
Abstract
Background:
Rapid on-site evaluation (ROSE) of image-guided fine-needle aspiration (IGFNA) of hepatic lesions is necessary to ensure adequate sample collection and render preliminary diagnosis. We review our experience with utilization of telecytopathology for ROSE of IGFNA of liver lesions.
Materials and Methods:
Cytotechnologists at a remote site transmitted real-time images of Diff-Quik-stained cytology smears of hepatic lesions obtained using an Olympus DP70 digital camera via Ethernet to a pathologist. All live communications were conducted using the Vocera voice communication system. Preliminary telecytopathology ROSE diagnosis was compared with the final diagnosis for accuracy.
Results:
ROSE using telecytopathology of IGFNAs of hepatic lesion was performed on a total of 178 cases. Preliminary diagnosis of unsatisfactory, benign, suspicious for malignancy, and positive for malignancy was 2%, 28%, 15%, and 55%, respectively, for telecytopathology. The overall concordance between the preliminary and final cytology diagnoses was 94.4%. Nine of the cases were upgraded to suspicious/malignant final diagnosis contributing to an upgrade rate of 5%. One case with preliminary evaluation of positive for malignancy was downgraded to benign cytology on final diagnosis resulting in a downgrade rate of 0.1%.
Conclusion:
Utilization of telecytopathology is highly effective and accurate for ROSE of IGFNAs of hepatic lesions and may serve as a substitute for conventional microscopy.
Introduction
Image-guided fine-needle aspiration (IGFNA) cytology of hepatic lesions serves as a decisive tool for arriving at a definite diagnosis. 1 Performance of liver aspiration under image guidance coupled with rapid on-site evaluation (ROSE) assessment by cytopathologists further improves the diagnostic accuracy and cost-effectiveness. 2,3 On-site assessment of samples allows for collection of diagnostic material for ancillary studies and provides immediate feedback for clinical management. 4 Despite the improved diagnostic yield with ROSE during IGFNA, staffing, significant time requirements, and inadequate compensation from a financial standpoint have restricted the availability of ROSE in every institution. 5
Dynamic telecytopathology systems transmit live video images to an interpreting cytopathologist in a remote location thereby circumventing the need for pathologists being on-site. 6 –8 The feasibility of dynamic telecytopathology for cytology specimens has been demonstrated using archived FNA smears. 9 –11 Prospective studies have reviewed the usefulness of dynamic telecytopathology for on-site assessment of FNAs of few body sites, for example, pancreas, thyroid, lung, axillary lymph nodes, head and neck, and mediastinum. 12 –21
We review our experience with telecytopathology-assisted ROSE of IGFNA of hepatic lesions over a period of 7 years and analyze the pitfalls and limitations that provide explanation for the discordance rate in challenging cases.
Materials and Methods
This study involved percutaneous IGFNA of hepatic lesions performed by an interventional radiologist at a radiology suite, with evaluation of slides performed by a cytopathologist located in a remote cytopathology laboratory located away from the ultrasound and CT suite of the hospital. A retrospective analysis of all Diff-Quik (Mercedes Medical, Sarasota, FL)-stained slides prepared on-site for telecytopathology-guided ROSE of IGFNAS was performed between January 2012 and March 2019 and was compared with the final cytology diagnosis that also included additional slides prepared using the Papanicolaou stain, cell block material, and ancillary techniques, for example, immunohistochemistry and flow cytometry.
Diagnostic cytology categories that were used for preliminary ROSE and final cytology diagnosis were as follows: Unsatisfactory: Cases with absent diagnostic features, including obscuring blood, crush artifact, cystic content, or debris. Benign: Cytological features characteristic of benign conditions, for example, benign hepatocytes, hepatic parenchyma with fatty change, regenerating nodule, hepatic parenchyma with bile ductular proliferation, cysts, abscess, sarcoidosis, and hemangiomas. Suspicious: Cases with cytological features suspicious for malignancy or cases with atypical cytological features where malignant neoplasm could not be excluded. Malignant: Cases with obvious cytologic features of malignancy.
The initial and final cytology interpretations for the majority of the telecytopathology and conventional cases were performed by the same cytopathologists.
Agreement between the preliminary and final cytology interpretations was considered concordant. Suspicious cases were considered concordant if the final diagnostic category was the same or malignant. Discordant cases were reviewed to assess the limitations and pitfalls contributing to the discrepancy. An evaluation upgrade was defined as any case with preliminary ROSE diagnosis of benign or unsatisfactory and a final cytology diagnosis of malignant. An evaluation downgrade resulted if any case with ROSE of suspicious or malignant had a final cytology diagnosis of benign. This study received Institutional Review Board exemption.
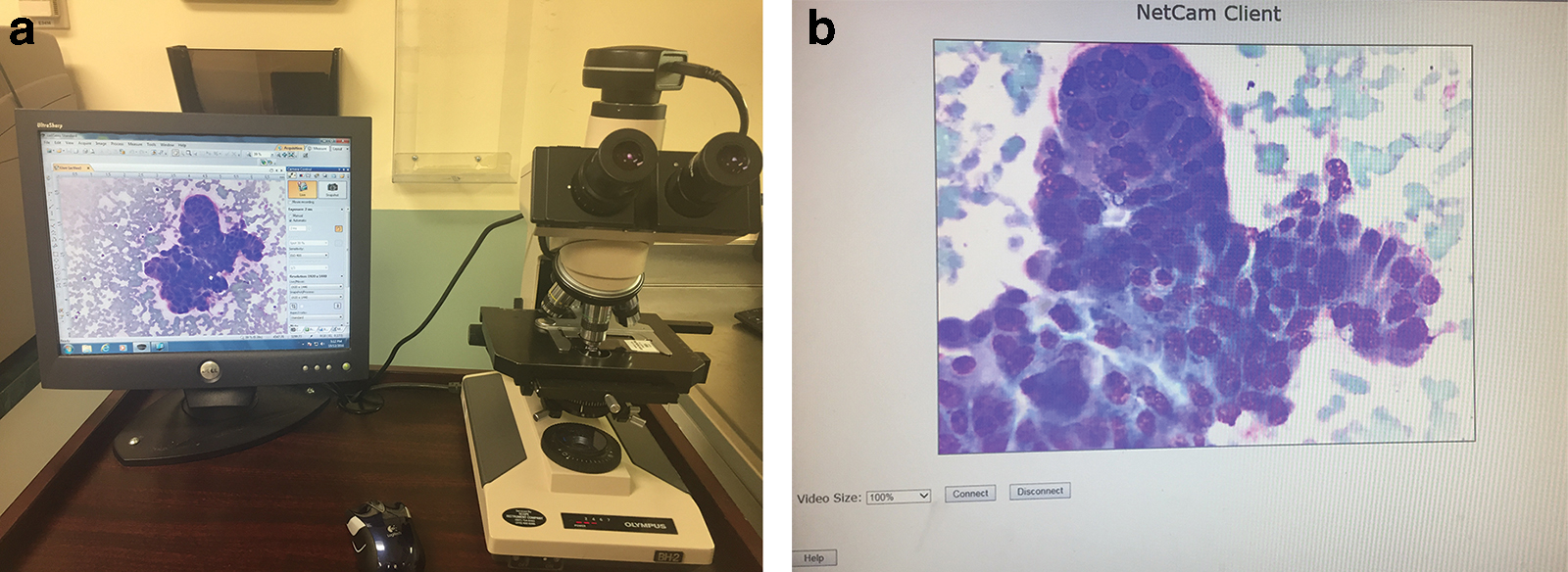
A detailed description of the telecytopathology system used in this study has been provided in other publications. 13,14,17,21 Briefly, the cytotechnologist at the radiology suites prepared slides on-site and used the telecytopathology system (Fig. 1) comprising an Olympus (Olympus America, Center Valley, PA) CX41 microscope and a digital camera with NetCam software (Olympus) to send live video images via internet to the cytopathologist's desktop at a remote site.
The cytopathologists interacted with the cytotechnologists via a hand-free Vocera (San Jose, CA) voice communication system. Once the ROSE was performed, the radiologist was informed of the preliminary diagnosis. Recommendations for collection of additional material for ancillary studies were made as deemed necessary.
Results
A total of 178 IGFNAs of liver lesions performed in ultrasound-guided and CT-guided suites underwent telecytopathology-assisted ROSE.
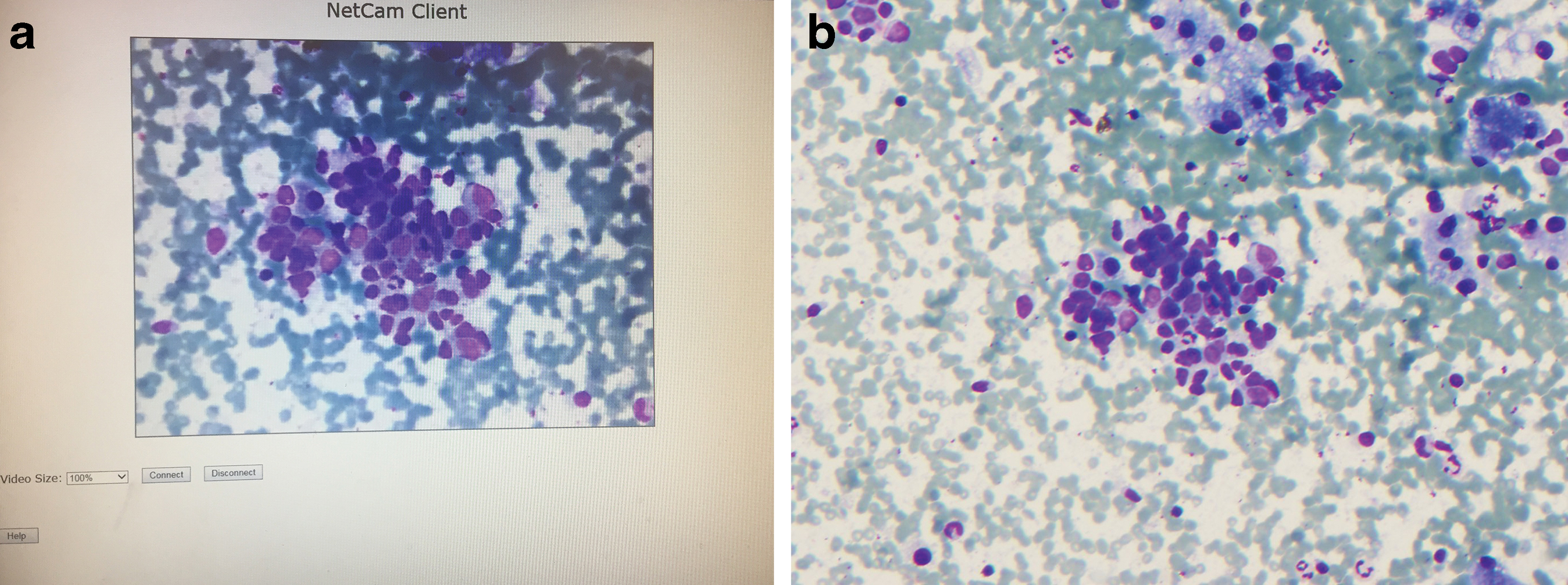
Table 1 shows the follow-up of the final cytology diagnosis on all IGFNA cases with the ROSE via telecytopathology. All 98 cases with initial telecytopathology diagnosis of malignant corresponded with a final cytology diagnosis of malignant (Fig. 2). Forty-two of the 49 cases with an initial benign diagnosis corresponded with benign diagnosis on final cytology (Fig. 3). The remaining seven cases were upgraded to a suspicious/positive for malignancy category. Of the 27 cases with an initial telecytology diagnosis of suspicious, final cytology diagnosis included malignant (23), suspicious (3), and one was downgraded to benign. Two of the four unsatisfactory cases remained unsatisfactory on final cytology, and two cases were upgraded to suspicious (one) and malignant (one) categories. In summary, the final cytology diagnosis after using telecytopathology yielded a high concordance or accuracy rate of 94.4% (168/178). The upgraded and downgraded diagnosis rates were 5% (n = 9) and 0.01% (n = 1), respectively.

Follow-Up of Final Cytology Diagnosis on All Image-Guided Fine-Needle Aspiration Cases with the Preliminary Diagnosis Rendered via Telecytopathology
Table 2 provides a detailed analysis of the 10 cases with diagnostic discrepancy between telecytopathology-assisted ROSE and final cytology diagnosis. In one of the cases that were downgraded to benign on final cytology diagnosis, reactive ductal cells during telecytopathology ROSE were misinterpreted as suspicious for malignancy. In five of seven cases with ROSE of benign and final cytology diagnosis of suspicious/malignant, additional material was present on alcohol fixed smears and cell blocks that were not available for review at the time of ROSE. The two remaining cases were misinterpreted as reactive hepatocytes during ROSE and represented cases with final cytology diagnosis of melanoma (one) (Fig. 4) and suspicious for hepatocellular carcinoma (one). Availability of additional material that could not be reviewed at the time of ROSE also resulted in reclassification of two cases with unsatisfactory ROSE to suspicious/malignant.

List of Cases with Reason for Discrepancy Between the Preliminary Diagnosis During Rapid On-Site Evaluation Using Telecytopathology and the Final Diagnosis
ROSE, rapid on-site evaluation.
Discussion
Several studies have examined the role of dynamic telecytopathology-guided ROSE in aspiration cytology. 11 –21 However, there remains an increased need for review of organ-based telecytopathology-assisted ROSE so that organ- and lesion-specific diagnostic dilemmas encountered with utilization of telecytopathology can be better understood and resolved. Also, the interventional radiologists, endoscopists, and gastroenterologists performing organ-specific FNAs would find it easy to embrace the utilization of telecytopathology for ROSE if it can be shown that it is highly accurate for organ-specific FNAs. To the best of our knowledge, this is the largest series of cases exclusively focusing on ROSE with dynamic telecytopathology of IGFNA of hepatic lesions.
In our study, we demonstrated a high diagnostic accuracy of 94% for telecytopathology-assisted ROSE of IGFNA of hepatic lesions. Our accuracy rate is comparable with our previously reported telecytopathology-assisted concordance rate for other body sites, including pancreas (84%), thyroid (94%), axillary lymph nodes (96%), head and neck (94.8%), and lung (96%). 11,13,14,17,19 Our results are also within the concordance rate range of 84% to 97% reported for ROSE using conventional microscopy, which requires the presence of pathologists on-site. 12,14,19,21,22
In our study, 5% of cases were upgraded from an initial ROSE of benign to suspicious/malignant for final cytology diagnosis. Lin et al. reported a diagnostic upgrade rate of 6.7% in their study. 23 Similar to our study, in the vast majority of their cases, lack of availability of all diagnostic material (e.g., cell blocks, additional smears stained later in the laboratory, and ancillary studies) at the time of ROSE contributed to diagnosis upgrade at the time of final cytology sign out. In addition, in two of our cases, malignant cells seen on Diff-Quik smears were misinterpreted as reactive hepatocytes at the time of telecytopathology-assisted ROSE, resulting in erroneous preliminary diagnosis of benign. Our diagnostic downgrade rate of 0.5% (n = 1) was also attributable to misinterpretation of reactive ductal cells as suspicious for malignancy.
Recently, Selhi et al. demonstrated that ROSE by cytopathologists using conventional microscopy shows significant improvement in diagnostic accuracy of IGFNA of hepatic lesions. 3 There is quite a variation in the practice of on-site cytology interpretation by pathologists in the United States. The cytopathology laboratories are finding it challenging to provide pathologists on-site for this time-consuming procedure due to time and distance constraints and poor reimbursements. Although some institutions collect without adequate assessment, it compromises the diagnostic yield of the specimen and may result in additional repeat procedures. 24,25
Similar to other studies on dynamic telecytopathology-guided ROSE from different body sites, we have shown that telecytopathology ensures accurate preliminary diagnosis in IGFNA of hepatic lesions. 14 –21 It circumvents the need for the cytopathologist to present on-site and allows the pathologist to triage specimens for various ancillary studies, for example, flow cytometry for hematopoietic lesions, cytogenetic analysis, and molecular studies for pediatric and adult tumors metastatic to the liver. It also provides a suitable alternative to conventional microscopy that requires the presence of a pathologist on-site for these time-consuming IGFNAs.
Telecytopathology-guided adequacy assessment may reduce the number of passes per lesion, which mitigates the problems of travel time to distant sites, the time required to wait between multiple sites on the same patient, or repeat FNA biopsies, thereby improving the overall efficiency by decreasing the time commitment for the pathologist and enhancing the use of health care resources. 6,8,21,26
The success of telecytopathology-assisted ROSE of hepatic lesions is dependent on an experienced cytotechnologist who is capable of transmitting real-time images and shows significant findings while interacting with the cytopathologist via Vocera or telephone, as has also been emphasized in other studies. 14,21 The need for the pathologist to be conversant with telecytopathology for interpretation of real-time images cannot be overemphasized. We did not perform any validation protocol for the present study. However, before introduction of telecytopathology at our hospital in November 2009, an internal validation testing was completed, which was fairly similar to a recent validation study by McCarthy et al. 27
The low number of unsatisfactory cases in our study is attributed to the expertise and proficiency of the interventional radiologists performing the procedures at our institution. Evaluating each pass for adequate material and performing additional passes if the pass was judged as inadequate also contributed in eliminating unsatisfactory cases.
In conclusion, we demonstrated that on-site telecytopathology preliminary evaluation for IGFNA of liver lesions appears to be highly accurate and reaches a comparable accuracy rate to other organ-based telecytopathology-assisted ROSE studies as well as to ROSE accuracy with conventional microscopy. As laboratories are subjected to increasing volume and time demands, and patients suffer from increase in health care costs, telecytopathology ROSE for IGFNA of liver lesions clearly demonstrates its value in delivering optimal patient care and improving patient outcomes. Our study supports ROSE for IGFNA of liver lesions as a suitable alternative to on-site conventional microscopy and proves its ability to overcome problems related to time commitment and distance constraints precluding pathologists' on-site involvement in ROSE.
Footnotes
Acknowledgment
The authors acknowledge the cytotechnologists at the SUNY Upstate Medical University for assisting in this study.
Disclosure Statement
The authors contributed equally to this study and declare that there is no conflict of interest regarding the publication of this study.
The authors affirm that this article is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
The authors confirm that ethics committee approval was sought where necessary and is acknowledged within the text of the submitted study.
Funding Information
This study is Institutional Review Board (IRB) exempted and there is no funding to report for the submission of this study.