
Abstract
Introduction:
Telehealth is a rapidly expanding health care delivery modality with increasing utility in the health care community. It is imperative that telehealth education is provided during the training of health care providers to ensure the proper usage and application of this health care delivery system. A comprehensive literature review of telehealth education integrated into the curricula of physician, physician assistant, and advanced practiced registered nurse training programs has not been reported to date.
Materials and Methods:
An electronic literature search was performed using Scopus®, PubMed, and 17 of the 35 databases on the EBSCOHost platform. We included studies where telehealth concepts and components were integrated in the curriculum for primary care students. We extracted information pertinent to understanding the scope and sustainability of the curriculum and tabulated the results.
Results:
After a full-text screening of 164 articles and critically analyzing 34, eight articles were included in this review. Comparison of these articles showed no consistency in how telehealth was integrated into the various health care curricula. Content delivered usually included basic telehealth information, however, the depth and breadth of content varied significantly based on the interventions.
Discussion:
For the articles included in this review, there were no formal study designs regarding basic telehealth educational integration or competencies. While authors recommended conducting evaluation and determining the effectiveness of the interventions, they did not provide a clear picture as to how these efforts should be conducted.
Conclusions:
In addition to developing a standardized telehealth curriculum, national competencies need to be created, which will guide the development of standardized curriculum across health care training programs.
Introduction
There is a pending shortage of primary care physicians, especially in rural and underserved areas, which may not solely be improved with the integration of other health care providers (e.g., advanced practice registered nurses [APRNs] and physician assistants [PAs]). 1 The National Nursing Workforce Survey identified that the current demand for APRNs overshadows the supply, impacting the health care delivery care gap as well. 2 These provider shortages further exacerbate the health care barriers and inequalities that populations located in remote geographical locations encounter, therefore nontraditional methods of health care delivery must be utilized. 3 Telehealth, as a modality of health care, is recognized by the Health Resource & Services Administration (HRSA) as an integral part of the United States medical system, one that can improve access to care, enhance quality, and reduce costs. 4
Telemedicine as a health care delivery mechanism to increase access to health care is increasing in popularity. 5,6 Since there is no one definition for telemedicine, the World Health Organization (WHO) has developed a general description, which states, “The delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities.”7(p9)
Telemedicine and telehealth have been used interchangeably in the literature, but for the purpose of this article, telehealth refers specifically to health care provided at a distance, whereas telemedicine is the broader term that encompasses everything related to telehealth, such as education (patient, student and provider), video conferencing, public health interventions, televisits (asynchronous and synchronous), and mobile health or e-health.
Lack of technical telehealth education has been identified as a barrier to adoption of telehealth by health care providers. 8 Few providers receive telehealth-specific education during their academic careers even though this education is encouraged by their respective organizations. 9 For example, the American Medical Association (AMA) recommends telehealth training of medical students and residents, and recognizes that use of telehealth is critical in reducing health care barriers. 10 The National Organization of Nurse Practitioner Faculties (NONPF) express similar recommendations and encourage telehealth education integration in nurse practitioner curriculum to provide competencies which yield tools necessary to successfully develop and implement a telehealth practice. 11 The Physician Assistant Education Association advocates for integration of technology into 2019–2020 curriculum but does not specifically address telemedicine education. 12 However, telehealth education integrated into trainee education or health care provider education continues to be deficient. 13
A recent survey by the Association of American Medical Colleges (AAMC) stated that 58% of medical schools currently provide telehealth training to their students and the curriculum is not consistent, varying from a quick introductory module to a full semester of content. 14 Literature is sparse regarding the adoption of telehealth education into Advance Practice Provider (APP) curricula. Taken with the low adoption rate in medical school curricula, there is a demonstrated need for integration of telehealth competencies into health professions' education and the publication of outcomes resulting from larger percentages of learners. With the increased acceptance and usage of telehealth, the majority of providers should be trained to offer telehealth services to their patients. 5
Telehealth concepts are multifaceted and can be overwhelming for students without foundational knowledge and guided experiences. Foundational concepts include terminology and definitions, technologies, applications, health informatics integration, etiquette and professionalism, legislation and policy, credentialing and privileging, regulations related to professional scope of practice, and the development of practical skills. Robust exposure to these concepts through multiple integration points in the curriculum is essential for a competent health care workforce.
Education and experiential learning regarding telehealth should be founded in evidence-based competencies that direct learning are consistent across disciplines and institutions and ensure that development and implementation of telehealth practice are integrated into the curriculum following evolving laws and regulatory guidelines. 11 This ensures that patient safety and privacy are maintained while increasing the access, effectiveness, and efficiency of care to achieve improved health outcomes. This systematic review provides an overview of current telehealth education integration of telehealth components and proper usage into health care provider education in the extant literature.
Aim
The aim of this systematic review was to identify the presence and modalities of documented telehealth educational integration into the curricula of physician and APP training programs.
Materials and Methods
A systematic search of electronic databases was conducted to understand and document what exists in the published, peer-reviewed literature (gray literature was considered but not included). The electronic databases included: Scopus® (minus Medline); PubMed; and 17 of 35 databases within the EBSCOHost platform, including: CINAHL Complete; Academic Search Premier; Computer Source; Education Full Text (H.W. Wilson); ERIC; Health Source: Nursing/Academic Edition; Library Literature & Information Science Index (H.W. Wilson); Library; Information Science & Technology Abstracts; MAS Ultra—School Edition; Military & Government Collection; Newspaper Source Plus; Professional Development Collection; PsycARTICLES; Psychology and Behavioral Sciences Collection; PsycINFO; and Teacher Reference Center. The searches were conducted using adaptive keyword searching for each database to consistently use the same search terms. See Table 1 for the search strategy and procedures employed in each of the databases or platform searches. A collection of hand-searched articles was included in the review and these comprised additional articles that were already in the authors' personal libraries, those that were found incidentally (i.e., Google Scholar) and those obtained from the reference lists of relevant articles. For reporting purposes, Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines were used to conduct this review (Fig. 1).
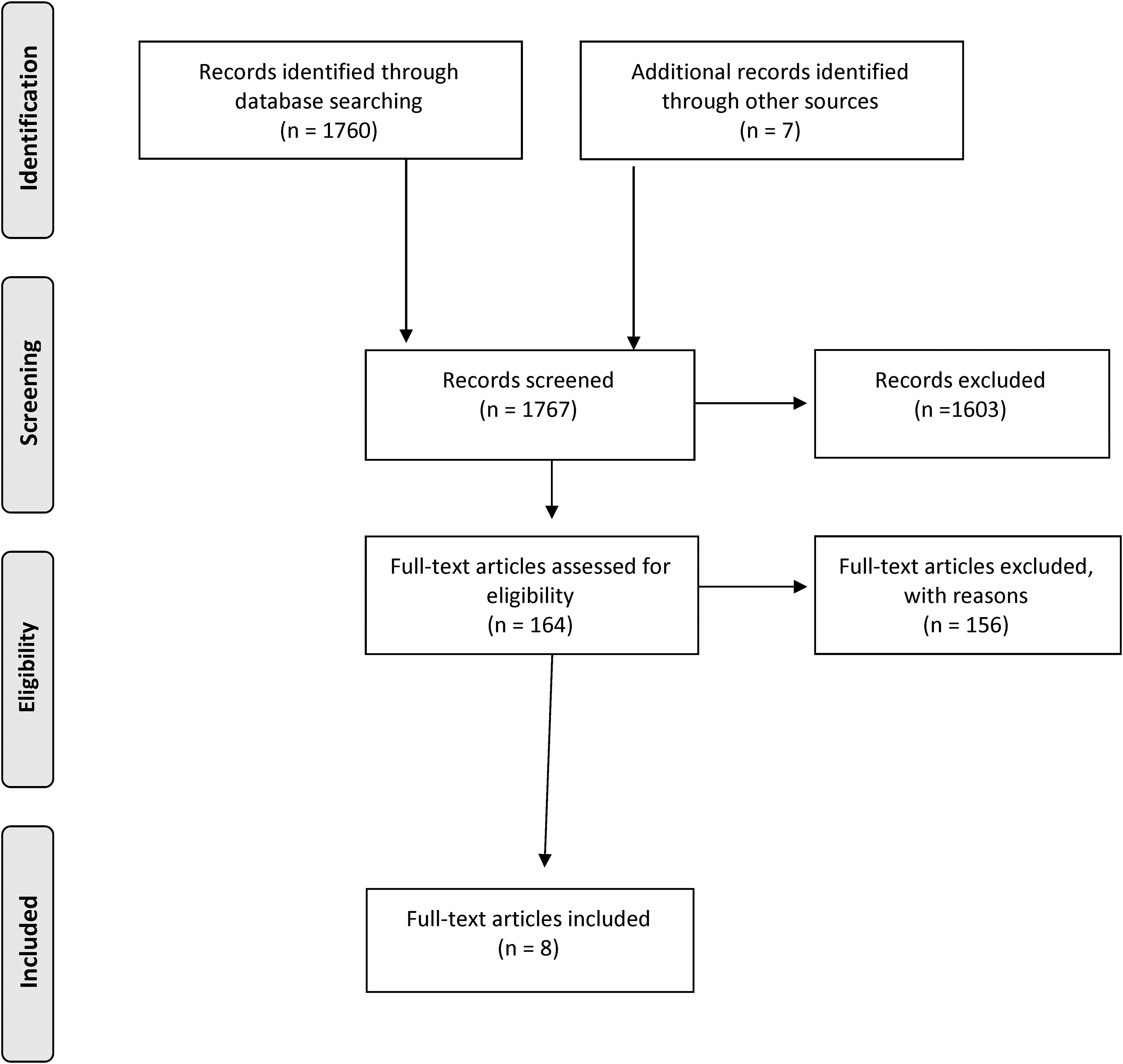
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) diagram.
Search Strategies and Procedures Employed in Each Database or Platform
Original search conducted on March 30, 2018.
To be included in this review, full-text articles from the last 10 years (January 1, 2008 through March 30, 2018) and in English (due to the lack of translation services) were chosen. Criteria for inclusion required a description of how telehealth was integrated into the curriculum, whether it was taught to medical and APP students, and if the curriculum included training based on the utilization of telehealth technologies. Articles that focused on counseling (unless it included descriptions of a physical assessment) or that were taught only to pharmacy, dental, occupational therapy, physical therapy, or cardiovascular perfusion students; or anything related to teleconferencing specifically (i.e., consulting, education, etc.), were excluded from this review.
An online survey tool, Microsoft® Form, was utilized by the Information Professional to assist in the abstract review, incorporating the inclusion/exclusion criteria by using branching logic and designated the articles as yes, no, or maybe based on the preset criteria. Once each reviewer completed the survey form for each article assigned, the results were viewed in Microsoft Forms and downloaded to Microsoft Excel for further tabulations.
Results
A total of 1,767 titles and abstracts of articles were reviewed by four reviewers. Based on the inclusion/exclusion criteria, only 164 full-text articles qualified for the next level of review established through this title and abstract review process. Based on the full article review using the predetermined inclusion/exclusion criterion and removal of duplicates, it was discovered that the inclusion/exclusion criteria needed refinement since a number of the articles found used telehealth as a means or method of education (e.g., teleconferencing) rather than the integration of telehealth components and usage into health care provider curricula. Use of this refined inclusion/exclusion criteria reduced the number of articles from 164 to 34 for critical analysis. Each questionable article was discussed by the author group to clarify any disagreements or questions before the article was moved forward to the critical analysis stage.
The literature search, full-text reading, and the critical analysis revealed eight articles that met the eligibility criteria for this systematic review. A summary of the synthesis of these findings is presented in Table 2.
Summation of Articles Included for Review
ABSN, Accelerated bachelor of science in nursing student; APRN, advanced practice registered nurse; COM, college (or school) of medicine; CON, college (or school) of nursing; DNP, Doctor of Nursing Practice; F2F, face to face; HRSA, Health Resources & Services Administration; HW, homework; IPE, Interprofessional education; IT, information technology; NE, nurse executive; NP, nurse practitioner; SIM, Simulation; SP, standardized patient.
ARTICLE AIM
All eight articles shared similar aims with most striving to introduce telehealth general knowledge. 15 –22 One article focused on telehealth's applicability in rural or underserved populations, 17 and three other articles on the collaboration among interdisciplinary or interprofessional (IP) disciplines. 18,21,22 Another article focused on investigating different communication technologies that can be utilized for teleconferencing. 15
STUDENT GROUPS
There was a wide range of health care professional students that were involved in the various education programs. Five programs focused on nursing students, accelerated bachelor of science in nursing (ABSN), and APRNs. 15,17,21,22 One of these programs described using a process of nursing students working in pairs, for example a Doctor of Nursing Practice (DNP) in the Nurse Executive track with an DNP APRN student, each living in a different U.S. region. 15 Two other nursing programs paired ABSN students with distant DNP students within a simulated setting using telepresence robots. 21,22 Two medical programs described the development of telehealth elective courses for medical students. 16,19 The final program described an Interprofessional Education (IPE) team consisting of APRN, graduate medical, pharmacy, and industrial engineering graduate students. 18
CURRICULUM PROGRAM AND INTEGRATION
Telehealth components were integrated into curricula using numerous methods and varied from mandatory to nonmandatory, modality of educational intervention, and whether or not experiential learning was provided. Of the eight programs, two programs integrated telehealth components into the curriculum as a mandatory requirement of the students' learning, 17 two were nonmandatory, 16,19 and three programs did not indicate whether or not the experience was mandatory. 18,19,22 One program created mandatory versus elective components based on student type; mandatory for the ABSN students but optional for the APRN students. 21
When examining the modality of telehealth education, there were differences regarding how telehealth education was offered to the students. Four programs utilized face-to-face instruction, 16,17,21,22 one program provided education through an online platform or through teleconferencing, 11 and three programs combined face-to-face instruction complemented with an online platform. 17,21,22
Of the eight programs reviewed for student exposure to any type of clinical experience, four offered a clinical rotation, 16 –18,20 of which two included simulated activities. 17,20 Two programs utilized simulated clinical experiences only. 21,22 Two programs did not specify offering any clinical application or simulation experiences. 15,19
DURATION OF TRAINING
There was variation in the duration of telehealth education in the programs that ranged from 1-h to 8 weeks, with no similarities. One program provided a 1-h class, followed directly by a 4-h clinical rotation. 17 Two program interventions occurred over 1 month, 15,16 another program provided 4-h classes for 7 days, 19 and one consisted of a weekend immersion of undetermined time followed by an 8-h clinical experience. 20 The longest telehealth integration was an 8-week rotation that afforded various in-class and IPE clinical opportunities. 18 Two programs did not indicate the time period used for the telehealth education. 21,22
INSTRUCTOR TYPES
All telehealth experiences were taught by faculty of their respective programs, 15 –22 with two of the eight programs taught by an IP team. 17,18 One IP team consisted of faculty from various academic programs 18 and the another included providers from the Health Department in addition to rural clinical site employees, graduate nursing faculty, and information technology professionals (one from the college and one at the clinic). 17 The level of instructor knowledge related to telehealth was not disclosed for any program reviewed.
NUMBER OF PARTICIPANTS
The number of student participants varied widely among programs. Two programs did not specify the number of participants. 15,17 One program reported the number of IP students who completed a survey (19 students), but did not indicate the total number of participants of the completed educational intervention. 18 Of the two medical school telehealth elective courses, one program reported 7 fourth-year medical students participating during the first year, 16 while the other had a total of 112 medical students over 4 nonconsecutive years. 19 Telehealth programs that focused on nursing students included 1 program reporting 60 DNP students, 20 2 describing an unknown number of interdisciplinary students, 1 program reporting 76 ABSN, and 8 pediatric APRN students, 21 and another with 48 ABSNs and 5 pediatric APRN students. 22
MODALITIES
Telehealth education was provided to students using different modalities, including topics such as telehealth definitions, roles, licensing, reimbursement, safety, patient empowerment, and developing a telehealth service. Three of the eight programs provided basic telehealth knowledge using online modules. 15,17,20 Of these three programs, two utilized online education with telehealth-related site visits or clinical experiences, 15,17 and another included IPE-simulated telehealth experiences. 20 Five programs utilized face-to-face instruction, 16 –20 of which one provided a 4-h telehealth clinical rotation 17 and the other an external immersion experience with student projects. 20 Two programs blended ABSN students who participated through in-person consultations with APRN students who participated remotely through a telepresence robot during the simulated telehealth experience. 21,22
OUTCOMES
Overall, all programs reported high student satisfaction, although one did not report on formal outcomes. 17 Students frequently shared they would consider using telehealth in their future practice or accept a position that involved telehealth. 16,19 One program reported students' increased acceptance of technology in patient care and a desire to incorporate telehealth into future practice. 17 Another program resulted in students identifying the need for IP teams and how utilization of telehealth can increase access to care. 18 Students expressed increased problem-solving scores when telepresence robots were used in a simulated environment, earning an average score of four out of five possible points. 21 Another program, using a telepresence robot, reported high levels of acceptance and the use of teleconferencing increased activity participation for distance students. 22 One program reported that graduates of the telehealth experience used the information to attain grants, develop and implement a nurse-run telehealth clinic, and incorporate teleconferencing between specialists and others for high-acuity pediatric patients. 20
EVALUATION AND ASSESSMENTS
The majority of programs included some type of student curriculum appraisal for the telehealth integration program development. 15,16,18 –22 One program used a self-reflective, written assignment to gauge the impact of telehealth on the student's eventual practice area. 16 Another incorporated a reflective assignment focusing on teams and team skills, while also seeking feedback through surveys and using pre- and post-tests to assess knowledge change. 17 A summative written assignment was employed in one program to evaluate teleconferencing technologies. 15 Finally, self-administered Likert scale evaluation surveys were used in three of the eight programs, 19,21,22 and one included both a Likert scale and open-ended questions. 20
LIMITATIONS
The self-identified barriers and limitations of the programs varied, although there are some reported commonalities. Minor technology frustration was listed by one program as a limitation. 15 Difficulties in the coordination of clinical-site rotations were identified as a barrier, 17 as well as the lack of diversity in the types of health care providers and programs. 21 Student recruitment in IPE was listed as challenging and included project planning, infrastructure development, and coordination of teams. 17 Another weakness identified was absence of an annual evaluation for each year of program implementation. 16,19,20
Lack of enrollment related to telehealth course offerings being elective in nature was viewed as a limitation to telehealth education in two programs. 15,19 Cost issues, such as start-up expenses, training, and lack of reimbursement by insurance companies were identified as potential barriers that might decrease student interest. 19 One program mentioned limitations but failed to elaborate as to what they were. 22
FUNDING AND SUSTAINABILITY
Two of the education projects were funded by HRSA, one by a Predoctoral Training Grant 16 and the other by an IPE project grant. 19 Regarding sustainability, three of eight programs did not report any plans to continue telehealth integration, 15,16,22 and one reported a pilot IPE integration program that could be replicated but did not indicate whether it would continue. 22
Three programs reported continuing the implementation of telehealth within their curricula 17,19,20 ; one of an undetermined length of time, 19 another for 18 months at the time of publication, 17 and one since 2011. 20 None of the authors discussed how or why these programs have been successful. Only two of the articles described embedding telehealth content into the curriculum, 17,20 while two others were elective courses. 16,19 Sustainability was discussed in two programs, but they did not share the monetary costs or how they were addressed in the budget process. 19,20 Overall, the programs reported pilot information gauging feasibility of telehealth education into the curriculum.
RECOMMENDATIONS
All programs recognized the benefit of integrating telehealth into the curriculum, either through experiential learning opportunities, 15,21,22 elective courses, 16,19 team-based learning approach, 17 or embedded into required courses. 17,20 IPE telehealth education is also recommended by two of the eight studies and specifies the importance of having educational teams across multiple disciplines to enhance student IPE and improve patient outcomes. 17,20 Finally, one study encouraged graduate nursing faculty to identify courses where these clinical components are most applicable to incorporate telehealth fully into the graduate nursing curriculum. 17
Discussion
The findings from this systematic review describe program development, implementation, and evaluations based on limited curriculum interventions and illustrate that no formal research has been performed on telehealth education integration. Based on this systemic review, there exists no set criterion in use for integrating telehealth education into the health care curricula. More research with formal quantitative, qualitative, and mixed-method protocols deployed from the inception of the curriculum are needed to establish evidence-based, best practice guidelines. Additional longitudinal evaluations of educational effectiveness should also be implemented.
Consistency of student learning, outcome documentation, the development of competencies, and how they are applied based on provider type is lacking in the current literature. Consistency is key to ensure that the multifaceted telehealth modality of health care delivery is provided to students across health care curricula in a manner that results in a workforce with shared and equitable knowledge.
Standardized telehealth education-based surveys that include basic telehealth knowledge and skill competencies can be used to provide consistency and the delivery of telehealth education and evaluation. These surveys can be comparative between institutions to normalize telehealth education integration strategies. Utilization of ongoing systemic reviews or discipline-specific surveys across professional health training programs could yield the current state of integration, which may be a more accurate measure of telehealth curriculum. The authors of this systemic review identified minimal limitations in the research and presentation of this review while stressing the need for additional rigor in telehealth education studies to include both quantitative and qualitative data.
Conclusion
To date, there are no formal study designs in the literature regarding basic telehealth educational integration or competencies in a world where telehealth continues to grow. It is difficult to estimate the total breadth of telehealth education integration in existence, as this review is based on published literature only. The findings detailed in this review recommend additional study and do not provide a clear plan as to how existing efforts will be continued. A telehealth common elements and research database would assist in comparison of programs and outcomes. In addition, the creation of national and international competencies will guide the development and evaluation of the standardized curriculum.
Footnotes
Disclaimer
The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Health Resources and Services Administration (HRSA) Advanced Nursing Education Workforce (Grant No. T94HP30872, 2017-19). The development of this article was supported by the HRSA of the U.S. Department of Health and Human Services (HHS) as part of the National Telehealth Center of Excellence Award (U66 RH31458-01-00).