
Abstract
Background:
Since 1990s, directly observed therapy (DOT) has been the standard-of-care for tuberculosis (TB), although it is cumbersome for patients as well as service providers. For raising implementation, an alternative delivery method with good potential is telehealth. The current study assessed the clinical and cost benefit of video directly observed therapy (VDOT), compared with DOT service.
Methods:
This prospective randomized controlled trial randomized adults with bacteriologically confirmed pulmonary TB to the intervention (VDOT) or control (DOT) group. The observation data for DOT and VDOT were updated by observers until the end of treatment or until the study concluded. The primary outcome was the TB treatment result defined by the World Health Organization (WHO) as used in some other studies conducted in North India and England as follows: good (cured and treatment completed), poor (death and failure), relocation, and lost to follow-up and others (refused, adverse reaction, not a TB case). Other secondary measures were treatment adherence, patient satisfaction, time and cost spent on DOT or VDOT.
Results:
On analyzing the results from 405 participants from each study arm, we found very high rates of treatment completion (96.1% with VDOT vs. 94.6% with DOT). The two observed treatment methods had no statistical differences, and all could accomplish their tasks well. Average time per dose observed was 16.5 min (standard deviation [SD] 12.1) for VDOT, while 44.1 min (SD 3.7) for DOT (including travel time), p < 0.01. And the cost incurred on VDOT was ¥34.3 (SD 3.8) manmo, which was statistically lower compared with ¥71.6 (SD 49.7) manmo in the DOT group, p < 0.01. Most of the patients in both groups believed that observed treatment (VDOT/DOT) helped them not to miss doses (185 [93.0%] vs. 171 [86.7%], p = 0.057). Patients in the VDOT group had a better experience compared with those in DOT group. They thought the way was convenient and comfortable (191 [96.0%] vs. 111 [56.6%], p < 0.001), would choose the original way if necessary (191 [96.0%] vs. 113 [57.7%], p < 0.001), and would recommend the method to other patients (191 [96.0%] vs. 113 [57.7%], p < 0.001).
Conclusion:
The study showed that VDOT enabled meaningful direct observation for TB patients through mobile devices, which was highly acceptable to patients and health care providers. It also saved time and is a cost-effective method, enabling the use of the saved money to other much-needed areas for TB.
Introduction
Globally, tuberculosis (TB) is the primary reason of death due to an infectious disease. 1 Although TB is curable through antibiotics, the long treatment regimens (≥6 months) may lead to poor compliance, increasing the transmission of ongoing disease, mortality, and acquired resistance to drugs. 2 –4 Thus, the recommended method by the U.S. Centers for Disease Control and Prevention and other health agencies is directly observed therapy (DOT) as the standard-of-care for TB patients to ensure adherence to anti-TB treatment. 5,6 While DOT is a reliable model for TB treatment, it may be an inconvenient practice because it is labor intensive and may hinder effective therapy. Moreover, for the public health care systems, which are often cash-strapped, the expense may be prohibitive. 7,8
The use of information technology and telecommunication for providing clinical health care to isolated or distant individuals is called telemedicine. There were some studies which showed that video directly observed therapy (VDOT) for treatment of TB might be a good practice model for TB treatment. However, these studies have a small sample size or require specialized equipment. 9 –12 The current study was planned to furnish high-quality evidence on the acceptability, effectiveness, and cost-effectiveness of VDOT for patients with TB.
Methods
Study Design
The Medicine Ethics Committee of Shandong Provincial Chest Hospital, Shandong University School, consented to the study protocol. The study was carried out as per the tenets of the Declaration of Helsinki. The trial was controlled, two-group prospective randomized, in which adult patients with bacteriologically confirmed pulmonary TB were randomized to the intervention (VDOT) or control (DOT) group. All patients provided written informed consent.
Participants
We consecutively enrolled all eligible patients admitted to Shandong Provincial Chest Hospital Affiliated to Shandong University from January 2018 to December 2018. Every TB patient was eligible if one met each of the following inclusion criteria: (1) ≥18 years of age, (2) bacteriologically confirmed pulmonary TB, (3) can be treated out of hospital, (4) ≥1 month of treatment remaining, (5) live in Jinan City, (6) after being trained, could efficiently use a smartphone accompanied with videoconferencing and identify and self-administer the prescribed medications, and (7) were able and willing to furnish informed consent.
The criteria for exclusion were as follows: (1) minors, (2) individuals with either confirmed or with suspected drug resistance, (3) patients who could not efficiently use a smartphone because of certain physical conditions (i.e., diminished vision, severe arthritis), and (4) denied consent.
Randomization and Masking
The participants were allocated groups randomly, as per computer-generated 1:1 simple randomization. The study research coordinator (K.C.) was used to generate random allocation sequence, and held by the study administrator in a secure opaque envelope and concealed from the study care coordinators (CCs). For group assignment, the participants chosen by CCs contacted the study administrator. Due to the nature of the intervention, health professionals, researchers, and participants were not blinded to the allocation of trial group.
Protocols
A schematic of the followed procedures are presented in Figure 1. During the morning round, screening on a daily basis was done for all patients for study recruitment. The participants who consented were to furnish information about their medical history, socioeconomic factors, demographics, and use of mobile phones. The patient's medical file was used to obtain additional information about diagnosis and treatment regimen. After enrollment, patients were allocated to either the VDOT or DOT (control) group.
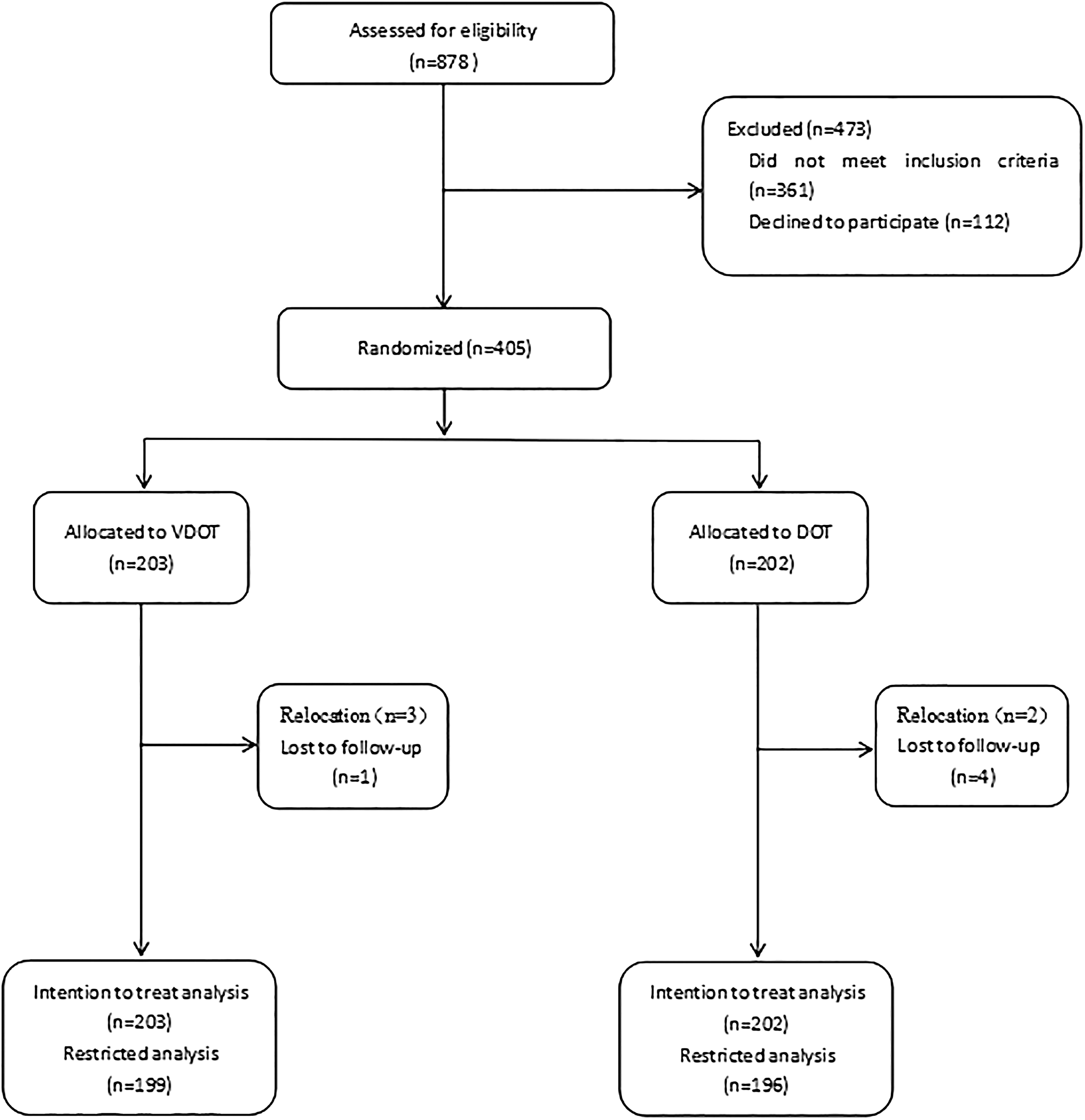
Enrollment and randomization. DOT, directly observed therapy; VDOT, video directly observed therapy.
VDOT was carried out using the information platform (Youping Technology Co., Ltd., Guangzhou, China), a synchronous smartphone application (“App”) that could be used in both iOS and Android system. A WiFi connection or the 3G or 4G mobile network could successfully enable its functioning. The health staff trained the patients to use the smartphones and go along with the VDOT process. After one patient was included in the study, he made an appointment with the administrator for reminder time. When he should take medicine, reminder information was sent to the patient's phone by special public number. After the patient logged on to the system, he talked to the administrator via live video and took medicine directly under the administrator's sight. If the patient had any problems with the disease and treatment, he could also give feedback at the same time. For missed VDOT appointments, follow-up was done through phone calls and home visits, if the former were unsuccessful. For routine clinic visits (i.e., monthly), both participants and nonparticipants carried out the same schedule for monitoring health status and medication refills. The system login needed to be validated by the patient's mobile phone and approved by the manager. The software was maintained by the development company to ensure information security to the maximum extent and eliminate the patient's concerns.
DOT was delivered as per the regular clinical protocol and required observation of treatment by a health care or lay worker once every 2 days.
The observation records for VDOT and DOT were provided by observers until the end of treatment or study. In the research, both TB follow-up records and video images were archived in the records for audit of compliance in the VDOT group, while in the DOT group only TB follow-up records were archived as the World Health Organization (WHO) required.
Outcome Measures
The chief outcome was the TB treatment result defined by the WHO as used in some other studies conducted in North India and England as follows (Table 1): good (cured and treatment completed), poor (death and failure), relocation, lost to follow-up and others (refused, adverse reaction, not a TB case). 13,14 Other secondary measures were treatment adherence; patient satisfaction; time and cost spent on DOT or VDOT.
Definitions of Treatment Outcomes for Tuberculosis Patients
TB, tuberculosis.
Analyses of Data
The SPSS software (IBM SPSS Statistics for Windows, Version 20.0; IBM Corp., Armonk, NY) was used to analyze both inferential and descriptive demographic variables. Data are expressed as mean ± SD (standard deviation) for parametric variables and median ± interquartile range for nonparametric continuous variables. The results for continuous variables were compared using t-test, and for categorical variables, the Fisher exact test or χ2 test was used. The significance level was set at p < 0.05.
Results
We enrolled 405 participants in Shandong University-affiliated Shandong Provincial Chest Hospital from January 2018 to December 2018. Two hundred three randomized to VDOT and 202 randomized to DOT. The characteristics of study participants are listed in Table 2. Participants in the two groups had no statistical variations in age (40.2 ± 16.1 vs. 44.3 ± 17.7 years, respectively, p = 0.237), sex (male: 146 [71.9%] vs. 138 [68.3%], respectively, p = 0.428), highest level of education (university or above: 33 [16.3%] vs. 41 [20.3%], respectively, p = 0.293), and TB treatment region distribution (first-line: 172 [84.7%] vs. 165 [81.7%], respectively, p = 0.412).
Baseline Characteristics of Study Participants
DOT, directly observed therapy; SD, standard deviation; VDOT, video directly observed therapy.
The primary outcome data were available for all 405 patients. In the VDOT group, 186 (91.6%) were cured, 9 (4.4%) completed treatment, 0 (0%) died, 4 (1.0%) had treatment failure, 3 (1.5%) relocated, and 1 (0.5%) was lost to follow-up. In the other group, 177 (87.6%) were cured, 14 (6.9%) completed treatment, 0 (0%) died, 5 (2.0%) had treatment failure, 2 (1.0%) relocated, and 4 (2.0%) were lost to follow-up. Also, all the differences had no statistical significance (Table 3).
Treatment Outcomes of Patients Treated for Tuberculosis Under Video Directly Observed Therapy and Directly Observed Therapy
The TB program bore the costs for items such as sputum examination, drugs, and other medical consumables, and the costs for these items would be the same irrespective of the treatment group. Therefore, we did not count this part. Also, the costs of those patients who relocated or were lost to follow-up were not included. Average time per dose observed was 16.5 min (SD 12.1) for VDOT, while 44.1 min (SD 32.7) for DOT (including travel time), p < 0.01. Moreover, the cost incurred on VDOT was ¥34.3 (SD 3.8) manmo, which was statistically lower compared with ¥71.6 (SD 49.7) manmo in the DOT group, p < 0.01 (Table 4).
Costs Associated with Video Directly Observed Therapy and Directly Observed Therapy
The information platform cost was ¥72,000 every year.
Most of the patients in both groups believed that observed treatment (VDOT/DOT) helped them not to miss doses (185 [93.0%] vs. 171 [86.7%], p = 0.057). Patients in the VDOT group had a better experience compared with those in the DOT group. They thought the way was convenient and comfortable (191 [96.0%] vs. 111 [56.6%], p < 0.001), would choose the original way if necessary (191 [96.0%] vs. 113 [57.7%], p < 0.001), and would recommend the method to other patients (191 [96.0%] vs. 113 [57.7%], p < 0.001) (Table 5).
Summary of Patient Satisfaction Survey
Discussion
Diagnosis and successful treatment of TB can avert millions of deaths each year. Any improvement in TB treatment is important in terms of both public health and economics. Worldwide, the standard treatment for patients of TB is DOT. 15 The present study compared VDOT with DOT.
The baseline results of this study showed that male patients, high school or below education patients and young adults are more, which was basically consistent with the results of the fifth national epidemiological sampling survey for TB in 2010. 16 The constituent ratio of first-line treatment was difficult to compare because of patient origin and exclusion of multidrug-resistant patients. The participants in the two groups had no statistical differences.
There were researches which reported that the patients treated by VDOT and in-person DOT has similar outcomes. 12,17 In the present study, to ensure the smooth progress of the project, we used the method of automatic and manual cooperation in the VDOT group and the original manual way in the DOT group. The compliance of both groups was high, so we also observed treatment completion at high rates (96.1% with VDOT vs. 94.6% with DOT). The two observed treatment methods had no statistical differences, and all could accomplish their tasks well.
Each VDOT session had an average duration of 16.5 min (SD 12.1), which saved patients and staff a lot of time compared with DOT. Furthermore, unlike DOT, VDOT would not be interrupted by adverse weather or if patients traveled outside the city. In this study, many of the patients who vacationed outside Jinan during their treatment had successfully observed treatment by video. In adverse weather, VDOT was advantageous to both health staff and patients by enabling no travel for observations, which also saved expenses. The cumulative cost for the information platform was ¥72,000 every year. Approximately the average cost of VDOT patients was ¥34.3 (SD 3.8) manmo (contains a small amount of the cost of going to the clinic for a review). If the number of patients who used the information platform increased, the average cost would be further reduced. Also, it was ¥71.6 (SD 49.7) manmo in the DOT group, which almost were travel expenses and would not change much with patient number. It was an impressive saving compared with DOT.
Although most of the patients in both groups believed that observed treatment helped them not to miss doses, patient acceptance of VDOT was higher. VDOT visits were briefer, and conferred high scheduling flexibility, convenient both for patients and for the staff of the health department. Patients shared positive views about VDOT as a health promotion intervention for TB care, and were more willing to receive VDOT and recommend it to other patients. There is a little episode, all three patients of the VDOT group who relocated to other areas from Jinan once upon a time called to express that they wanted to continue VDOT instead of conventional DOT. We were very happy to receive their calls, but regrettably refused their requests because of national policies and research regulations.
The study also had some limitations. First, patients with drug-resistant TB were ineligible, and only the patients who could willingly use the technology were selected. The likelihood of the participants taking the treatment was greater than general patients. Thus, treatment adherence could not be compared by us. However, the satisfaction with VDOT seemed less likely to have been affected. Second, this approach may not apply to all settings and to all patients; the areas with poor signals may not have internet facility, and patients may not be comfortable with technology or not have the device and economic capacity to use a video system dependent on the internet. With the development of technology and economy, these conditions may gradually improve. Particularly, privacy was another concern of VDOT: the transmitted protected health information through the internet could be potentially compromised, and we used special encryption software to avoid it as much as possible.
Conclusion
The study showed that VDOT in mobile devices enabled direct relevant observation, which was highly acceptable to TB patients as well as providers, being cost-effective, while significantly saving time and money. The savings of cost from VDOT can be invested in other much-needed areas for TB. 18 Besides, with rapid global usage of mobile phone networks and smartphones, an increase in the use of digital technologies will be more feasible. 19
Footnotes
Acknowledgments
The time and cooperation given by the patients and staff are greatly appreciated. The authors are especially grateful to Youping Technology Co., Ltd. for conducting the VDOT sessions.
Disclosure Statement
No competing financial interests exist.
Funding Information
This project was funded by grants from Shandong Medicine and Health Science and Technology Development Plan (2017WS443) and Shandong University-affiliated Shandong Provincial Chest Hospital.