
Abstract
Background:
Telemedicine market in China has been rapidly developing. However, no systematic review has been published in China. Details of the implementation of telemedicine interventions in the chronic obstructive pulmonary disease (COPD) in China have not been described, and the effectiveness of telemedicine interventions is still unclear. Therefore, in this review, we describe the implementation details of telemedicine intervention in China and access the efficacy of telemedicine.
Materials and Methods:
A literature search was conducted in Embase, Cochrane Library, PubMed, China National Knowledge Infrastructure (CNKI), Wan Fang Data, and China Science and Technology Journal Database by July 9, 2018.
Results:
A total number of 24 studies were meta-analyzed. There are many differences during the implementation of telemedicine in China. Quality of life in the group of the telemedicine intervention was better than that in the control group (mean difference = −4.93 [95% confidence interval; CI −6.86 to −3.01], p < 0.00001), but the heterogeneity is high (I 2 = 86%, p = 0.0001). The rates of hospitalization were lower than those in the control group (odds ratio = 0.24 [95% CI 0.20–0.29], p < 0.00001), and the heterogeneity was low (I 2 = 25%, p = 0.14).
Conclusion:
The implementation of telemedicine in China has not yet been standardized. Nonetheless, results of our review indicated that telemedicine in China can improve the quality of life and reduce the rates of hospitalization in COPD patients.
Introduction
In 2018, chronic obstructive pulmonary disease (COPD) patients of over 20 years in China have reached about 100 million. 1 Reportedly, COPD will become the third leading cause of death in the world by 2020. 2 Although the management of COPD in primary health care has advanced, it is still the second leading cause of emergency hospitalization. 3 Therefore, there is an urgent need to strengthen the management of COPD to delay the disease process and improve the quality of life of patients.
Telemedicine is defined as the use of electronic information and communication technology by medical personnel to provide and support health care to patients when they are far away. 4 In 2016, the telemedicine market (including remote monitoring, videoconferencing, and online consultation) has reached about 6.15 billion Yuan in China. With the development of telemedicine technology and the increase of the number of elderly chronic patients, the demand of medical service market is further increased. According to prognoses of the China Prospective Industry Research Institute (CIPI), the telemedicine market in China is expected to exceed 23 billion Yuan by 2023. 5 Currently, the application of telemedicine in chronic disease management has attracted considerable research attention. 6
Telemedicine is a complex intervention, including multiple implementation components, human support, technology, basic equipment, and a patient's acceptance of technology, which will affect the outcome. 7 –10 Telemedicine technology includes the use of videoconferencing, internet platforms, storage, forwarding equipment, and so on. 11 Although the effectiveness of telemedicine in the improvement of quality of life and the reduction in the rates of hospitalization in COPD have been previously investigated, controversial results have been obtained. 12,13
The telemedicine market in China has been rapidly developing, but no systematic evaluation or meta-analysis published in China exists. Hence, the effectiveness of telemedicine intervention in COPD in China is still unclear. Therefore, this article described our research findings of Chinese telemedicine in COPD patients from the aspects of providers, technology, and duration. Quality of life and the rates of hospitalization were subjected to meta-analysis.
Materials and Methods
Data Sources and Searches
A literature search was performed by two researchers (F.L. and Y.J.), in July of 2018, on Embase, Cochrane Library, PubMed, China National Knowledge Infrastructure (CNKI), Wanfang data, and China Science and Technology Journal Database (CSTJ). Additional searches were conducted for relevant studies from the references of the included articles. The retrieval form of the Medical Subject Headings (Mesh): [Pulmonary Disease, Chronic Obstructive] and [Telemedicine or Remote Consultation or Education, Distance or Telenursing or Telephone or Cell Phone or Patient Portals or Electronic Mail or WeChatTM (Tencent Holdings, Ltd., Shenzen, China) or Television] and [China or Hong Kong or Taiwan or Macau]. The retrieval form is available in Appendix A1.
Selection Criteria
Clinical trials conducted in China and published in the Chinese or English language were included. (1) COPD was definitely diagnosed by medical units. (2) Telemedicine was an intervention during the process of COPD rehabilitation. (3) Control group types were not restricted. (4) Among the subjective or objective outcome indicators, hospitalization rate or quality of life was assessed by CAT (COPD Assessment Test). (5) Randomized-controlled trials. COPD complications and telemedicine technology used only as a survey media were excluded. The screening of research literature was conducted by two researchers (F.L. and Y.J.). A third researcher (G.X.) was consulted when differences in opinions occurred.
Data Extraction and Quality Assessment
Two researchers (F.L. and Y.J.) independently extracted data on the characteristics of the included studies (first author's name, publishing time, area, participants, intervention group, and control group) and intervention strategies (providers, technologies, duration, and outcomes), and assessed their quality. Any disagreements during the process were resolved by discussions with a third researcher (G.X.). In this review, we used the Cochrane risk-of-bias assessment tool. 14 Based on the aforementioned evaluation criteria, a low-risk, unclear, and high-risk bias was assessed.
Data Analysis
The included studies were analyzed by Review Manager (RevMan; Version 5.3). The rates of hospitalization were measured by odds ratio (OR) and Mantel-Haenszel (M-H). Mean difference (MD) and inverse variance (IV) were used to evaluate the results of CAT. The 95% confidence intervals (CI) were used to characterize the reliability of the summary results. In addition, I 2 statistics was utilized to access the heterogeneity of included studies (I 2 < 50%, heterogeneity was accepted), and funnel plot was made for the bias of synthetic evidence. A fixed-effect model was applied to address the cases of lack of heterogeneity. In case the results were heterogeneous, the random-effect model was used. Otherwise, sensitivity analysis and subgroup analysis were performed to explain the sources of heterogeneity.
Results
The database search identified 974 potentially relevant articles that were distributed as follows: CNKI (n = 332), Wanfang (n = 402), CSTJ (n = 225), Embase (n = 5), Cochrane Library (n = 4), and PubMed (n = 6). After exclusion of duplicates, 470 articles were removed. During the process of the title and abstract screening, 432 articles were eliminated due to the following reasons: meta-analysis (n = 5), conference report or other types of articles (n = 34), COPD was not the main object (n = 92), investigation and cause analysis (n = 86), the trial was not carried out in China (n = 34), telemedicine was not the main intervention method (n = 177), and qualitative research (n = 4). After reading the full-text, 45 studies were excluded as 18 studies were not the randomized-controlled trial, and 27 studies did not evaluate the rates of hospitalization or did not use CAT to assess the quality of life. Finally, 27 studies were included in our analysis. Four studies 15 –18 were included in the foreign database, and 23 studies 19 –41 were present in the Chinese database, among them, eight studies with English abstracts (Supplementary Data 1). The results of three of the studies did not meet the requirements of the present meta-analysis 34,36,38 ; thus, 24 studies were finally included in the analysis. The literature screening process can be seen in Figure 1.

Flow diagram of study selection process.
Study Characteristics
Table 1 represents the characteristics of the study. Two studies were conducted in Taiwan, 15,18 and one was performed in Hong Kong. 17 The others were carried out in the Chinese mainland. Four of the studies were realized in first-tier cities, 16,21,37,40 whereas six studies were carried out in new frontline cities. 26 –30,34,36,38 One study was conducted in second-tier cities, 27 eight studies in third-tier cities, 19,22 –24,32,33,39,41 two in four-tier cities, 31,35 and one in five-tier cities. 20,42 Two studies did not indicate where they were performed. One study was carried out in Guangxi Zhuang Autonomous Region and the other was in Shaanxi Province. 25,28 The number of the subjects included varied. The minimum sample consisted of 40, 17 whereas the maximum sample was 224, 41 and the average number of samples was 115. Most randomized-controlled trials compared telemedicine interventions with routine discharge guidance.
Characteristics of the Included Studies
ATS, including internet, wireless systems, database and software for decision analysis.
ATS, ASTRI telecare system; CG, control group; ICU, intensive care unit; IG, intervention group; NA, not available.
Process of Telemedicine Intervention Implementation
The components of telemedicine intervention in COPD in China are summarized in Table 2. Nurses were the providers of telemedicine interventions in 16 studies, 17 –21,24,26,29,31 –33,35 –37,39,40 of which 3 studies were provided by nurses at different levels. 31,32,35 In two studies, doctors and nurses worked together to provide telemedicine interventions to COPD patients. 22,30 Four studies were conducted by doctors, 23,26,34,41 and one of them was conducted by doctors at different levels. 34 One study was conducted by a multidisciplinary team of doctors, psychologists, and community health workers to provide telemedicine interventions. 32 The providers of telemedicine interventions in three studies were researchers. 15,27,38 Another study was performed by clinical pharmacists. 16 The applications of telemedicine technology included telephone, 15,16,19,22 –24,26,28,29,31 –33,37,40 WeCha, 20,21,30,34 –36 QQ, 25 telecare system, 17 electronic diary, 18 mobile application, 15,27 mobile short message, 38 and so on. The duration of the interventions was different. There were 2-month, 17 3-month, 27,28,34,39 –41 22-week, 38 6-month, 18,23,31,33,35 –37 and 12-month 15,16,19,21,24 –26,30,32 studies. A total of 21 studies assessed the rates of hospitalization 16 –18,27 –34,36 –41,43 –46 and 6 studies assessed the quality of life. 27,34,38 –41 In addition, behavioral indicators are most frequently assessed, followed by functional indicators.
Components of Telemedicine in Chronic Obstructive Pulmonary Disease in China
+, positive results; −, negative results; no, no difference.
6MWD, 6-minute walking distance; COPD, chronic obstructive pulmonary disease; CAT, COPD Assessment Test; ESCA, Exercise of Self-Care Agency; Ex-SERS, Exercise Self-Regulatory Efficacy Scale; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; ICU, intensive care unit; ISWT, Incremental Shuttle Walk Test; mMRC, modified British Medical Research Council Scale; NA, not available; PH, potential of hydrogen; SCL-90, symptom check list 90; SF-12, Jane's Health-Related Quality of Life Questionnaire.
Quality Assessment
In the quality evaluation (Table 3), 5 studies were classified as grade A, 21 as grade B, and only 1 as grade C. 43 We found that 51.6% of the studies were unclear in terms of random sequence generation, 88.9% in allocation concealment, 77.8% in blind design of researchers and subjects, and 74.1% in blind design of outcome evaluation. A summary of the bias risk assessment is displayed in Figure 2.
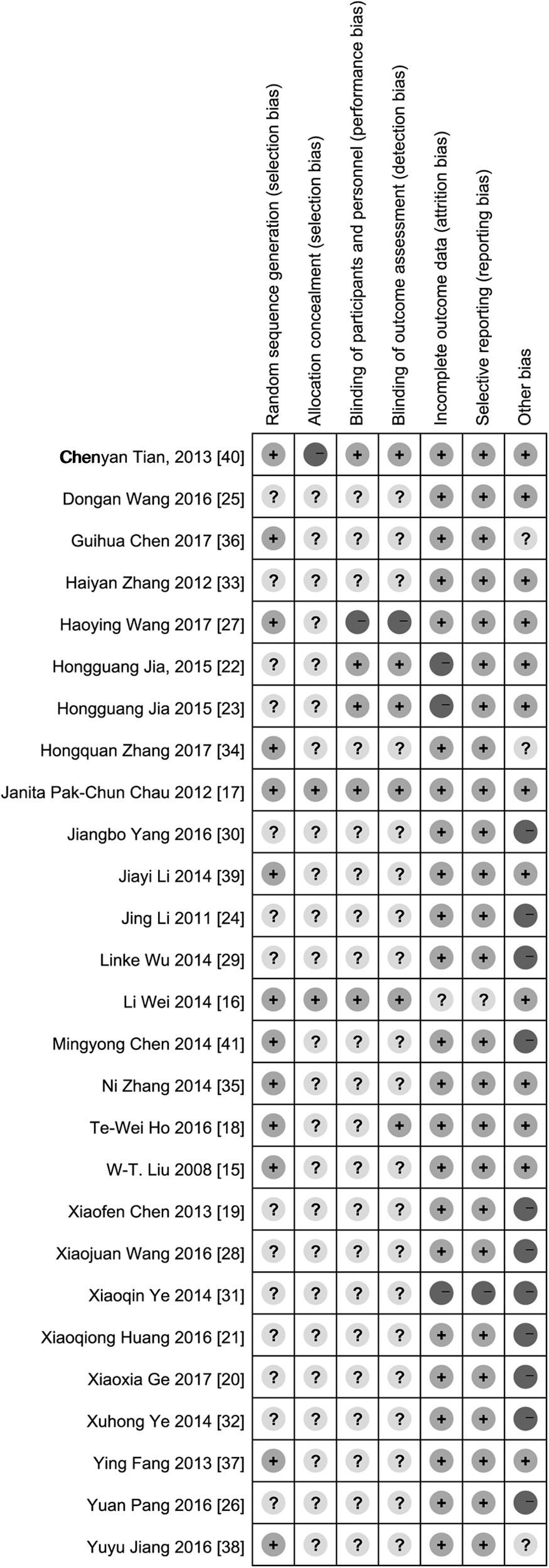
Risk-of-bias summary.
Quality Assessment of the Included Studies
Outcome: Quality of Life
As can be seen in Figure 3, telemedicine intervention significantly improved the quality of life of COPD patients (MD = −4.93 [95% CI, −6.86 to −3.01], p < 0.00001), but the heterogeneity was high (I 2 = 86%, p = 0.0001). Sensitivity analysis was performed by removing a single study. When the study of Tian et al. was removed, there was no heterogeneity in a pooled analysis (I 2 = 0%, p = 0.65) 40 (Fig. 4). Subgroup analysis of telephone and nontelephone (WeChat, mobile application, e-mail, etc.) in the studies showed that both telemedicine intervention strategies could improve the quality of life of COPD patients (MD = −4.50 [95% CI −5.08 to −3.92], p < 0.00001), as depicted in Figure 5. Considering that fewer studies were included and the duration of the studies were different, subgroup analysis was no longer carried out according to the duration of the studies. Two studies that were not included in meta-analysis also showed that telemedicine improved the quality of life of COPD patients and decreased CAT total score. 34,38

Forest plot of comparison: CAT. COPD, chronic obstructive pulmonary disease; CAT, COPD Assessment Test.

Forest plot of comparison: CAT: sensitivity analysis.
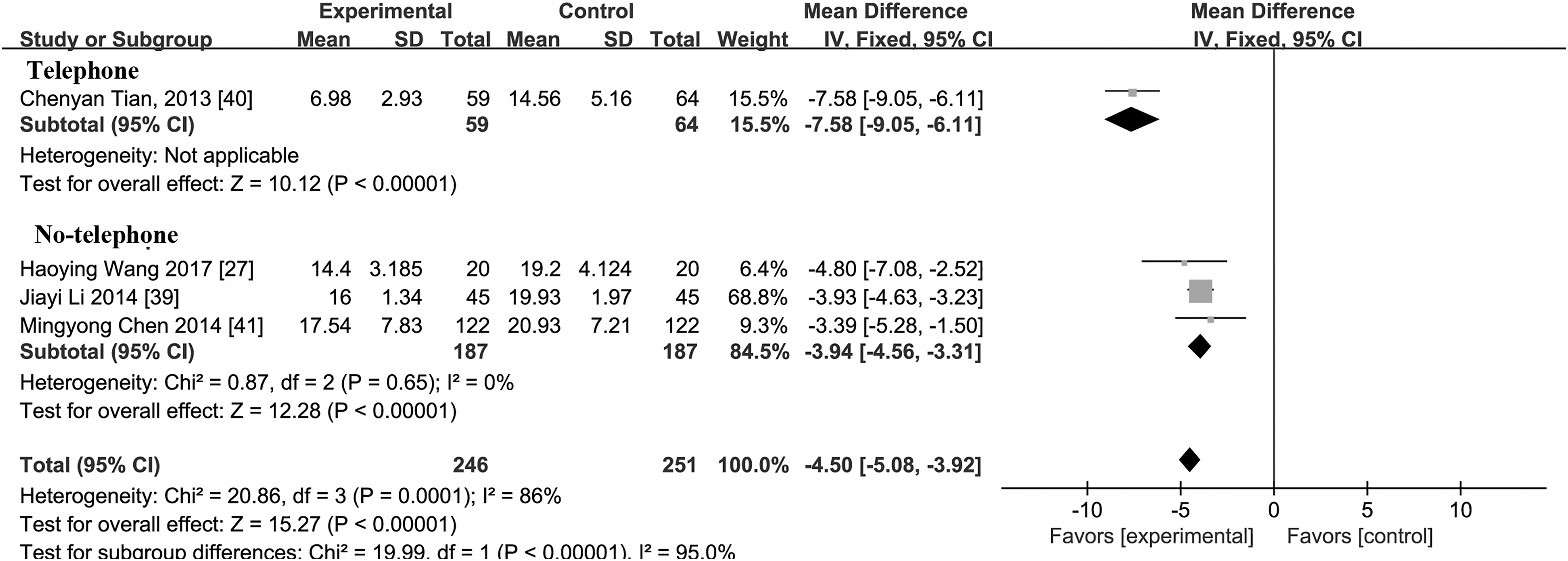
Forest plot of comparison: CAT: subgroup analysis of different technologies.
Hospitalization Rate
As seen in Figure 6, telemedicine reduced the rates of hospitalization of COPD patients (OR = 0.24 [95% CI 0.20–0.29], p < 0.00001), with low heterogeneity (I 2 = 25%, p = 0.14). A funnel plot for the combined analyses of 21 studies is presented in Figure 7. Subgroup analysis based on telephone and nontelephone (WeChat, mobile short message, telecare system, electronic diary, etc.) showed that both intervention strategies could reduce the rates of hospitalization of COPD patients (OR = 0.25 [95% CI 0.20–0.31], p < 0.00001), with low heterogeneity (I 2 = 25%, p = 0.14), as shown in Figure 8. Subgroup analysis was carried out according to two different intervening duration periods of <6 months and ≥6 months. The results showed that the rates of hospitalization of COPD patients were reduced (OR = 0.25 [95% CI 0.20–0.31], p < 0.00001), and the heterogeneity was low (I 2 = 25%, p = 0.14), as illustrated in Figure 9. A study that was not included in the meta-analysis showed that WeChat could also reduce the hospitalization rate of COPD patients. 36

Forest plot of comparison: the rates of hospitalization.

Funnel plot.

Forest plot of comparison: the rates of hospitalization—subgroup analysis of different technologies.

Forest plot of comparison: the rates of hospitalization—subgroup analysis of different durations.
Discussion
Implementation of Telemedicine in Patients with COPD in China
Based on the present review results, we can conclude that a unified standard has not yet been created for the implementation of telemedicine in COPD patients in China. Of note, nurses are the main providers of telemedicine intervention for COPD patients in China. Studies in other countries also suggested that nurses can be the leaders of telemedicine interventions. For example, nurses led a telemedicine intervention for diabetic patients in six U.S. rural areas, which improved the effectiveness of the intervention in diabetic patients and changed the self-management behavior of chronic patients. 47 Nage and Penner proposed a comprehensive conceptual model of telemedicine nursing practice. They elaborated on the characteristics of telenursing practice. It provided guidance for nurses to carry out holistic human-centered medical services through telemedicine technology. 48 Obviously, nurses have become the main providers of telemedicine intervention. As telemedicine interventions become part of continuing care, more nurses will practice telemedicine. However, whether this will conflict with the existing work of nurses and whether they are willing to play this role need to be elucidated in further research. In China, the research of the multidisciplinary team combined with telemedicine in the field of COPD is relatively less. There is only one study in this review involving multidisciplinary teams. 25 However, many studies in other more developed countries have established an obvious positive effect of multidisciplinary team inclusion. Importantly, multidisciplinary teams improved the quality of research work through telemedicine management. 43 Ko et al. suggested that multidisciplinary teams combined with telemedicine can reduce the length of rehospitalization and the number of hospitalizations in patients with acute COPD. 44 Providers are exceedingly important for the effectiveness of telemedicine interventions. Medical personnel with professional backgrounds, such as in the fields of informatics, respiratory disease, and rehabilitation nursing, may be the best providers of telemedicine intervention in the future, which may also lead to the emergence of new medical roles.
Telephone is the most commonly used telemedicine intervention technology in China, which has the advantages of simple operation and suitability for different groups of people. However, the effect of telephone intervention can be easily reduced by potential negative factors such as information misunderstanding and incomplete information. Telemedicine systems are widely applied as intervention technologies in other countries. By 2014, telemonitor systems have been used in 12 studies in 9 developed countries. 45 At present, some obstacles are still present in the wide application of telemedicine system. For example, Sanders et al. established the following main obstacles to the acceptance of telemedicine systems: (1) lack of training in the application of telemedicine devices and software systems; (2) perceived threat to disease through telemedicine system; and (3) possible negative effect on self-management and independence of elderly patients. 46 Moreover, Demiris et al. confirmed that early assessment of patients' acceptance of telemedicine systems contributed to increased patient adherence. 49
The psychological barriers in the application of telemedicine system can be eliminated by educating. 49 In addition, training of both intervention providers and patients can promote a more effective interaction between them. 50 Telemedicine system is a relatively new technology in COPD in China, especially in remote mountainous areas where the education level of patients is low and the internet is not covered. Nevertheless, the publicizing and education of the elderly COPD patients in China so as to accept and master this technology skillfully are difficult. Therefore, with the improvement of technological level, patients' service sense should be taken into account in the field of health care. The results of subgroup analysis in this review indicated that both telephone and nontelephone interventions can reduce the hospitalization rate. It is worth noting that in the era of rapid development of telemedicine technology, we cannot ignore the traditional intervention technology, especially in patients with high technology use disorders.
Our review established that the maximum duration of the telemedicine intervention is 12 months, whereas the minimum is 2 months. The guidelines for pulmonary rehabilitation in New Zealand and New York emphasized the insufficient evidence to support the benefits of extending the standard 8-week programs. 46 In this meta-analysis, the durations of <6 or ≥6 months improved the quality of life of patients with COPD and reduced the hospitalization rate. In addition, the included studies were not comprehensive in terms of evaluation indicators, compared with others; the present studies contained less evaluation on mortality and cost. 45 In the future, we will increase the evaluation index.
Analysis and Discussion of the Results of the Review
In summary, here we found that telemedicine interventions in China can reduce the hospitalization rate of COPD patients, which is similar to the results of existing system reviews.
12,13
In addition, our review showed that telemedicine intervention in China can improve the quality of life of COPD patients, which differs from the views of some researchers. Other researchers obtained results similar to those of our review such as McLean et al.
12
However, the systematic reviews of Gregersen et al.
51
and Jin et al.
52
revealed that telemedicine does not improve the quality of life of COPD patients. These controversial results may be due to the following reasons: Different assessment methods. Ulrik's system review uses many evaluation tools, such as SGRQ (St George's respiratory questionnaire), CCQ (Clinical COPD Questionnaire), SF-36 (Short Form 36), CRQ (Chronic Respiratory Disease Questionnaire), and MOS-SF12 (Medical Outcome Study, Short Form 12 Items Scale). The results showed that the quality of life in COPD patients did not improve significantly.
51
However, our review is to evaluate the quality of life of patients with COPD by using CAT. The results showed that the quality of life of patients with COPD has improved significantly. In fact, the 2011 GOLD (Global Initiative for Chronic Obstructive Lung Disease) guidelines clearly indicated that CAT can be used as a first-line assessment tool for evaluating symptoms in COPD patients.
53
CAT can be used as a reliable assessment tool for quality of life.
54
Furthermore, other studies have shown that over time, CAT can be used to assess risk and predict future disease deterioration, depression, and mortality.
55
Sample size, duration of intervention, and application of different technologies will affect the results of divergence. Our review only includes telemedicine research in China, which has some limitations and may lead to bias.
Telemedicine Theory and Model
It is well known that the theoretical model is helpful to understand the relationship between content, behavior mechanism, and expected results, and can provide guidance for the experiment. 56 However, no conceptual model of telemedicine has been mentioned in the included studies, similar phenomena also exist in COPD telemedicine interventions in other countries. At present, the theoretical models applied are as follows: (1) Thomas conducted a telemedicine intervention study based on the TECH conceptual model, which explored the effectiveness and cost-effectiveness of telemedicine in long-term disease management. 57 (2) Technology Acceptance Model explains why telemedicine is accepted by the patients. 58 (3) The Model for Assessment of Telemedicine (MAST) provided an evaluation framework to help decision makers choose the most effective telemedicine technology and use it optimally. 59 (4) The eHealth chronic care model (eCCM) was used to explore the supportive role of telemedicine technology in the self-management program carried out in chronic diseases. 50 However, the existing theories belong to the wide-area theory and cannot be directly applied to clinical practice. Future research should carefully address the mid-domain theory of telemedicine intervention. The best match among providers, technology, and patients is to be identified. For example, of great significance in this respect are factors, such as the professional background of the provider, the aging interface of technology, and the education level of patients.
The following limitations to the present review are to be acknowledged: (1) Many uncertainties were present in the quality evaluation of the research included in this review, and the research methods were not sufficiently rigorous. (2) Various telemedicine intervention technologies were included in the study, and thus, there is no comparison of the optimal effect of telemedicine technology. (3) This review also describes the implementation process, which may be incomplete and not detailed.
No unified standard exists for the implementation of telemedicine in China. This review established that telemedicine intervention in China can improve the quality of life and reduce the rates of hospitalization in COPD. At the time of rapid development of advanced technologies, we cannot ignore the role of traditional interventions, especially for those whose access to telemedicine or the internet is limited or absent. In addition, the results of this review are the first to find that CAT can be used as a reliable assessment tool for evaluating the quality of life of COPD patients in China. To date, Chinese researchers have not carried out studies on the correlation between CAT and disease deterioration, depression, and mortality.
Footnotes
Acknowledgments
We express our gratitude to the authors of the included studies.
Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by the Wuxi Maternal and Child Health Research Project (Grant/Award Number: MS201622); Wuxi Science and Technology Development Fund (Grant/Award Number: WX0302B010507180074PB); and Launching Fund of Research office of chronic disease management and rehabilitation, Wuxi School of Medicine, Jiangnan University.
Supplementary Material
Supplementary Data 1
Appendix A1
Search Name: liu
Date Run: 08/07/18 12:00:47.746
Description:
ID Search Hits
#1 MeSH descriptor: [Pulmonary Disease, Chronic Obstructive] explode all trees 5,067
#2 Chronic Obstructive Pulmonary Disease:ti,ab,kw (Word variations have been searched) 10,112
#3 COPD:ti,ab,kw (Word variations have been searched) 12,603
#4 COAD:ti,ab,kw (Word variations have been searched) 51
#5 Chronic Obstructive Airway Disease:ti,ab,kw (Word variations have been searched) 1,622
#6 Chronic Obstructive Lung Disease:ti,ab,kw (Word variations have been searched) 7,707
#7 Airflow Obstruction, Chronic:ti,ab,kw (Word variations have been searched) 450
#8 Airflow Obstructions, Chronic:ti,ab,kw (Word variations have been searched) 450
#9 Chronic Airflow Obstructions:ti,ab,kw (Word variations have been searched) 450
#10 Chronic Airflow Obstruction:ti,ab,kw (Word variations have been searched) 450
#11 #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 16,507
#12 #1 or #11 16,794
#13 MeSH descriptor: [Telemedicine] explode all trees 2,298
#14 Mobile Health:ti,ab,kw (Word variations have been searched) 2,227
#15 Health, Mobile:ti,ab,kw (Word variations have been searched) 2,227
#16 mHealth:ti,ab,kw (Word variations have been searched) 430
#17 Telehealth:ti,ab,kw (Word variations have been searched) 852
#18 eHealth:ti,ab,kw (Word variations have been searched) 245
#19 #15 or #16 or #17 or #18 3,326
#20 #14 or #19 3,326
#21 MeSH descriptor: [Telemedicine] explode all trees 2,298
#22 MeSH descriptor: [Remote Consultation] explode all trees 442
#23 Consultation, Remote:ti,ab,kw (Word variations have been searched) 534
#24 Teleconsultation:ti,ab,kw (Word variations have been searched) 480
#25 Teleconsultations:ti,ab,kw (Word variations have been searched) 30
#26 #23 or #24 or #25 964
#27 #22 or #26 974
#28 MeSH descriptor: [Education, Distance] explode all trees 120
#29 Distance Education:ti,ab,kw (Word variations have been searched) 683
#30 Distance Learning:ti,ab,kw (Word variations have been searched) 395
#31 Learning, Distance:ti,ab,kw (Word variations have been searched) 395
#32 Online Learning:ti,ab,kw (Word variations have been searched) 747
#33 Learning, Online:ti,ab,kw (Word variations have been searched) 747
#34 Online Education:ti,ab,kw (Word variations have been searched) 1,412
#35 Education, Online:ti,ab,kw (Word variations have been searched) 1,412
#36 Online Educations:ti,ab,kw (Word variations have been searched) 1,412
#37 Correspondence Courses:ti,ab,kw (Word variations have been searched) 39
#38 Correspondence Course:ti,ab,kw (Word variations have been searched) 39
#39 Course, Correspondence:ti,ab,kw (Word variations have been searched) 39
#40 #29 or #30 or #31 or #32 or #33 or #34 or #35 or #36 or #37 or #38 or #39 2,723
#41 #28 or #40 2,723
#42 MeSH descriptor: [Telenursing] explode all trees 28
#43 MeSH descriptor: [Telephone] explode all trees 3,001
#44 Telephones:ti,ab,kw (Word variations have been searched) 11,766
#45 Switchboard Service:ti,ab,kw (Word variations have been searched) 1
#46 Service, Switchboard:ti,ab,kw (Word variations have been searched) 1
#47 Services, Switchboard:ti,ab,kw (Word variations have been searched) 1
#48 Switchboard Services:ti,ab,kw (Word variations have been searched) 1
#49 #44 or #45 or #46 or #47 or #48 11,767
#50 #43 or #49 12,682
#51 MeSH descriptor: [Cell Phone] explode all trees 1045
#52 Phone, Cell:ti,ab,kw (Word variations have been searched) 968
#53 Phones, Cell:ti,ab,kw (Word variations have been searched) 968
#54 Cellular Phone:ti,ab,kw (Word variations have been searched) 118
#55 Cellular Phones:ti,ab,kw (Word variations have been searched) 118
#56 Phone, Cellular:ti,ab,kw (Word variations have been searched) 118
#57 Phones, Cellular:ti,ab,kw (Word variations have been searched) 118
#58 Telephone, Cellular:ti,ab,kw (Word variations have been searched) 41
#59 Cellular Telephone:ti,ab,kw (Word variations have been searched) 41
#60 Cellular Telephones:ti,ab,kw (Word variations have been searched) 41
#61 Telephones, Cellular:ti,ab,kw (Word variations have been searched) 41
#62 Cell Phones:ti,ab,kw (Word variations have been searched) 968
#63 Portable Cellular Phone:ti,ab,kw (Word variations have been searched) 2
#64 Cellular Phone, Portable:ti,ab,kw (Word variations have been searched) 2
#65 Cellular Phones, Portable:ti,ab,kw (Word variations have been searched) 2
#66 Portable Cellular Phones:ti,ab,kw (Word variations have been searched) 2
#67 Transportable Cellular Phone:ti,ab,kw (Word variations have been searched) 0
#68 Cellular Phone, Transportable:ti,ab,kw (Word variations have been searched) 0
#69 Cellular Phones, Transportable:ti,ab,kw (Word variations have been searched) 0
#70 Transportable Cellular Phones:ti,ab,kw (Word variations have been searched) 0
#71 Mobile Phone:ti,ab,kw (Word variations have been searched) 1,689
#72 Mobile Phones:ti,ab,kw (Word variations have been searched) 1,689
#73 Phone, Mobile:ti,ab,kw (Word variations have been searched) 1,689
#74 Phones, Mobile:ti,ab,kw (Word variations have been searched) 1,689
#75 Mobile Telephone:ti,ab,kw (Word variations have been searched) 294
#76 Mobile Telephones:ti,ab,kw (Word variations have been searched) 294
#77 Telephone, Mobile:ti,ab,kw (Word variations have been searched) 294
#78 Telephones, Mobile:ti,ab,kw (Word variations have been searched) 294
#79 Car Phone:ti,ab,kw (Word variations have been searched) 22
#80 Car Phones:ti,ab,kw (Word variations have been searched) 22
#81 Phone, Car:ti,ab,kw (Word variations have been searched) 22
#82 Phones, Car:ti,ab,kw (Word variations have been searched) 22
#83 #52 or #53 or #54 or #55 or #56 or #57 or #58 or #59 or #60 or #61 or #62 or #63 or #64 or #65 or #66 or #67 or #68 or #69 or #70 or #71 or #72 or #73 or #74 or #75 or #76 or #77 or #78 or #79 or #80 or #81 or #82 2,191
#84 #51 or #83 2,520
#85 MeSH descriptor: [Patient Portals] explode all trees 2
#86 Patient Web Portal:ti,ab,kw (Word variations have been searched) 125
#87 Portal, Patient Web:ti,ab,kw (Word variations have been searched) 125
#88 Portals, Patient Web:ti,ab,kw (Word variations have been searched) 125
#89 Web Portal, Patient:ti,ab,kw (Word variations have been searched) 125
#90 Web Portals, Patient:ti,ab,kw (Word variations have been searched) 125
#91 Patient Internet Portals:ti,ab,kw (Word variations have been searched) 72
#92 Patient Internet Portals:ti,ab,kw (Word variations have been searched) 72
#93 Patient Internet Portals:ti,ab,kw (Word variations have been searched) 72
#94 Patient Internet Portals:ti,ab,kw (Word variations have been searched) 72
#95 Internet Portal, Patient:ti,ab,kw (Word variations have been searched) 72
#96 Internet Portal, Patient:ti,ab,kw (Word variations have been searched) 72
#97 Internet Portals, Patient:ti,ab,kw (Word variations have been searched) 72
#98 Patient Internet Portal:ti,ab,kw (Word variations have been searched) 72
#99 Portal, Patient Internet:ti,ab,kw (Word variations have been searched) 72
#100 Portals, Patient Internet:ti,ab,kw (Word variations have been searched) 72
#101 Patient Web Portals:ti,ab,kw (Word variations have been searched) 125
#102 Patient Portal:ti,ab,kw (Word variations have been searched) 2,945
#103 Portal, Patient:ti,ab,kw (Word variations have been searched) 2,945
#104 #86 or #87 or #88 or #89 or #90 or #91 or #92 or #93 or #94 or #95 or #96 or #97 or #98 or #99 or #100 or #101 or #102 or #103 2,945
#105 #85 or #104 2,945
#106 MeSH descriptor: [Electronic Mail] explode all trees 304
#107 Mail, Electronic:ti,ab,kw (Word variations have been searched) 675
#108 Email:ti,ab,kw (Word variations have been searched) 1,315
#109 Emails:ti,ab,kw (Word variations have been searched) 1,315
#110 E-Mail:ti,ab,kw (Word variations have been searched) 1,614
#111 E Mail:ti,ab,kw (Word variations have been searched) 1,846
#112 E-Mails:ti,ab,kw (Word variations have been searched) 1,614
#113 #107 or #108 or #109 or #110 or #111 or #112 2,847
#114 #106 or #113 2,847
#115 wechat:ti,ab,kw (Word variations have been searched) 30
#116 qq:ti,ab,kw (Word variations have been searched) 24
#117 QQ:ti,ab,kw (Word variations have been searched) 24
#118 #116 or #117 24
#119 MeSH descriptor: [Television] explode all trees 1,508
#120 Televisions:ti,ab,kw (Word variations have been searched) 909
#121 #119 or #120 2,084
#122 MeSH descriptor: [China] explode all trees 4,011
#123 People's Republic of China (Word variations have been searched) 817
#124 Mainland China (Word variations have been searched) 250
#125 Manchuria (Word variations have been searched) 1
#126 Sinkiang (Word variations have been searched) 4
#127 Inner Mongolia (Word variations have been searched) 94
#128 #123 or #124 or #125 or #126 or #127 1,149
#129 #122 or #128 4,973
#130 MeSH descriptor: [Hong Kong] explode all trees 619
#131 Hongkong (Word variations have been searched) 47
#132 Kowloon (Word variations have been searched) 326
#133 New Territories (Word variations have been searched) 625
#134 #131 or #132 or #133 992
#135 #130 or #134 1,547
#136 MeSH descriptor: [Taiwan] explode all trees 981
#137 Republic of China (Word variations have been searched) 4,121
#138 Formosa (Word variations have been searched) 35
#139 #137 or #138 4,155
#140 #136 or #139 5,025
#141 MeSH descriptor: [Macau] explode all trees 4
#142 Macao (Word variations have been searched) 32
#143 #141 or #142 35
#144 #20 or #27 or #41 or #42 or #50 or #84 or #105 or #114 or #115 or #118 or #121 25,692
#145 #129 or #135 or #140 or #143 9,981
#146 #12 and #144 and #145 4
#147 #146 4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.