed as a potential solution to better balance supply and demand. 22 The benefits of telestroke led to the American Heart Association's recommendation that telemedicine should be implemented within stroke systems of care. 27 Successful implementation of acute stroke care through telestroke in rural areas and strong advocacy from the American Academy of Neurology led the U.S. Congress to pass the Furthering Access to Stroke Telemedicine Act, which expanded Medicare reimbursement of telestroke beyond just rural areas to all geographic regions. This expansion illustrates the growing presence of telestroke and underscores the need for adequate exposure and proper training of new neurologists as they enter the workforce.
Telestroke training has been proposed for the vascular stroke ACGME fellowship 28 as it would add to core competencies. To our knowledge, our model (Table 2) represents 29 the first telemedicine training in neurology residency to improve stroke systems of the care model in the Unites States, teaching future neurologists a critical telemedicine skill set that could be used for other applications in neurology. In our opinion, the biggest strength of this work is first-in-kind teaching telemedicine skills to neurology residents early in their training, as well as integrating this model into an ACGME-accredited neurology residency along with our vascular neurology fellowship and cerebrovascular neurology teaching faculty. One limitation of this project is the relatively small neurology residency of 4 residents per year of training for a total complement of 12 residents.
Components of Adult Neurology Telestroke Curriculum
AIS, acute ischemic stroke; NIHSS, National Institutes of Health Stroke Scale; PGY, postgraduate year.
The success of this initial implementation is, in part, due to the pre-existing, robust, vascular neurology clinical education within the Mayo Clinic College of Medicine and Science neurology residency program. Since 2008, Mayo Clinic neurology residents have had the opportunity to take part in observing telestroke encounters with cerebrovascular attending physicians during cerebrovascular elective rotations. In 2012, a Transitions to Neurology course was started for incoming neurology residents to develop foundational knowledge and skills before the start of their second postgraduate year. Traditionally, foundational subjects include neuroanatomy, neurologic examination, common consults, and neurologic emergencies. We have now expanded the Transitions to Neurology course to include formal telemedicine education. In 2016, a telestroke simulation was introduced at our simulation center to further develop telemedicine skills in a simulated environment. Equally as important as the technical skill of computer management in telemedicine is the concept of a good webside manner. This skill, similar to the bedside manner, can be evaluated using ACGME core competencies of professionalism and communication, with the goal of delivering the same high quality of care as in-person encounters. Additionally, it is important for trainees to gain an appreciation for many of the more subtle aspects of communication that may be blunted during telemedicine encounters, such as body language. 30 Neurology residents are monitored and critiqued using formal metrics to assess their technical proficiency, thoroughness of patient assessment, communication skills, professionalism, and time efficiency. We are now looking at future teleneurology models to incorporate into our curriculum to better prepare our residents for this evolving field. 31
Telemedicine for Trainees
As a result of telemedicine's growing role in health care, medical schools around the country have initiated exposure and training opportunities for students. In 2016, the American Medical Association urged that telemedicine training be included in medical school curricula. 32 The Association of American Medical Colleges reported that about 58% of medical schools included telemedicine training, in some form, during the 2016–2017 academic year. 33 Undoubtedly, the degree and quality of exposure vary widely from school to school; however, formal assessments are being developed to provide standardized metrics for evaluation of students.
While exposure and practice with telemedicine during medical school are valuable, formal training and experience in residency are arguably more necessary as residents can tailor this experience to their future careers. 34 Although in-person faculty teaching and supervision of trainees' management of neurologic emergencies such as stroke are preferred, they are not always practical. A survey at Mayo Clinic highlighted the valuable role of robotic telepresence in graduate medical education. 29 Another study demonstrated the usefulness of robotic telepresence for stroke alert team assessments. 29,35 Experience has been shown to be an important element in developing proficiency in telemedicine. One study found that neurovascular fellows took nearly 13 min longer during the evaluation and treatment of AIS than attending physicians, 36 but treatment times decreased for both neurovascular fellows and attending physicians by 1 min for every 14 telestroke consults run. 37 If structured practice is limited to only those at or above the fellowship level, then the time for worthwhile practice is short. We believe that residency is the ideal time for structured implementation and practice of telehealth because trainees have chosen a specialty and likely have a general idea of what their practice setting will look like and the role that telemedicine may play. In addition to opportunities for observation and simulation, we aim to provide residents with opportunities to gain actual experience given the known benefits of real-life practice. 36,37
In addition to the educational benefit to our trainees, incorporation of prehospital NIHSS acquisition decreases time to treatment. To date, no patients have had AISs, but have had other neurologic emergencies, including subarachnoid hemorrhage, intracerebral hemorrhage, or seizures. While treatment of these conditions does not include IV alteplase or endovascular intervention, they do require rapid assessment and treatment. Given that patients were transferred to our facility for suspected AIS, NIHSS evaluation was required. Acquiring this and other pertinent clinical data during an otherwise uneventful ambulance ride enabled earlier evaluation and administration of treatment. Data gathering is ongoing, but preliminary reports from 11 patients indicate that we are saving an average of 10.6 min in time to treatment for these neurologic emergencies. This time represents the total video encounter time, which includes acquisition of the NIHSS and, when transportation time remains, additional historical information on the patient. Because both of these elements are necessary to determine the best treatment approach, we believe that the duration of each video encounter represents time that would otherwise be spent after the patient arrives at the treating facility, thus increasing time to treatment. Because none of our patients have had a final diagnosis of ischemic stroke, metrics of DTN/DTIR times are not yet available; however, we anticipate a decrease in these treatment metrics compared with historic control cases of the preceding 2 years. This comparison will be necessary to demonstrate a true effect on outcomes.
The implementation of work-hour restrictions has made residents' time a precious commodity, and any additions to their duties must be optimized by minimizing disruptions 18 while maximizing improvements in the delivery of care. 16,17 We believe that our three-phase implementation model of telestroke training and practice of telestroke in the neurology residency program is a worthwhile investment, with the expected two-fold benefit of providing patients with better care and providing residents with high-quality high-yield training.
Conclusions
We report the first integration of telestroke training into a neurology residency at a comprehensive stroke center to shorten DTN and DTIR times for patients with suspected AIS. Using a three-phased educational model and a graduated increase in the number of telestroke-equipped ambulances in our area, we have been able to effectively train residents to adapt to this creative and nontraditional health care delivery model in a way that enhances patient care. Additionally, time to treatment for patients with AIS can be decreased with this model, as suggested by our preliminary data showing an average of 8 min saved in time to treatment. This integrated education model allows neurology residents contemporary telemedicine training early in their residency to better prepare them for the future of neurology.
Footnotes
Acknowledgments
The authors would like to thank David M. Strauss, Rochelle F. Putzier, Troy R. Delaney, Ronald Ferreira, Leslie V. Simon, R. Nicole Blegen, and Amy M. Lannen for their assistance in implementing the prehospital NIHSS system for residents and Dale M. Gamble and Elliot L. Dimberg for their guidance in developing/implementing elements of the teleneurology curriculum.
Disclaimer
Mayo Clinic does not endorse specific products or services included in this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.