
Abstract
Background:
Online health communities (OHCs) are one of the developments related to online health. Patient compliance plays a vital role in improving health treatment outcomes. Patient activation is associated with patient activities in OHCs, such as physician–patient communication and health information seeking. In other words, OHCs influence patient compliance. Therefore, identifying the relationship between patient activation in OHCs and patient compliance is important for improved health outcomes.
Methods:
This study established a research model consisting of one independent variable (patient activation), four mediators (physician–patient communication, health information seeking, perceived information asymmetry, and e-health literacy), one dependent variable (patient compliance) and four control variables (gender, age, education level, and status). Data were obtained through a web-based survey, involving a total of 387 valid participants in China. These data were analyzed and tested through structural equation modeling and partial least squares.
Results:
Patient activation positively affects patient compliance through the mediation of physician–patient communication, health information seeking, perceived information asymmetry, and e-health literacy. Perceived information asymmetry has no direct effect on patient compliance. However, perceived information asymmetry affects patient compliance through the mediation of e-health literacy.
Conclusions:
Patient compliance is significantly affected by patient activation. Thus, physicians can achieve higher patient compliance by improving patient activation. Guaranteeing and improving the information quality in OHCs is essential for physicians and OHCs operators. Physicians should pay extra attention in cultivating patients' e-health literacy through communications and health information-seeking behaviors to further improve patient compliance.
Introduction
In these modern times, the need for medical and treatment-related information is rapidly increasing, given the alarming need for improvement of living quality and health literacy. 1 The drastic development of the internet provides a wide range of technological possibilities for online health-related actions. 2 Specifically, the internet aids in boosting the growth of online health communities (OHCs). OHCs are platforms for health consumers and patients to discuss different diseases, therapeutic regimens and personal experiences. 3 Then, OHCs utilize the accumulated health care knowledge to widen its influence. 4 In OHCs, patients can discuss their experiences and medical conditions freely without worrying about embarrassment and other similar apprehensions.
Although OHCs provide abundant medical information, locating information remains challenging for consumers because of information overload. 3 This information overload is continually experienced, especially of those people who are not skilled or expert in searching online medical information. Determining the exact information the consumers seek is relatively difficult for those who lack complete understanding of their health conditions due to the absence of medical knowledge. 5 Moreover, nontechnical language utilized by users impedes the effectiveness of information searching. 6 Therefore, facilitating the patients' access to their desired online health information is imperative and crucial.
Patient compliance is defined as how patients follow medical diagnoses and treatment regimens recommended by their physicians. 7 Social support is confirmed to enhance the outcomes of medical treatment by improving patient compliance. 8 People with higher rates of compliance will most likely find a cure to their diseases or experience a better health situation. 9,10 By contrast, noncompliance increases when practitioners' perceptions of the patients' prognosis or efficacy differ from patients' perception. 11 As one of the greatest challenges in the therapeutic process, noncompliance can lead to waste or inefficiency of some treatments, 11 and even lead to treatment failure. 12 Therefore, identifying the manner, in which patient compliance can be increased, is important to improve patients' health outcomes.
Patient activation is defined as patients' motivation and involvement in managing health-related needs. 13 Activated patients represent people who have confidence and motivation to manage their health with effective decisions. 14 According to Hibbard et al., patient activation has a valid and reliable measurement called patient activation measure (PAM). This measurement involves four aspects, namely believing in the importance of patient roles, necessary confidence and knowledge for actions, taking actions for health, and preserving even under pressure. 13 Thus, PAM is a comprehensive indicator related to patients' beliefs, confidence, knowledge, and self-management of health and health care. 15
Social information processing theory implies that mental steps always take place before individuals respond to social cues by behavior. 16 –18 The theory indicates that patients' aspiration is important for their actions. Moreover, the results of higher activation indicate better self-care, less emotional distress, healthier behavior, lower health costs, and better health outcomes. 19 –29 Thus, patient activation is valuable in studying the desired therapeutic effect further. However, existing studies on the influence of patient activation on patient compliance are limited. Thus, determining an approach that increases patient compliance is necessary to guarantee an improved treatment outcome.
Nevertheless, the relationship between patient activation and patient compliance is indirect. Thus, the current study aims to identify the mediators in the existing relationship between patient activation and patient compliance. Hibbard et al. found that engaged patients are curious about their health situation and feel accountable concerning their health care; thus, they may pay additional attention to information related to their health situation. 18 The information can be obtained from two approaches, namely physician–patient communication and online information searching, especially through the OHCs. 30,31 Thus, physician–patient communication and health information-seeking behavior may be considered mediators in the relationship between patient activation and patient compliance.
Moreover, relative articles on the direct relationship between physician–patient communication and patient compliance or between health information seeking and compliance are limited. Thus, the mediators require further exploration. Communicating with physicians is a traditional and critical way for patients to gain knowledge related to their health situations. 32 Communication can narrow the knowledge gap between physicians and patients. Consequently, a decrease in information asymmetry becomes possible. Information asymmetry is considered a mediator between physician–patient communication and patient compliance. The knowledge obtained during communication can also improve the ability of addressing health problems related to e-health literacy. 28 e-Health literacy is defined as the ability to solve health problems by seeking and understanding health information online. 33 Thus, e-health literacy can be improved through physician–patient communication. Therefore, e-health literacy is also considered a mediator between physician–patient communication and patient compliance.
Online information-seeking behavior can affect physician–patient relationship, which is one of the critical parts of the connection. 34,35 However, seeking information online has complex influence on patient compliance. For example, seeking information online enables the acquisition of health knowledge (i.e., information asymmetry). 36 Likewise, patient compliance can be enhanced because information asymmetry can help patients feel their physicians' reliability and competence. 37 Therefore, information asymmetry is considered a mediator between health information seeking and patient compliance. Health information-seeking behavior can also improve patients' abilities to use digital devices and gain health knowledge. Therefore, health information seeking improves e-health literacy. 36 High e-health literacy implies that patients have the ability to identify correct online information that is consistent with their physicians' advice. Consequently, patients will be compliant with their physicians' prescriptions. Thus, e-health literacy is considered a mediator between health information seeking and patient compliance.
According to social information processing theory, people's behavior can be affected by social information, which may build people's opinions and beliefs. 38 As for physician–patient relationship under OHC circumstance, patients' views and feelings on health information and their physicians can affect the response enactment of treatment. In this study, we can rigorously examine the patient–physician relationship by applying the social information processing theory. Thus, on the basis of this theory, we aim to explore the internal mechanism of improving patient compliance by patient activation. Moreover, we use physician–patient communication, health information seeking, perceived information asymmetry, and e-health literacy as mediators in the relationship between patient activation and patient compliance to determine the association between patients' activation and compliance.
Research Model and Hypotheses
Figure 1 shows the research model describing how patient activation can influence patient compliance. Based on the discussion in session 1, although other factors may be involved in compliance, the following four sections should be the focus of this study: physician–patient communication, health information seeking, perceived information asymmetry, and e-health literacy. The independent variable is patient activation, and the dependent variable is patient compliance. The mediators are physician–patient communication, health information seeking, perceived information asymmetry, and e-health literacy.

Research model. H, hypothesis.
Two main approaches are available for acquiring health information, that is, by communicating with physicians and by seeking health information online. 30,31 Maloney et al. found that patients prefer to discuss health information related to therapies and treatments with their physicians. 39 Patients' active attitudes have been found to be critical in promoting communication with their physicians. 40 Thus, patient activation considerably enhances the effects and effectiveness of physician–patient communication. 32 In other words, if patients have adequate activation, then they will communicate often with their physicians.
On the basis of social information processing theory, when the information is insufficient, individuals will seek information from their immediate social environment. 41 Specifically, when people are curious and active about their illness, they will search health information online to gain sufficient knowledge. Consequently, health information-seeking behavior will meet patients' demands for health information. 7 In conclusion, people are willing to seek information when they are proactive on their health conditions. Hence, we propose the following hypotheses:
Iverson et al. claimed that patients pay more attention to their physicians' advice than any other source of information. 42 Hence, patients can engage with physicians on specific health topics via OHCs to promote interactions with one another. 43 Furthermore, communicating with physicians is the primary and traditional method of obtaining health information. 44 –46 Specialists even tend to set institutional arrangement to make the benefits of expert medical knowledge widely available to solve information asymmetry. 47 Patients can acquire health information from physicians during communication, which will enrich patients' knowledge. 32 Then, a narrowing gap of health knowledge is anticipated between patients and physicians. Consequently, patients will perceive less asymmetry. On this basis, we derive the following hypothesis:
Health and computer literacies are the two main components of e-health literacy. 48 With the development of the internet, web-based health platform breaks the time and space limitation for patients to communicate with physicians in real-time. The quality of physician–patient communication is regarded as one of the critical components of health literacy. 49 If patients gain sufficient information related to their illness during the communication, then physicians can improve patients' health literacy. Moreover, Atanasova et al. stated that physicians communicating with patients can increase the possibility of using health services. 50 Furthermore, people also wish to search health data details on the website after visiting their physicians. 45,46 Accordingly, computer literacy can be improved through exposure and practice of digital devices. Consequently, patients not only can improve their health literacy but also their computer literacy. In other words, e-health literacy can be enhanced comprehensively through physician–patient communication. Thus, we assume the following:
Information retrieval and browsing are two kinds of purposeful activities of information-seeking behavior that target specific requirements. 51 Patients can gain additional health information related to their medical condition apart from those provided by their physicians. 52 Therefore, patients can gain information about their illnesses during information seeking. Then, information asymmetry perceived by patients will lessen. The central premise of the hypothesis is that the health information sought by patients must be true. Research shows that low-quality information will confuse patients and may lead to a negative effect on physician–patient relationship. 39,53
Using the internet to seek health information frequently is an important predictor of high e-health literacy. 54 In other words, frequently seeking online health information is a critical and positive predictor of e-health literacy. This phenomenon is explained by the fact that searching health-related information online can improve one's ability to solve problem via electronic devices. 55 Seeking health information online is a basic and functional process for applying useful information to address various health problems. 49 Moreover, solving health problems through the information obtained from searching online is a crucial indicator of high e-health literacy. 49 Even in some instances, patients with some less serious illnesses can determine cure for themselves depending on the online health information they sought. 56 Therefore, online health information seeking may have a positive effect on building e-health literacy and medication adherence. 57 This argument leads to the following hypotheses:
Pavlou et al. reported that perceived information asymmetry implies that physicians have a larger quantity and/or quality of information than their patients. 58 Solem et al. indicated that forming an understanding of the knowledge gaps between physicians and patients is critical to improve patient compliance. 59 As for patients, the competence and reliability of their physicians can be built through information asymmetry. On this basis, patients will feel that they are obliged to follow the physicians' medical diagnosis and treatment. 60 Consequently, patients will trust information provided by their physicians and obey strictly their physicians' advice. Thus, we propose the following hypothesis:
The internet provides accessibility for patients to seek information related to their treatment online, and this action may have an influence and affect the relationship between physicians and patients. 61 For example, if patients can determine high-quality health information fitted with physicians' advice online, then they will gain awareness about treatments and realize that the physicians are competent about their diseases. 62 Consequently, a reduction in disagreements, conflicts, and biased speculations may arise. 37 Patients can comply when they have a certain level of understanding of their diseases and health care regimens. 63
On the basis of social information processing theory, the reaction and behavior of employees' in the management industry are influenced not only by information but also by employees' comprehensive abilities. 64 When the theory is applied to physician–patient relationship, accepting that patients' abilities to process information can influence the their reactions to their physicians' advice is reasonable. Therefore, if patients have adequate e-health literacy, then they will find meaningful and useful information online. This action has a positive effect on patient–physician relationship. Hence, we propose the following hypothesis:
Materials and Methods
Instrument Development
The current study measured variables in the research model by utilizing a 5-point Likert response format validated by published works, ranging from strongly disagree to strongly agree. We adopted the scales used in published works to establish reality and validity. We adopted a 13-item scale from Hibbard et al. 65 to measure patient activation and a 14-item scale used by Makoul et al. 66 to assess physician–patient communication. Health information-seeking behavior was examined by utilizing a 4-item scale from Maryam et al. 67 We also adopted a 4-item scale used by Laugesen et al. 7 to measure perceived information asymmetry. By combining the studies of Norman and Skinner 68 and Park and Lee, 69 e-health literacy was measured with a 10-item scale. Patient compliance was measured using a 5-item scale adopted from Laugesen et al. 7
Analysis Tool Selection
Structural equation modeling (SEM) was used to test in testing our hypotheses to examine the complex relationships of the research model and the individual effect on dependent variables. SEM incorporates the measurement error and detect effects. 70 This study adopted the partial least squares (PLS)–SEM method because the research model is complex and the sample size can be small. 71 We used SmartPLS® version 3 (SmartPLS GmbH, Bönningstedt, Germany) to analyze the collected data and test our hypotheses. SmartPLS version 3 was selected because it can cope with highly complex models, achieve efficient and unbiased analysis, and evaluate the latent variable interactions.
Data Collection and Respondents' Profile
All subjects of this survey were Chinese individuals who had searched for information in different OHC platforms or communicated with their physicians within the previous month to ensure that they could recall their related experiences. Before starting the survey process, we translated the survey instrument into Chinese. The survey would be investigated in China. Thus, the participants were Chinese individuals, and the content of the survey should be written in Chinese.
First, similar to the translation process in previous works, 72,73 for the consideration of cross-cultural adaption, 74 we recruited native Chinese speakers with master's degree or above who could speak English fluently and were proficient in scientific research translation in converting our scales into Chinese. Second, we invited experienced individuals with different age levels, gender, and educational qualifications to fill in the questionnaire and provide suggestions to improve the scales. Third, we enhanced the comprehending capacity, conciseness, appropriateness, and readability of scales. Finally, we performed a reverse-translation process that guaranteed the similarity of our scales to the original English version in the conceptually consistent section. 75
The investigation was conducted in December 2018. The response completion time which that is considerably lower than the average time was considered invalid. Incomplete responses or at least missing an answer were also considered invalid. Following these conditions, we received a total of 463 responses, among which 387 were considered valid. The validity rate was 80.0% (387/463). The characteristics of OHC users were young, female, and highly educated. 76 Table 1 shows the demographics of the sample. We found that 59.2% (229/387) of the participants were aged from 20 to 40 years, 52.7% (204/387) were female, and 52.5% (203/387) held at least a bachelor's degree. More than half of our sample was young, female, and highly educated. Such characteristics were consistent with those of OHC users. Therefore, the sample met our requirements.
Sample Demographics (n = 387)
Results
Data Analysis
We used previously validated scales to measure variables, thereby rendering the reliability and validity acceptable. The reliability was recalculated by Cronbach's alpha because the research background and the sample object were different. The Cronbach's alphas (needed to be greater than 0.70075) of several constructs in Table 2 show that the reliability of scale in this study was acceptable.
Cronbach's Alpha of the Constructs
Hypothesis Test
The demographical statistics were used to identify the effects of demographic factors. We added gender, age, education level, and status as control variables into the research model. On the basis of the multivariate coefficient of determination results shown in Table 3, the values were among 0.600 to 0.800. These figures implied that each item exhibited acceptable significance level (small: 0.19; medium: 0.33; large: 0.67). Moreover, Cohen ƒ 2 was used to assess the effects of the control variables (i.e., insignificant: <0.020; small: ≥0.020 and <0.150; medium: ≥0.150 and <0.300; and large: ≥0.350). The effects of control variables were limited because the gap between those with control variables and without control variables was small.
Multivariate Coefficient of Determination (R 2 ) Results
ΔR 2 : R 2 with control variables − R 2 without control variables.
Cohen ƒ 2 .
EHL, e-health literacy; HIS, health information seeking; PC, patient compliance; PIA, perceived information asymmetry; PPC, physician–patient communication.
Table 4 and Figure 2 present the magnitude and significance of path coefficients, respectively. H1, H2, H4, H6, H7, and H8 were supported because the magnitude and significance were acceptable. However, H3 and H5 were not supported because the algebraic sign of influences was inconsistent with the original hypotheses. Our results indicated that physician–patient communication had a positive impact on perceived information asymmetry. Likewise, health information seeking had a positive impact on perceived information asymmetry. The next section provides explanations for these insignificant relationships.
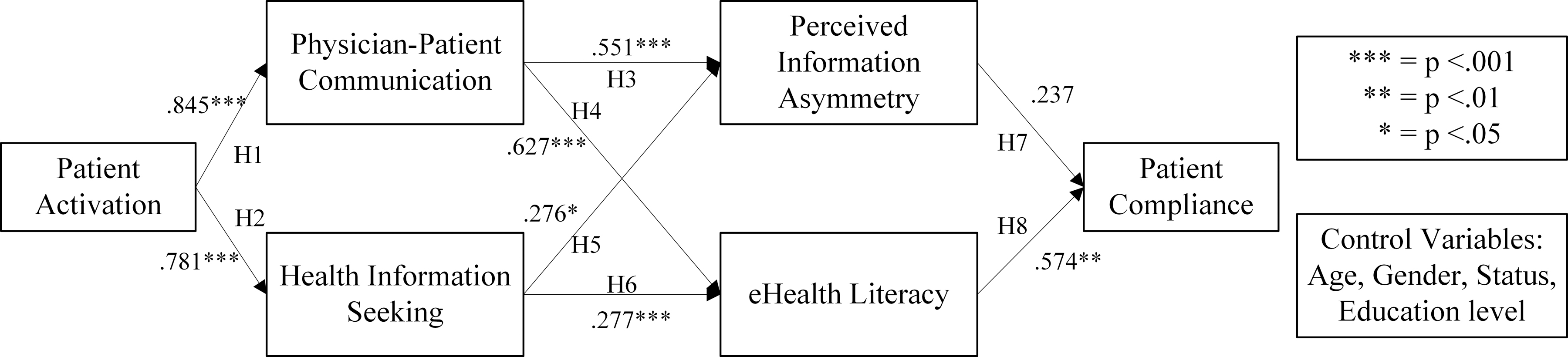
Research model with path coefficients and significances.
Hypothesis Testing
P < .05; ** P < .01; *** P < .001.
Table 5 shows the effect size of each constructs in the research model. Patient activation had a strong influence with large effect sizes on physician–patient communication and health information seeking. e-Health literacy could be significantly affected by the physician–patient communication and be insignificantly affected by health information seeking. Moreover, the effects of physician–patient communication and health information seeking on perceived information asymmetry were moderate and weak, respectively. Furthermore, the impact of e-health literacy on patient compliance was moderate, whereas the impact of the perceived information asymmetry was weak.
Partial Least Squares Effect Size Analysis
Discussion
Principal Findings
This study explores the relationship between patient activation and patient compliance due to limited related studies. It provides understanding on the advantages of patient activation. This study also guides physicians and medical practitioners on how to make use of patient activation to improve patient compliance. Previous studies have focused on the effect of patient activation and the advantages of high patient compliance. 22 –29 However, studies on the relationship between patient activation and patient compliance were limited. Therefore, we initially constructed a research model to identify the relationship between patient activation and patient compliance and its four mediators, namely physician–patient communication, health information seeking, perceived information asymmetry and e-health literacy.
The advent of the internet allows people to keep in touch with people who are unlikely to meet because of geographical distance or perceived “out-group” status. On the basis of social information processing theory, the nature of online relationships can be examined through social settings. 77 In OHCs, people are motivated to develop interpersonal relationships wherein their emotional and social connection is not considered less significant than with offline activities. Therefore, we used social information theory in our studies to determine the inner mechanism between patient activation and patient compliance.
Specifically, patient activation has direct and positive effects on physician–patient communication (0.845) and health information seeking (0.781). The path coefficients from patient activation on physician–patient communication and health information seeking are significantly larger than any other path coefficients. These results show that the effects of patient activation on the first two mediators are relatively significant. Therefore, physicians and OHCs' designers can discuss the pressing issue on how to provide an efficient and convenient way for patients to communicate with physicians and to seek health information and then indirectly improve patient compliance.
Second, physician–patient communication positively affects perceived information asymmetry and e-health literacy with path coefficients of 0.551 and 0.627, respectively. Health information seeking also positively affects perceived information asymmetry and e-health literacy with path coefficients of 0.276 and 0.277, respectively. In addition, path coefficients of physician–patient communication to perceived information asymmetry and to e-health literacy are higher than the corresponding coefficients from health information-seeking behavior. Thus, the effect of physician–patient communication is stronger than health information seeking on perceived information asymmetry and e-health literacy.
However, the directions of these effects contradict H3 and H5. Thus, H3 and H5 were not supported. We assume that physicians will sufficiently deliver information that patients do not have during communication. Patients might realize that physicians are more knowledgeable than they are. Thus, patients will perceive further information asymmetry. Moreover, incorrect message will mislead patients' judgment, which will increase information asymmetry. However, patients with high e-health literacy can assess the information and will not believe in any misleading information.
Therefore, physicians can discuss how to improve patient e-health literacy through physician–patient communication and health information seeking. As for communication, physicians provide similar content and style between online communication and in-person. 78 Thus, the online communication has similar effect with offline communication. Physicians need to enrich their knowledge and make patients fully understand communication content. Then, medical practitioners should build a competent and reliable image for patients during communication. This action will motivate patients to use OHCs and comply with their physicians. As for health information seeking, both physicians and OHCs must make efforts to guarantee the quality of information in OHCs by requiring the latter to provide information with greater accuracy. Moreover, physicians should pay additional attention to the links of communicating with patients, as communication has a stronger impact on perceived information asymmetry and e-health literacy and highly affects patient compliance.
Third, patient compliance is positively and directly affected by e-health literacy. However, we did not identify any direct effect from perceived information asymmetry to patient compliance. Individuals without adequate internet skills might also unknowingly obtain inaccurate health information. This situation negatively influences the improvement of e-health literacy. Thus, we assumed that perceived information asymmetry has a mediating effect on the relationship between e-health literacy and patient compliance. Specifically, perceived information asymmetry directly affects e-health literacy and indirectly affects patient compliance.
To confirm this new assumption, we reexamined the research model. The path coefficient from perceived information asymmetry to e-health literacy is 0.255, whereas the p-value is less than 0.001. In addition, the path coefficient from e-health literacy to patient compliance is higher than the corresponding coefficient in the original model. Therefore, perceived information asymmetry has a direct and positive effect on e-health literacy and has an indirect impact on patient compliance. These findings indicate that cultivating patients' e-health literacy is important to improve patient compliance. Thus, improving e-health literacy is crucial. Other than using physician–patient communication and health information seeking to improve e-health literacy, physicians must also pay extra attention on the influence of information asymmetry on e-health literacy. Thus, we modified the research model in Figure 3.

Modified research model.
Limitations and prospects of this study require consideration. First, we only regarded physician–patient communication, health information seeking, perceived information asymmetry, and e-health literacy as mediators to determine the relationship between patient activation and patient compliance. Other factors could be added for further investigation, such as social determinants of health (SDoH) and financial drivers. Second, we studied the research model based on the context of China. However, some differences may exist between China and other countries because of China's large population and disproportionate medical development. Thus, this research model should be tested and developed in other countries. Third, we used cross sectional survey to collect data from respondents, which could not capture patients' real-time attitudes. Fourth, we only considered the characteristics of OHC users but not those of China's census data. Further analysis could address this issue. Finally, the number of respondents was relatively small. Thus, our findings may be accidental.
Conclusions
This study indicates that patient activation positively affects patient compliance in OHCs through the mediations of physician–patient communication, health information seeking, perceived information seeking, and e-health literacy. In our research model, patient activation affects patient compliance through the mediation of four mediators. Patient activation has strong and direct effects on physician–patient communication and health information seeking. Physician–patient communication has a stronger impact on perceived information asymmetry and e-health literacy than health information seeking and consequently affects patient compliance. Perceived information asymmetry has no significant impact on patient compliance. However, it directly impacts e-health literacy and indirectly affects patient compliance. Therefore, e-health literacy has a stronger impact than perceived information asymmetry on patient compliance. These findings suggest that (1) physicians can analyze further approaches on improving patient activation for high patient compliance; (2) physicians and OHCs must exert further effort to improve the quality of information in OHCs; and (3) physicians should pay additional attention in cultivating patients' e-health literacy through communication and health information-seeking behavior to further improve patient compliance.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (key program; grant number 71532002) and National Social Science Foundation of China (major project; grant number 18ZDA086).