
Abstract
Background:
Access to dermatologists is limited for disadvantaged patients, who may receive suboptimal dermatologic care from nonspecialists. We assessed if teledermatology could improve primary care provider (PCP)-delivered care for cutaneous disease at a clinic serving uninsured patients.
Materials and Methods:
Utilizing the American Academy of Dermatology's free AccessDerm program, we offered store-and-forward teledermatology to PCPs, who initiated consultations at will during clinical care independent of the study. We retrospectively analyzed all consultations from 2013 to 2017 and collected patient age/sex, teledermatologist diagnosis, time to teledermatologist reply, time to next dermatology appointment, as well as PCP- and teledermatologist-proposed care plans.
Results:
Retrospective analysis of 131 consults revealed a 37-h mean teledermatology response-time versus a 14-day appointment wait (p < 0.00001). Teledermatologists provided a definitive care plan without in-person evaluation for 82 (65%) of completed consults and recommended interim treatments while awaiting appointments in 15 cases, thus accelerating care plan delivery in 97 cases (76%). The triage decision rate differed among diagnostic categories; deferral to in-person evaluation was more frequent for neoplasms (p < 0.0001). When PCPs specified preconsult treatment plans, 82% differed from teledermatologist-advised management. Following teledermatologist recommendations would have changed the clinical course in 70% of cases, potentially avoiding suboptimal care, including inappropriate corticosteroids, antimicrobials, and emergency room referrals.
Conclusions:
We found teledermatology can effectively guide PCPs in resource-limited settings by accelerating delivery of dermatologist-recommended care plans for uninsured patients. Expanding teledermatology for PCPs in under-resourced clinics has the potential to improve treatment of cutaneous disease by nonspecialists and to mitigate suboptimal care for disadvantaged patients.
Introduction
Although cutaneous concerns are a frequent reason for visiting a health care provider, 1 –3 including in charitable clinics, 4 patient access to dermatologists is limited in the United States and this disproportionately affects impoverished, uninsured, and underinsured patients. 5,6 These disadvantaged populations are thus more likely to receive treatment for cutaneous disease from nondermatologist primary care providers (PCPs), which may result in suboptimal outcomes. Teledermatology has emerged as a viable strategy to reduce this health care disparity in under-resourced clinics lacking timely and reliable access to dermatologist consultation. 7 The value of specialist input in these settings has been highlighted in studies showing that PCP- and teledermatologist-proposed diagnoses and treatments for cutaneous concerns differ significantly. 8,9
Prior studies have demonstrated that teledermatology outreach programs allow remote dermatologists to guide PCPs caring for vulnerable patients who would otherwise not receive specialist-level care. 8 –13 In fact, use of teledermatology has improved PCP knowledge of dermatologic conditions 14 and accelerated care delivery, 15 and could improve patient quality of life. 16 Moreover, teledermatology outreach can have a significant economic impact by avoiding more costly means of obtaining dermatologic care, such as through emergency room (ER) visits. 17
The goal of our study was to determine if teledermatology consultation could optimize PCP-delivered care for patients lacking access to dermatologists with a focus on its potential to mitigate suboptimal treatments. To that end, we assessed a volunteer academic teledermatology outreach partnership with Puentes de Salud (“Bridges of Health” in English), an urban community health clinic serving exclusively uninsured patients. 8 Utilizing the American Academy of Dermatology (AAD) AccessDerm store-and-forward teledermatology platform, we retrospectively analyzed PCP consultations from Puentes de Salud to measure the potential impact of remote dermatologist input on time-to-care and management plans for cutaneous disease.
Materials and Methods
Clinical Setting and Teledermatology Workflow
All PCPs working at Puentes de Salud were offered free and voluntary enrollment in the AAD Health Insurance Portability and Accountability Act-compliant store-and-forward teledermatology platform, AccessDerm (supported during the study period by Vignet Corporation, Fairfax, VA). Enrollees were provided a one-time in-person tutorial or a PowerPoint file explaining its use. AccessDerm could be used by PCPs to submit consultations either through a smartphone application or a web-based platform. The teledermatology electronic consult form prompted PCPs to provide patient age, sex, a focused history of the dermatologic concern, and photographs of the patient's physical exam findings (uploaded through personal devices, most commonly a camera-equipped mobile telephone). No other identifying patient information was collected. Optionally, PCPs were asked to provide their own differential diagnosis and treatment plan before receiving teledermatologist advice, including whether the patient would be referred to an ER or urgent care facility in the absence of teledermatology consultation.
All PCP-submitted consults were reviewed by one of several remote volunteer board-certified dermatologists at the University of Pennsylvania. Upon receiving an e-mail notification for each new consult, the first available teledermatologist would claim the consult and provide a reply as time permitted with the sole purpose of directing patient care independent of the study. Teledermatologists were prompted to provide a diagnosis and a treatment plan, including a recommendation regarding whether the patient required in-person evaluation by a dermatologist, which was scheduled during the next monthly specialty clinic at Puentes de Salud.
Study Design, Data Collection, and Analysis
With approval from the University of Pennsylvania Institutional Review Board, we retrospectively analyzed a case series of all teledermatology consults (N = 131) received from Puentes de Salud between January 2013 and November 2017. Teledermatology consults were considered complete if (i) the PCP uploaded at least one photograph and (ii) the teledermatologist provided any plan of care. Extracted data for each completed consult included patient age and sex, time of consult submission, time of consultant reply, as well as PCP- and teledermatologist-proposed diagnoses and treatment plans. These data were used to calculate the mean and median time-to-reply for teledermatology consults versus the wait time for the next dermatology clinic as recorded in the Puentes de Salud clinical schedule; paired values were compared using the Wilcoxon signed-ranked test.
The average deferral rate for all consults was calculated based on the number of completed cases in which teledermatologists recommended in-person evaluation. The number of deferrals and nondeferrals was calculated for neoplasms versus non-neoplasms and compared using a Fisher's exact test. The reason for in-person evaluation was determined from the teledermatologist plan as either due to diagnostic uncertainty (recommended in-person visualization before rendering a diagnosis or treatment) or specified requirement for a nonelective procedure that would normally be performed in the dermatology clinic (e.g., lesion biopsy, destruction). Teledermatology was deemed to accelerate care delivery if either (i) a definitive plan of care was rendered by the teledermatologist or (ii) any interim plan of care was recommended by the teledermatologist to be initiated by the PCP while the patient awaited a dermatology appointment.
For each case in which a treatment plan was specified by the PCP (N = 72), C.L.S. categorized the PCP-submitted plan of care based solely on comparison to the teledermatologist-recommended treatment plan as recorded in AccessDerm. PCP plans were considered to be different from that of the teledermatologists if they either (i) included any specific treatment/plan that was not recommended by the teledermatologist or (ii) excluded any specific treatment/plan that was recommended by the teledermatologist. Example PCP plans considered to be undertreatment failed to include treatment for a suspected infection, a sufficiently potent topical corticosteroid, a systemic agent for inflammatory acne, a preferable topical agent, or a specialty referral when any of these was specifically recommended by the teledermatologist. Example PCP plans considered to be overtreatment included an antibiotic, an antiviral agent, an antifungal agent, or a corticosteroid, when any of these was not specifically recommended by the teledermatologist.
The study (Protocol 832136) was approved by the University of Pennsylvania Institutional Review Board.
Results
Teledermatology can be Used to Guide PCPS in an Under-Resourced Clinic
To improve access to dermatologist consultation in a primary care clinic serving disadvantaged patients, we previously partnered with PCPs at Puentes de Salud, a nonprofit community health clinic that cares exclusively for uninsured patients, many of whom are Latino immigrants facing various barriers to health care. 8 PCPs were offered enrollment in AccessDerm to submit teledermatology consultations at will during their normal course of clinical care (see section “Materials and Methods”). A group of volunteer board-certified dermatologists replied to consults to guide PCPs independent of the study.
To determine the feasibility of utilizing store-and-forward teledermatology in this setting, we retrospectively analyzed all teledermatology consults from Puentes de Salud during the study period (Fig. 1). Among all submitted consults (N = 131), we found a completion rate of 97% in which teledermatologists received enough historical and photographic information to provide a reply. This indicates that after minimal instruction, PCPs were able to successfully use the AccessDerm platform. Only four cases (3%) were deemed technical failures; all were due to photograph omission during early program implementation, which prohibited teledermatologists from providing any specific guidance.
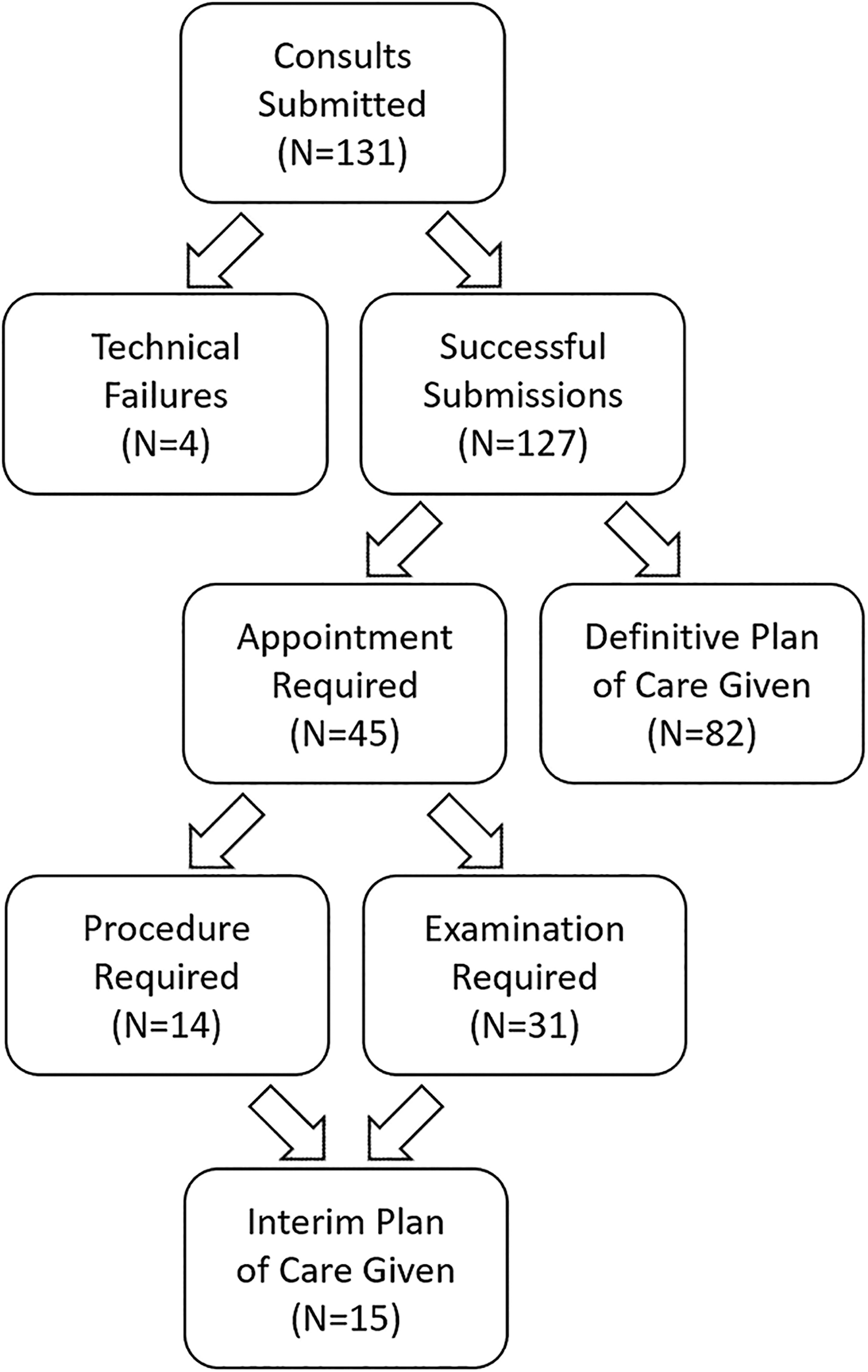
Teledermatology consult handling.
Teledermatology Consultations Revealed Diverse Cutaneous Concerns from Uninsured Patients
Patients included in our series of 131 cases were 63% male and were on average 31.7 years old (range 1–92). All lacked health insurance, which is a requirement to be cared for at the Puentes de Salud Clinic. To characterize the nature of the cutaneous concerns driving teledermatology consultation, each of the completed consults (N = 127) was categorized based on the teledermatologist-proposed diagnosis (Table 1). The most prevalent diagnostic category was inflammatory (43%, 55/127), which included acneiform, eczematous, and psoriasiform eruptions. Nonpigmented neoplasms (20%, 25/127), such as suspected pyogenic granulomas or pilar cysts, were more common in this patient population than pigmented lesions (6%, 7/127), for which teledermatology may provide limited diagnostic capability without teledermoscopy equipment that may be available in better-resourced primary care clinics. 18,19 Infectious skin diagnoses (18%, 23/127) were most often suspected fungal or viral infections like tinea or verrucae, whereas hair disorders (7%, 9/127) included alopecia areata and acne keloidalis nuchae.
Teledermatology Consult Characteristics
SD, standard deviation; IQR, interquartile range.
Teledermatology can Accelerate Delivery of Specialist-Recommended Care for Patients Lacking Access to Dermatologists
We assessed whether PCP-generated teledermatology consultations were sufficient to allow remote dermatologists to provide specific treatment plans based on the provided history and photographs (Fig. 1). Of completed consultations, teledermatologists determined that in 65% (82/127) of cases, in-person evaluation was not initially required and a definitive plan of care was delivered to the PCP through remote consultation alone. Even if teledermatologists could not render a definitive plan of care, they were able to recommend an interim treatment, which could be initiated immediately by the PCP in 33% (15/45) of cases referred for an in-person appointment. Thus, in total, teledermatology accelerated the delivery of a dermatologist-recommended plan of care for 76% (97/127) of patients in this study.
Among the 35% (45/127) of cases referred for an in-person appointment, the reasons driving this decision were diagnostic uncertainty necessitating examination (24% of all cases, 31/127) or requirement for a nonelective procedure (11% of all cases, 14/127) such as a lesion biopsy or destruction. The rate of deferral to in-person evaluation differed based on the category of the diagnosis that was rendered by the teledermatologist (Table 1). While teledermatologists recommended in-person examination of 71% of pigmented neoplasms and 64% of nonpigmented neoplasms, only 11% of hair disorders and 24% of inflammatory eruptions necessitated a dermatologist appointment. In particular, the difference between the deferral rate of 66% (21/32) for all neoplasms versus 25% (24/95) for non-neoplasms was statistically significant (p-value <0.0001, Fisher's exact test) (Table 2). This suggests teledermatology can more often obviate the need for in-person evaluation for non-neoplastic dermatologic concerns.
Teledermatology Timing and Deferral Rate
SEM, standard error of the means.
In the absence of teledermatology, all patients would have waited until the next in-person dermatology clinic to obtain specialist input. To quantify the potential impact of teledermatology on the time-to-care for patients, we calculated the average time-to-reply for teledermatology consults and compared this with the average wait time for the next in-person appointment at the Puentes de Salud monthly dermatology clinic (Table 2). The mean teledermatology response time of 1.6 days (37.4 h ± standard error of the mean [SEM] 7.7) was significantly shorter than an appointment wait time of 13.9 days (333.1 h ± SEM 20.6) (p-value <0.00001, Wilcoxon signed-rank test). By using teledermatology consultation, the mean reduction in wait time for dermatologist input was 12.3 days (296 h ± SEM 22).
Teledermatologist Management Differs from Nonspecialists and may Mitigate Suboptimal Care
In submitting a consult, PCPs were asked to provide their proposed plan of care for the patient if teledermatology had not been available. In comparison to specific PCP-reported preconsult treatment plans (N = 72), teledermatologist-recommended plans differed in 82% (59/72) of cases, emphasizing the value of specialist input for the management of cutaneous disease. In the remaining cases (N = 55), PCPs offered no specific plan or simply stated they would refer to dermatology.
Analyzing all completed cases (N = 127), we found that implementing the recommendations that were delivered through teledermatology would have led to a significant change in the patient's course of care in 70% (89/127) of cases. We further characterized the potential suboptimal outcomes that would have occurred in those 89 cases if the PCP-proposed plan (including awaiting a dermatology appointment without any interim treatment) had been followed in the absence of specialist-level advice provided through teledermatology (Table 3). We categorized PCP-proposed plans as undertreatment in 27% (34/127) of cases; examples included omitting treatment for a suspected infection, a sufficiently potent topical corticosteroid, or a systemic agent for inflammatory acne. On the other hand, we deemed PCP-proposed plans overtreatment in 11% (14/127) of cases; examples included unnecessary use of oral antibiotics, antifungal agents, or systemic corticosteroids.
Primary Care Provider Versus Dermatologist Plan Outcomes
PCP, primary care provider; ER, emergency room.
In 26% (33/127) of cases, the patient's receipt of a care plan would have simply been delayed in the absence of teledermatology. In those cases, the PCP plan was to refer to the dermatology clinic but the teledermatologist either (i) advised an interim treatment that could be initiated immediately or (ii) provided more rapid delivery of reassurance that a condition was benign. In the latter cases, teledermatology allowed the clinic to better allocate its limited specialist appointments to those patients truly in need of in-person evaluation by a dermatologist. Finally, we assessed if the proposed disposition for the patient may have been altered by utilizing teledermatology. In eight cases (6.3%), PCPs indicated they would have referred the patient to an ER or urgent care facility in the absence of teledermatology consultation. These results emphasize the potential of teledermatology to have a positive impact on health care resource utilization for cutaneous disease.
Discussion
Ubiquitous camera-equipped smartphones offer the ability to deliver high-quality photographs to remote dermatologists, who can review images and provide clinical advice to PCPs with good diagnostic accuracy and high user satisfaction. 11,20 –23 This technology has the potential to accelerate the delivery of dermatologist advice to nonspecialists caring for disadvantaged populations and could mitigate suboptimal treatment of cutaneous disease. Accordingly, we found that teledermatologist-recommended treatment plans differed significantly from those proposed by PCPs and, if followed, would have altered management for the majority of patients. In fact, following the teledermatologist-recommended plan could have led to significant improvements in clinical care, including more judicious use of antimicrobial agents and avoidance of acute care referrals. Our study demonstrates how store-and-forward teledermatology consultation can be implemented to support PCPs working in under-resourced clinics, who often have limited access to specialists. We also found that teledermatology could be used as a triage mechanism to reduce the number of patients requiring in-person evaluation and could significantly shorten the queue of patients awaiting dermatology appointments, which can become quite long at volunteer-run specialty outreach clinics.
While the size and specific setting of our study may limit its generalizability, our partnership with Puentes de Salud also provides important insight into the cutaneous diseases seen in clinics serving uninsured patients, particularly those of Latino ethnicity. Although race and ethnicity data were not specifically collected in our study, the availability of Spanish-speaking medical staff and Spanish-focused community outreach programs at the Puentes de Salud Clinic certainly enhanced the representation of Latino patients in our case series and influenced the distribution of diagnoses. Prior investigation has revealed that the Latino population in the United States faces numerous barriers to seeking and obtaining health care in the United States, including costs, legal status, transportation, discrimination, and language. 24 –27 While previous studies have reported the particular dermatologic issues facing Latino workers in rural areas, mostly in agricultural environments, 26,28,29 our teledermatology partnership with Puentes de Salud PCPs allowed us to assess dermatologic consultations originating from an inner city community health clinic with a particular focus on serving the urban Latino community.
Our study drew from a partnership with a community health clinic located in an urban setting, but expanding access to specialist input through teledermatology platforms can also help remedy the paucity of dermatologists working in rural areas. 30,31 In fact, prior studies have demonstrated that teledermatology outreach programs similar to ours have increased access to specialist-level care in rural areas of the United States 32,33 and in remote areas of resource-limited countries, 34 –36 where travel to see urban specialists in-person can be especially challenging. Moreover, while our mean wait for an in-person dermatologist evaluation was 14 days at our on-site volunteer clinic, this underestimates the wait time in the United States, where the average wait for a new patient dermatology visit was found to be more than a month. 37 The resultant delay in care further underscores the potential value in utilizing teledermatology programs such as ours to triage dermatologic consults to help prioritize patients with more urgent cutaneous eruptions or lesions, which require expedited specialist referrals.
In sum, we have shown that volunteer teledermatology consultation programs such as ours can effectively deliver much needed specialist-level advice to PCPs caring for uninsured populations, who commonly present with cutaneous concerns. Scalability and sustainability of teledermatology outreach, especially when volunteer-dependent, can be logistically challenging, although multiple groups have outlined strategies for expanding teledermatology programs. 38,39 In addition to AccessDerm, the Dermatology Extension for Community Healthcare Outcomes (ECHO) program 40,41 in the United States and various international collaborative networks 42 –44 have successfully expanded PCP access to specialist advice through electronic consultation with off-site dermatologists. Through its website,* the AAD is actively engaging and enrolling PCPs who work in clinics serving patients with limited access to dermatology to pair them with volunteer teledermatologists licensed in their State and to train them in the use of the free AccessDerm platform. We hope our results will encourage participation in teledermatology outreach efforts, which have the potential to expand access to dermatologist advice for disadvantaged patients who would not otherwise receive specialist-level care and could ultimately help reduce health care disparities in dermatology.
Footnotes
Acknowledgments
The authors thank all current and former volunteer teledermatologists at the University of Pennsylvania who answered the consultations included in this study. They thank Dr. Carrie Kovarik, MD, for insightful review of the article. As well, the authors are grateful to the American Academy of Dermatology for its support of the AccessDerm program, which was used in this study.
Disclosure Statement
No competing financial interests exist.
Funding Information
C.L.S. was supported by a Career Development Award from the Dermatology Foundation. A.N.H. was supported by the Diversity Mentorship Program of the American Academy of Dermatology.