
Abstract
Introduction:
To evaluate if the offering of Fitbit technology led to changes in cardiovascular health metrics in a cohort of older adults.
Methods:
A retrospective cohort study was developed in two community-embedded health monitoring sites, located in aggregate housing communities for older adults in Westchester County, NY. Participants included older adults (55 years or older) enrolled in the Telehealth Intervention Programs for Seniors (TIPS) initiative, a community-embedded remote patient monitoring initiative. Weekly blood pressure, heart rate, weight, and blood oxygenation were taken on all participants. For participants who accepted a Fitbit Zip device, a weekly step count was also collected.
Results:
Ninety-four TIPS participants were offered Fitbit technology. Thirty participants accepted the technology and used it for a minimum of 6 months. No significant differences in any of the regularly acquired biometrics were noted between Fitbit users and non-Fitbit users. Across all participants, regardless of Fitbit use, there was a significant decrease in systolic blood pressure (SBP) over time.
Conclusions:
Neither Fitbit Zip ownership or compliance to Fitbit Zip usage influenced any of the biometrics taken as part of the TIPS. However, participation in the TIPS initiative may have an overall positive effect on SBP in older adults.
Introduction
Wearable devices can be used to track and record various health parameters such as vital signs, physical activity, and falls. By providing physicians with remote access to patients' vital signs, wearables can facilitate early detection of health changes and can thereby prevent sudden disease onset or patient hospitalization. 1 This especially benefits individuals with physical disabilities or chronic conditions, as well as older individuals who have a higher risk for disease and falls. 2,3
In addition, consumer-facing health wearables can benefit patients directly by helping them monitor their own health. These devices display basic and easily understandable information about daily physical activity such as (1) number of steps taken, (2) distance walked, (3) calories burned, (4) hours of sleep, and (5) duration of exercise, 4 and there is some evidence to suggest that activity monitors may encourage some users to maintain a physically active lifestyle. 5,6 Promotion of physical activity is often associated with increased physical activity and improved health outcomes. 2
However, the actual impact of health wearables is still unclear. Many large trials 7,8 indicate that Fitbit (Fitbit, San Francisco, CA) usage has minimal health benefits. Alternatively, other studies suggest that wearables can positively impact diet, mental health, self-efficacy, medication adherence, disease management, body mass index, and physical activity by targeting user behavior and satisfaction. 9,10,11 Many older adults who are health wearable users are increasingly reporting them as helpful and easy to use, 12,13 and therefore, it is likely that they will continue to grow in popularity. However, their benefits are still unclear, and there is a pressing need to further investigate the impact of activity monitoring wearables on health outcomes.
In our previous work, 14 we investigated the Telehealth Intervention Programs for Seniors (TIPS), a community-embedded health and wellness initiative led by the Westchester Public/Private Partnership for Aging Services. TIPS targets low-income, high health-risk older adults and provides wrap-around aging services, including weekly monitoring and assessment of vital signs and subjective wellness. We found that TIPS reduced self-reported hospital visits by 28.9% between 2014 and 2016. 14 In the present study, we aimed to determine whether offering a Fitbit Zip, a health wearable, could passively improve health biometrics in a cohort of older adults.
Methods
Ethics Statement
Researchers from the Icahn School of Medicine at Mount Sinai obtained fully deidentified data collected by the Westchester Public Private Partnership as part of their TIPS initiative. The Icahn School of Medicine at Mount Sinai Program for the Protection of Human Subjects reviewed the nature of the deidentified data and made a formal determination that they did not qualify as human subjects' data (IRB-17-02553).
The TIPS Initiative
Participants were deemed eligible for the TIPS initiative if they were aged 55 years or older and were managing any chronic health conditions. Telehealth Technician Assistants (TTAs) employed by the TIPS initiative were trained to measure physiological biomarkers from older adults attending TIPS monitoring sessions (Fig. 1). TTAs would attend TIPS sites once or twice per week (depending on location and availability of the TTAs) and TIPS participants were encouraged to attend monitoring sessions at least once per week. The biomarkers measured at TIPS sites were systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), weight (Wt), and blood oxygen saturation (SpO2). In addition, TIPS participants also had access to a variety of social services, such as the National Council on Aging Benefits Checkup Assessments, Livable Communities Speakers Bureau Educational Presentations, Chronic Disease Self-Management Programs, and caregiver support programs.

During Telehealth Intervention Programs for Seniors monitoring sessions, participants had their physiological biometrics measured.
The iTIPS Fitbit Program
In 2016, the TIPS initiative received the requisite funding to offer all older adults who were attending either one of two TIPS sites in Westchester County with the Fitbit activity tracking technology. The Fitbit device that was selected for this program was the Fitbit Zip—a wireless actimeter that is hooked onto the users' clothing, typically at the waist. To capture the full day's activity, participants were instructed to attach the Fitbit Zip when they were dressing at the beginning of each day, and remove it when they were preparing to go to bed at the end of the day. During each weekly TIPS session, TTAs collected and recorded step count data from the Fitbits to estimate participants' daily level of activity. The number of steps taken on a week was calculated as the difference between the number of steps displayed by the tracker during a TIPS session and the number of steps displayed during the previous session. To maintain consistency across the cohort, TIPS participants were not responsible for tracking their own steps on the Fitbit app, regardless of whether they owned a smartphone. All TIPS participants were offered a Fitbit Zip when they attended their weekly TIPS session. All other TIPS services were provided as usual, regardless of the participant's choice to accept or decline the Fitbit.
Data Analysis Approach
Physiological biomarker data from TIPS participants were collected at each visit with the TTAs. Objective changes in biomarkers were determined by measuring the difference in first and final values collected during TIPS monitoring sessions. Participants were pooled into “Non-Fitbit Users” or “Fitbit Users” based on usage of the device. Within each group, participants were then categorized as noncompliant (<3 months), short term (3–6 months), and long term (>6 months) based on the duration of their participation in the TIPS initiative, not the duration of Fitbit usage (Fig. 2). Any TIPS participants who showed poor compliance to the TIPS as a whole, or were missing large amounts of data from their records were excluded from the analyses.
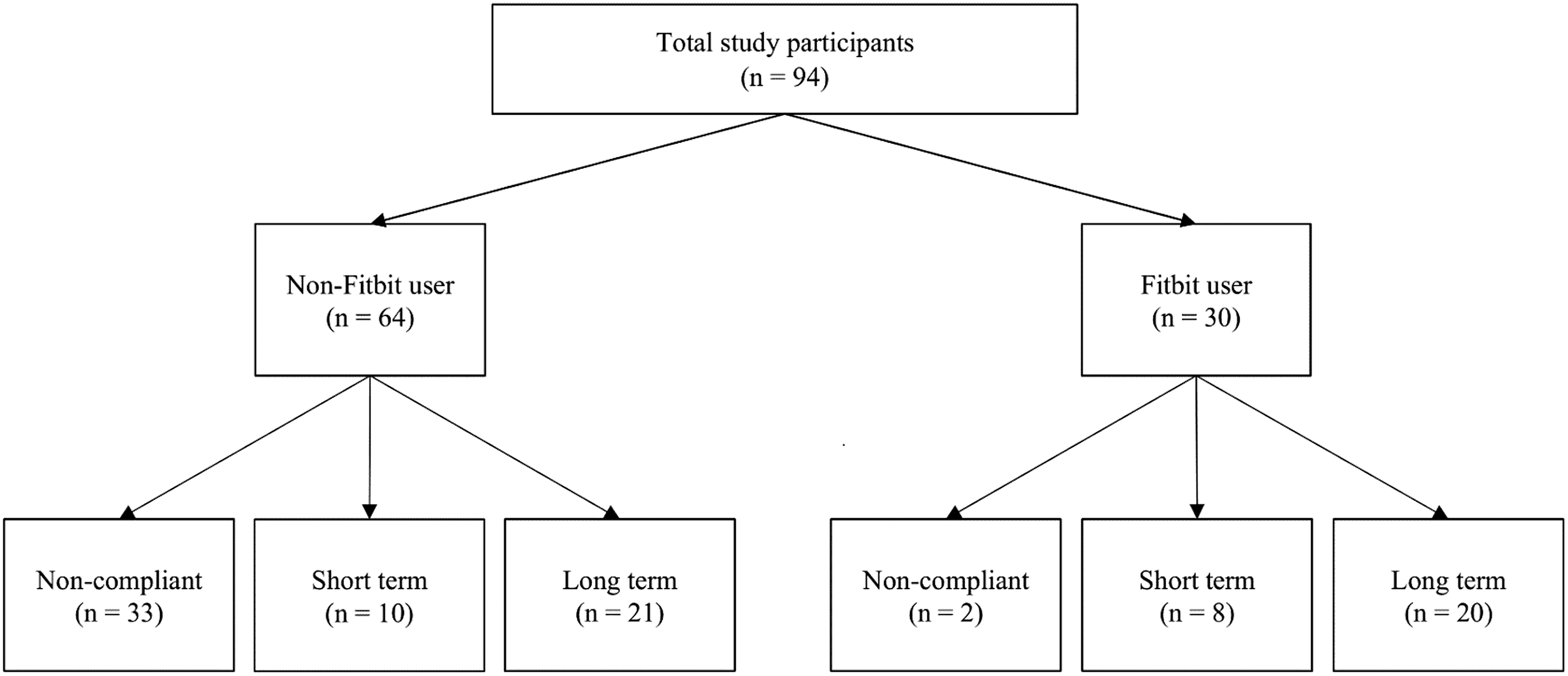
CONSORT diagram displaying participant group assignments.
Univariate within-group analysis of Fitbit users and non-Fitbit users was performed using a one-factor t-test. To determine the effect of Fitbit usage, Fitbit users and non-Fitbit users were compared using a two-factor independent t-test. In all cases, Bonferroni correction was used to control for multiple comparisons.
Results
For the purposes of this study, data from two TIPS locations were audited from a 12-month period, starting June 1, 2016, and ending April 31, 2017. Data from a total of 94 TIPS participants were monitored. Of the 94 participants, 30 participants chose to accept a Fitbit, and 64 participants declined a Fitbit (Fig. 2). In the 12-month period of observation, Fitbit users utilized Fitbits for an average of 328 days and logged an average of 462,028 total steps, with an average of 1,327 steps per day. Using our criteria for noncompliance, 33 non-Fitbit users and 2 Fitbit users were deemed noncompliant (Fig. 2).
All TIPS participants also engaged in weekly monitoring of vitals' data, which captured measurements on SBP, DPB, HR, Wt, and SpO2 (Table 1). Independent t-tests between Fitbit users and non-Fitbit users showed no statistically significant differences in any health biometrics monitored as part of the TIPS initiative. However, across all participants, regardless of Fitbit usage, SBP was on average 6.5 mmHg lower, which was statistically significant (p < 0.004). In addition, we noted a trend of reduced DBP across all TIPS participants (mean: −3.6 mmHg; p = 0.06) that may become significant with a larger sample size.
Participant Characteristics and Physiological Biomarkers for Non-Fitbit and Fitbit Users (Mean ± Standard Deviation)
DBP, diastolic blood pressure; HR, heart rate; LT, long term; SBP, systolic blood pressure; SpO2, blood oxygen saturation; ST, short term; Wt, weight; Δ, difference between pre- and postvalues.
Discussion
After comparing Fitbit users and non-Fitbit users, no significant differences in the deltas for SBP, DBP, HR, Wt, or SpO2 were noted. However, across all participants, there was a significant decrease in SBP associated with extended participation in the TIPS, which agrees with previous work showing that remote patient monitoring programs can be effective in improving health outcomes. 14 Since the significant reduction in SBP was seen in both Fitbit users and non-Fitbit users, it is unlikely to be a consequence of Fitbit usage. This finding concurs with existing literature surrounding the nonsignificant impact of health care wearables on health biomarkers and physical activity. 7,8
It is important to note that no incentives were used to encourage TIPS participants to accept or use the Fitbits that were offered as part of this program. As such, 68.1% of participants chose to not accept the Fitbits at all, and among participants who accepted the Fitbit, one-third used their Fitbit for <6 months before discontinuing use altogether. Many studies observe higher performance of health care wearable users if presented with personalized feedback or interventions. 15,16 To supplement users' interactions with activity tracking devices, customized automated messages or tailored interventions can better reinforce user engagement and positive behavioral changes. 6,15,16,17 Perhaps if TIPS participants had been offered Fitbit technology as part of a social program with personalized feedback and other forms of social reinforcement for meeting physical activity goals, the outcome of this program may have been different.
As a limitation for the study, we relied on objective step-count data from the Fitbit to make inferences on activity level. Although we must account for possible discrepancies between actual activity and activity recorded, Fitbit trackers have shown to be sufficiently accurate to monitor and give feedback on step counts. 18,19
Fitbits and other health wearables are reliable for the purpose of physical activity tracking and patient monitoring. However, Fitbits may not entirely meet their intended goal of inducing sustained physical activity or long-term significant positive influence on physiological biomarkers. Additional features, such as text message prompts or personalized feedback, may improve adherence, ease of usage, and the benefits of these devices. Meanwhile, community-embedded chronic disease management initiatives such as TIPS continue to reduce hospitalization rates and improve health outcomes for older individuals.
Footnotes
Acknowledgments
The authors acknowledge the TIPS participants, TTAs, and registered nurses for their important contribution to the acquisition of data for this project. This work was made possible due to a generous donation from the Harry and Jeanette Weinberg Foundation.
Disclosure Statement
No competing financial interests exist.
Authors' Contributions
D.S., J.M., C.P., J.S., M. Capasso, and M. Carpenter contributed to the study concept and design, data collection, and article preparation. E.H., A.N.J., A.S., E.B., G.U., and L.T. performed data analysis and interpretation and article preparation. All authors read and approved the final version.
Funding Information
This work was made possible due to a generous donation from the Harry and Jeanette Weinberg Foundation.