
Abstract
Background:
Stroke is the leading cause of serious long-term disability in the United States. Barriers to rehabilitation include cost, transportation, lack of trained personnel, and equipment. Telerehabilitation (TR) has emerged as a promising modality to reduce costs, improve accessibility, and retain patient independence. TR allows providers to remotely administer therapy, potentially increasing access to underserved regions.
Objectives:
To describe types of stroke rehabilitation therapy delivered through TR and to evaluate whether TR is as effective as traditional in-person outpatient therapy in improving satisfaction and poststroke residual deficits such as motor function, speech, and disability.
Methods:
A literature search of the term “telerehabilitation and stroke” was conducted across three databases. Full-text articles with results pertaining to TR interventions were reviewed. Articles were scored for methodological quality using the PEDro scale.
Results:
Thirty-four articles with 1,025 patients were included. Types of TR included speech therapy, virtual reality (VR), robotic, community-based, goal setting, and motor training exercises. Frequently measured outcomes included motor function, speech, disability, and satisfaction. All 34 studies reported improvement from baseline after TR therapy. PEDro scores ranged from 2 to 8 with a mean of 4.59 ± 1.94 (on a scale of 0–10). Studies with control interventions, randomized allocation, and blinded assessment had significantly higher PEDro scores. All 15 studies that compared TR with traditional therapy showed equivalent or better functional outcomes. Home-based robotic therapy and VR were less costly than in-person therapy. Patient satisfaction with TR and in-person clinical therapy was similar.
Conclusions:
TR is less costly and equally as effective as clinic-based rehabilitation at improving functional outcomes in stroke patients. TR produces similar patient satisfaction. TR can be combined with other therapies, including VR, speech, and robotic assistance, or used as an adjuvant to direct in-person care.
Introduction
Stroke is the leading cause of serious long-term disability in the United States. 1 –3 Each year, ∼795,000 Americans suffer a stroke and 140,000 die from stroke. 1,3 Stroke is the fifth leading cause of death in the United States and the second worldwide. The annual cost of stroke management in 2017 was $34 billion. 1
As only 25% of patients return to their prestroke level of physical function and social involvement, stroke also increases stress and demand on caretakers and family members. 2 Although motor and sensory deficits are among the most common disabilities, other deficits include aphasia, cognitive deficits, and emotional disturbances. The psychological and physical trauma of a stroke may lead to clinical depression, which is a predictor of poor functional outcome. 4 Significant barriers to poststroke rehabilitation include dependence on caregivers, financial problems, lack of regional medical resources, and challenges with transportation—all exacerbated in rural settings. 5 –7
Telerehabilitation (TR) has emerged as a promising modality to overcome several of these limitations. TR is a telemedicine approach that allows patients and caregivers to interact with providers as they remotely supervise, monitor, and administer various forms of physical, occupational, speech, and other therapies. Types of TR include guided physical therapy, speech therapy, virtual reality (VR), robotic-assisted training, and goal setting. Therapy sessions can be individual or community based. TR can improve accessibility and health care worker-to-patient ratios in underserved regions. 6,8
Improvements in technology have allowed TR to grow in popularity and expand beyond simply monitoring therapeutic exercises. VR provides patients with a motion sensing device and a headset or screen displaying a virtual environment. Patients are asked to perform therapeutic movements that correspond to tasks within the virtual environment. This provides a more immersive experience for the patient while allowing remote monitoring of patient progress. 9 –16
VR has also been combined and integrated with robotic-assisted training. 8,17 Hand and foot strengthening robots can provide strength and movement assistance for patients with accessibility needs who might otherwise require in-clinic rehabilitation. 18 Furthermore, robotic devices can be used both for training and for assessment, including automatic transmission of daily usage statistics, adding a more objective tool for providers to gauge and adjust treatment remotely.
While individual home-based therapy is the most popular form of TR, this therapy has extended beyond the home into community-based TR. This approach is administered remotely through video to patients outside the home in small groups such as retirement homes or at publicly accessible kiosks. 19,20
This literature review aims to assess studies of various forms of TR in stroke survivors and their findings in regard to functional outcomes, patient satisfaction, and health care access.
Methods
A literature search using the phrase “telerehabilitation and stroke” was conducted across three databases (PubMed; Cumulative Index to Nursing and Allied Health Literature (CINAHL); and Physiotherapy Evidence Database (PED)). Inclusion criteria were full-text articles written in English as of October 31, 2019 describing completed clinical interventions on human subjects. Exclusion criteria were duplicate publications describing the same study, reviews, case studies reporting on only a single patient, studies not performed exclusively with stroke patients, studies not describing a TR intervention, and studies that did not report motor, sensory, cognitive, satisfaction, or functional outcomes. Titles and abstracts were reviewed independently by two authors (J.Z.M. and K.D.K.) for eligibility. All authors reviewed included full texts. All disagreements were handled through consensus.
Quality Assessment
Studies were evaluated for quality by the Physiotherapy Evidence Database (PEDro) scale metric. 21 Quality is scored on a scale of 0–10 based on 0 or 1 points assigned to each of the following factors: randomized participant allocation, concealed participant allocation, comparable baselines, blinding of participants, blinding of therapists, blinding of assessors, key outcome measurements completed in >85% of participants, intention to treat analysis, between-group statistical comparisons, and results reported as point measures with measures of variability. Although the PEDro scale is designed to assess controlled trials, the scoring criteria were also applied to the uncontrolled studies included in this review. Individual study PEDro scoring details can be found in Supplementary Appendix Table SA1. PEDro evaluations of all studies were performed independently by two authors (F.O.O. and P.W.), with subsets scored independently by two other authors (K.D.K. and N.Y.H.). Differences in scoring were resolved by consensus.
Data Synthesis and Analysis
All data analysis was performed using Excel and SPSS® Version 26. Sums, means, and standard deviations are reported for total number of patients and for PEDro scores across studies. Independent Student's t-tests were used to compare mean differences for PEDro scores across subgroups of studies. A Bonferroni correction was applied to the six subgroup comparisons, setting criteria for significance at p = 0.05 ÷ 6 = 0.0083.
Results
The initial database search yielded 178 articles in PubMed, 79 in CINAHL, and 16 in PED. After excluding duplicate studies, 180 unique articles remained. After applying inclusion and exclusion criteria, 34 articles remained and were included in qualitative review (Fig. 1). These included 32 in PubMed, 11 in CINAHL, and 11 in PED. The only studies that were not indexed in PubMed were Deng (CINAHL) and Meltzer et al. (CINAHL). 22,23 Fifteen studies controlled for TR versus in-person therapy, 4 studies compared different TR approaches to one another, 1 study controlled for TR versus no therapy, and 14 studies were uncontrolled (Table 1). One group of patients was reported in two articles analyzing different outcomes. 5,24 Both articles were reviewed, but the patients were only counted once toward the total number of 1,025 patients included in this study. Sample sizes ranged from 5 to 188 patients with a mean of 31.1 ± 37.7.
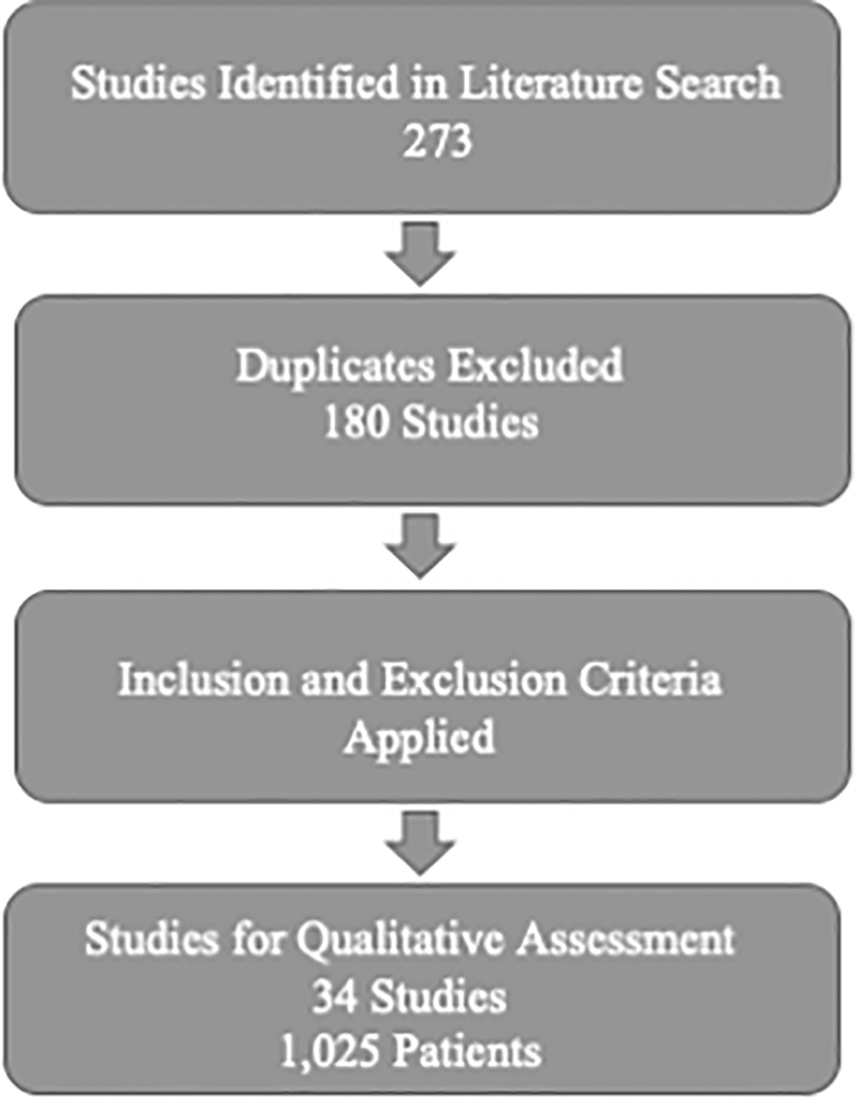
Flowchart of study selection.
Description of Included Studies
Same cohort of 52 patients from 2012 study. Not counted twice in Totals.
PT, physical therapy; TR, telerehabilitation; tx, treatment; VR, virtual reality.
The most commonly studied type of TR was video-supervised home motor training exercises (11 studies, 350 patients). 5,22,24 –33 Eight studies including 166 patients involved tele-VR therapy 9 –16 ; 7 studies including 124 patients involved tele-speech therapy 23,34 –39 ; 4 studies including 148 patients involved telerobotic-assisted exercise 7,18,40,41 ; 2 studies including 209 patients assessed community-based teletherapy 19,20 ; and 1 study of phone-based goal setting included 28 patients. 42 (Fig. 2).

Types of TR with numbers of patients and studies. TR, telerehabilitation.
Physical, functional, speech, logistical, and subjective self-reported outcome measures were used across studies. The Wolf Motor Function test and Fugl-Meyer assessment (six studies each) were the most commonly used measures of motor function, 7,10,15,16,19,22,27,28,32,33,41 Functional Independence Measure (four studies) was the most commonly used measure for degree of disability. 5,11,18,30 Western Aphasia Battery (three studies) was the most used measurement of speech ability. 23,36,39 Satisfaction was another commonly tested measure, although the majority of articles that reported satisfaction used nonstandardized questionnaires or patient interviews. 15,29,30,36,43
All 34 studies showed quantitative patient improvement from baseline after TR therapy. Among the 16 studies with non-TR control interventions, 9 observed equivalent outcomes between TR and non-TR, and 7 observed better outcomes after TR, although many of these had mixed results among multiple outcomes, with difficulty distinguishing primary from secondary outcomes.
Study quality was assessed using the PEDro scale. 21 PEDro scores ranged from 2 to 8 with a mean of 4.59 ± 1.94 (Table 1). We compared PEDro scores between subgroups of studies according to whether or not they achieved key criteria of study quality (Table 2). Studies that compared TR with a control intervention (n = 20, 5.80 ± 1.70) had significantly higher PEDro scores than uncontrolled studies (n = 14, 2.86 ± 0.36, p < 0.0001). Studies that enrolled 10 or more subjects (n = 26, 4.92 ± 2.12) tended to have higher PEDro scores than those that enrolled <10 subjects (n = 8, 3.50 ± 0.76, p = 0.0736). Studies that randomly allocated subjects to groups (n = 15, 6.20 ± 1.74) had significantly higher PEDro scores than those that did not (n = 19, 3.32 ± 0.95, p < 0.0001). Studies that utilized concealed allocation of subjects to groups (n = 7, 7.71 ± 0.49) had significantly higher PEDro scores than those that did not (n = 27, 3.78 ± 1.25, p < 0.0001). Studies that utilized blinded assessment (n = 11, 6.82 ± 1.40) had significantly higher PEDro scores than those that did not (n = 23, 3.52 ± 1.12, p = 0.0001). Finally, studies that recorded key outcome data in at least 85% of different (n = 28, 4.75 ± 2.08) did not have significantly different PEDro scores than those that did not (n = 6, 3.83 ± 1.17, p = 0.3085).
PEDro Score by Subgroup
Significant <0.0083.
From the patient-oriented perspective, the interactive video capabilities of TR have shown increased patient satisfaction over home rehabilitation programs without video functionality. 30 Two studies reported superior patient satisfaction or anxiety scores in patients receiving TR compared with those receiving traditional clinical therapy, 14,24 whereas two studies reported equivalent scores. 13,29 One study reported superior satisfaction and motivation scores in patients receiving in-clinic therapy over those receiving TR, despite equivalent improvements in motor function. 33 Two studies addressed cost: Lloréns et al. found VR-based TR to cost $654.72 less per patient than clinic-based rehabilitation, a savings of 30.5% over the course of the program. 13 Housley et al. reported a cost savings of 64.97% for home-based robotic therapy over clinic-based therapy. 18
Discussion
Multiple studies demonstrated that TR is an effective treatment for stroke, leading to increased motor function, speech function, cognitive function, and quality of life. Although there is no consistent evidence to show that TR is superior to in-person therapy, TR does offer several inherent advantages: The interactive video capabilities of TR have shown increased patient satisfaction over home rehabilitation programs without video functionality. 30 TR has also expanded the scope of rehabilitation by allowing providers to see and interact with patients without the patient having to leave home, which may be difficult due to residual motor deficits, costs, and accessibility.
Furthermore, combining TR with other home-based interventions is likely to improve patient-oriented outcomes when patients otherwise have no access to rehabilitation services. Kamwesiga et al. showed that even in an area where rehabilitation therapy was unavailable, simply guiding patients and family members to set daily goals led to increased satisfaction and improvements in performance of activities of daily living. 42
Regardless of modality (supervised physical exercise, VR, robotic-assisted training, or cognitive/speech therapy), patients receiving TR have generally reported high usability and satisfaction ratings with the technology, whether used in the home or at community kiosks. Although some patients prefer the gratification of direct human interaction, other patients may favor the increased convenience and accessibility of TR over repeated clinic visits.
No significant differences in functional outcomes were shown between patients who used community-based TR and patients who exercised at home without TR. 20,42 Although improving access for those who lack home internet access or internet literacy, community-based TR has apparently lower compliance than home-based TR. 19,20 Benvenuti et al. reported only 30% compliance with TR kiosk visits. 19 However, patients who visited the kiosks regularly were more compliant with home exercise therapy and showed improvements in stroke education.
TR can also be used to provide more effective education. Daily stroke education through the TR system was associated with a 39% increase in stroke prevention knowledge. 32 Patient education scores were similar between TR and clinic groups. 31
Although patient–provider interaction occurs remotely with TR, providers do have the ability to communicate and assess patient feelings. Depression scores obtained through TR correlated with scores obtained in person, suggesting that TR provides a reasonably accurate way for providers to assess and treat emotional effects of stroke. 32
Limitations
Although a transparent literature search strategy and inclusion criteria were utilized, the specific focus on the term “telerehabilitation” may have resulted in excluding some studies that fall within the TR scope. For example, studies by Boter and HESTIA Study Group and Bishop et al. that used telephone calls to provide extra home follow-up after hospital discharge may show promise, but were not included in our results. 44,45
Furthermore, the use of inconsistent outcome measurement scales makes meta-analysis of TR efficacy difficult. For example, the most commonly used outcome measures, Wolf Motor Function test and Fugl-Meyer assessment, each appeared in only 6 of the 34 articles. 7,10,15,16,19,22,27,28,32,33,41 Two systematic reviews on TR for stroke that were published during the revision of this article both noted the same limitations of poor overall study quality and inconsistent approaches making it impossible to conduct reliable meta-analysis. 46,47 Although uncontrolled studies rarely provide high strength of evidence, we decided to include them in this review, given the relative dearth of randomized controlled stroke TR research available. This review of TR for stroke is the first to our knowledge to apply the PEDro criteria to assess study quality.
Future Directions
Although TR demonstrates potential to improve rehabilitation outcomes and patient satisfaction, the amount of research is limited by sample size, power, and study design. Out of the 34 articles selected from the literature search, only 15 studies controlled for TR versus other modalities, and only 2 studies included >100 patients. Including more studies with larger subject pools could offer a more thorough assessment of TR study conclusions. Another limitation for TR therapy evaluation stems from the inability to blind subjects and health care providers during treatment. All patients and therapists were aware that TR was being administered, making blinding to therapy difficult. We observed significantly higher PEDro scores of study quality in studies that compared TR with a control intervention, randomized and concealed subject assignment, and used blinded assessment.
Future directions should include larger controlled studies on the effectiveness of TR, with an emphasis on blinded assessment, standardized outcome measurements, and cost analysis. Research should investigate not only the determinants of patient satisfaction with TR, but the determinants of provider satisfaction with TR as well. Furthermore, additional investigation could examine the effectiveness of TR at delivering other new therapy modalities such as neuropsychological and computerized cognitive behavioral therapy approaches. 48,49
Conclusion
TR is equally as effective as conventional clinic-based rehabilitation at improving functional outcomes after stroke. Patient satisfaction with TR may be higher, lower, or equivalent to clinical rehabilitation depending on methods and individual patient preference. However, advantages of TR over traditional clinical therapy include increased accessibility and possibly decreased cost, making TR a valuable alternative for patients with financial, geographical, or transportation constraints. Furthermore, TR may also be combined with clinic-based rehabilitation.
TR can be applied in many ways, including with home-based robotic therapy, speech therapy, and VR. TR can also be delivered effectively through community kiosks. Integration of TR with other services such as home visits improves patient compliance. Future research should use standardized measures and assess the costs and satisfaction of TR in addition to functional outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.
Supplementary Material
Supplementary Appendix Table SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.