
Abstract
Background:
Telemedicine is not significantly spreading globally and large variations in its availability and use exist internationally. Although many factors already inhibit the dissemination of telemedicine, its complexly intertwined factors make it more difficult to solve this problem. This study aimed to analyze and visualize relationships among factors inhibiting the dissemination of telemedicine. We applied the interpretive structural modeling method and cross-impact matrix multiplication applied to classification analysis.
Materials and Methods:
Factors inhibiting the dissemination of telemedicine in Japan were extracted by literature review and hearing from four medical informatics experts belonging to a university or hospital using the Kawakita Jiro method.
Results:
Eighteen factors were extracted as those inhibiting the dissemination of telemedicine service in Japan: initial and operation cost, research data, legal development, profitability, usability, human resources, image quality, network speed, information security, technical limitation, restriction for clinical practice, practice continuity, target use case, burden for physicians, respondence, risks for clinical safety, understanding of medical staff, and understanding of patients. The hierarchical structure chart showed a nine-level structure and the cross-impact matrix showed the relationship among factors and the classification of them inhibiting the dissemination of telemedicine.
Discussion:
We found that the underlying factors were high implementation and operation costs, low research data, and risks for clinical safety. Implementation and operation costs, research data, legal development, and profitability have high driving power; thus, it is expected that the elimination of these inhibiting factors would lead to the dissemination of telemedicine.
Conclusions:
There are many kinds of factors inhibiting the dissemination of telemedicine in Japan. The result of this showed the structure of these factors visually and could be useful to solve the problem inhibiting the dissemination of telemedicine effectively and efficiently.
Introduction
Telemedicine is a medical service using information and communication technology. However, it is not significantly spreading globally, compared with the electronic medical record, computerized physician order entry, or electronic health record systems. In addition, large variations exist in the availability and use of telehealth and personal electronic health records among countries. 1
The factors inhibiting the dissemination of telemedicine are mentioned in several reports. The World Health Organization's Global Observatory for eHealth (2016) surveyed member states about the barriers to m-health implementation and revealed main barriers, including conflicting health system priorities, knowledge concerning the possible applications, policy, cost-effectiveness of solutions, legal, and operation cost. 2 In high-income countries, priorities, cost-effectiveness, and legal systems were the most important barriers. A report of Europe Commission mentioned that telemedicine barriers exist in all countries but do not affect them to the same degree. 3 Such barriers are considered equally applicable to factors inhibiting the dissemination of telemedicine.
In Japan, the Japanese Telemedicine and Telecare Association report 4 mentioned that the establishment of a foundation in telemedicine, information and communication technology, and medical technology has sufficiently progressed. However, the report revealed that medical education, educational systems, and delay in establishing policy perspectives in telemedicine development are problematic. The report also stated incidental issues such as delays in developing the prospects of social experts and confounding of health and industrial policies. Although there are already several report showing many factors inhibiting the dissemination of telemedicine, the complexly intertwined factors make it more difficult to solve this problem. Furthermore, it is not easy to understand the overall picture of these connections, even if one knows the relationship of each factor. In such a situation, it is important to gain a complete picture through visualization of the inhibiting factors.
The interpretive structural modeling (ISM) is a method for identifying complex relationships among specific items, by defining a problem or an issue. 5 –7 The ISM method has been applied to numerous studies, including those evaluating senior daycare center locations, evaluating the workflow of radiation therapy, and extracting factors influencing escalator-related incidents. 8 –17 However, there are no studies on the factors inhibiting the dissemination of telemedicine using the ISM method.
This study aimed to analyze and visualize relationships among the factors inhibiting the dissemination of telemedicine; we applied the ISM method and cross-impact matrix multiplication applied to classification (MICMAC) analysis.
Materials and Methods
ISM is a multivariate analysis method that determines the mutual relationship between factors by a pairwise comparison and performs a logical operation on the result to structure each element. The ISM method can visualize a problem composed of many factors as a hierarchical model of the factors. In addition, structural models could be expressed as causal relationships between elements in a directed graph based on graph theory, through which the implicit relationship between the factors can be clarified.
In this study, factors inhibiting the dissemination of telemedicine in Japan were extracted through a literature review and consulting from four medical informatics experts belonging to a university or hospital using the Kawakita Jiro (KJ) method. 2 –4 Experts wrote the candidate factors on a card exhaustively and then grouped similar factors through discussion. Finally, factors were decided in reference to the literature review. In extracting factors, telemedicine was assumed to include communication of any type of data, such as text, images, videos, and voices, and comprising both doctor-to-doctor and doctor-to-patient communication.
The extracted factors were calculated based on the structured hierarchy analysis. First, the relationship between each factor was determined using the one-pairwise comparison. Then, the adjacency matrix and reachability matrix were calculated, and relationships. After iteratively fixed the relationship among factors, the hierarchical model of factors inhibiting the dissemination of telemedicine was constructed.
In addition, the degree of association and influence were calculated from the sum of rows and that of columns of the reachability matrix using the MICMAC analysis. These were depicted in a 2-dimensional scatter plot, in which inhibiting factors were divided into four clusters by driving power axes and dependence power axes. The characteristics of inhibiting factors were evaluated with the following four clusters: (1) autonomous factors, (2) dependent factors, (3) linkage factors, and (4) independent factors.
Results
The following 18 factors were extracted as factors inhibiting the dissemination of telemedicine service in Japan.
INITIAL AND OPERATION COST
The initial cost for secure networks and hardware/software that medical institutions need to initiate telemedicine inhibits the dissemination of telemedicine. Operation costs include daily labor and maintenance costs. The cost of updating equipment is also expensive, but it is required every few years.
RESEARCH DATA
In Japan's insurance system, telemedicine is positioned to complement face-to-face consultations. To change this position, evidence of the safety and effectiveness of telemedicine is necessary. However, there is very little evidence about telemedicine, which demonstrate the same safety and effectiveness as face-to-face consultations. The insufficient research and case reports on telemedicine are factors that inhibit the dissemination of telemedicine from an evidence-based medicine perspective.
LEGAL DEVELOPMENT
The current Japanese medical practitioners' law enacted in 1948 has considered only face-to-face consultations but not telemedicine. The current laws and regulations related to doctors' use of telemedicine are unclear and hinder them from venturing into telemedicine. Specifically, online medical treatment using smartphones considers a limited number of target diseases, and there are many restrictions on medical treatment rules.
PROFITABILITY
Under the Japanese universal health insurance system, medical fees set by the government have a significant effect on the profits of medical institutions. 18 The current cost of telemedicine is very low, although there are many restrictions on accounting for medical fees. It is difficult to cover the costs of installation and operation with the income obtained as medical fees by telemedicine. Poor profitability compared with face-to-face consultation has inhibited the dissemination of telemedicine.
USABILITY
Since the general functions and configuration of the telemedicine system are not unified and the communication standard of the application may be different for each manufacturer, it is necessary to prepare dedicated systems and equipment for each remote medical care partner or medical institution. The usability differs depending on the telemedicine system might inhibit the dissemination of telemedicine.
HUMAN RESOURCES
There are few information technology (IT) staff in medical institutions in Japan. Shortage of staff who are familiar with IT and can operate telemedicine systems make difficult to disseminate telemedicine.
IMAGE QUALITY
The doctors' view when using a videophone may be different from that using the naked eye. Image quality such as color information is important in determining the patients' health. The color of the videophone must be adjusted to be the same as the naked eye. Lack of quality assurance for telemedicine systems can inhibit the dissemination of telemedicine.
NETWORK SPEED
To use telemedicine, it is necessary to connect to a high-speed network. However, in rural areas, network infrastructure providing high-speed internet service has not been sufficiently established. The inadequate guaranteed high-speed and stable traffic on the network will inhibit the dissemination of telemedicine.
INFORMATION SECURITY
Connecting to the internet increases the risk of leaking personal information. To connect to the internet, it is necessary to take enough security measures. The cost of implementing security measures has inhibited the dissemination of telemedicine.
TECHNICAL LIMITATION
Technical constraints due to inadequate establishment and standardization of basic technologies for telemedicine (medical information systems, networks, and equipment) inhibit the dissemination of telemedicine. Insufficient verification of the usability of the product also inhibits the dissemination of telemedicine.
RESTRICTION FOR CLINICAL PRACTICE
Usual clinical diagnosis is performed based on the physicians' knowledge and experience using inspection, palpation, auscultation, and percussion. However, the current telemedicine technology can use only a few of these means. So, limited medical information can be obtained from telemedicine.
PRACTICE CONTINUITY
When a service failure occurs in a telemedicine system due to a disaster or technical trouble, medical practice using telemedicine cannot be performed. Concerns about this risk of telemedicine services inhibit its dissemination.
TARGET USE CASE
Telemedicine is mainly expected to benefit patients in remote areas and remote islands with low accessibility to large hospitals. The current health insurance system in Japan specifies a few diseases that are eligible for doctor-to-patient telemedicine and other patients are ineligible for telemedicine. However, with the dissemination of online services such as smartphones and social networking services, targets with patients' needs are spreading from a population living in remote areas to a businessperson in urban areas. The mismatch between the needs of telemedicine and currently eligible diseases might inhibit the dissemination of telemedicine.
BURDEN FOR PHYSICIANS
The operation of telemedicine is divided into two cases, one in which physicians only perform telemedicine, and another in which physicians perform telemedicine combined with a regular medical practice schedule. Performing telemedicine in addition to regular medical practice might increase the burden on physicians. Inefficient physicians' workflow and inefficient schedule management would inhibit the dissemination of telemedicine.
RESPONDENCE
The responsibilities in the event of a medical accident resulting from the use of telemedicine or the disadvantage of a patient or health care professional due to the failure to use telemedicine are not fully discussed. Unclear responsibility leads to physicians' risk-aversive behavior, which is a major factor inhibiting the dissemination of telemedicine.
RISKS FOR CLINICAL SAFETY
It is unclear whether the risk of misdiagnosis is the same between telemedicine and normal practice. Clinicians will avoid the uncertain risks of using telemedicine in practice. This might be one of the factors inhibiting the dissemination of telemedicine.
UNDERSTANDING OF MEDICAL STAFF
Staff training may be required to begin telemedicine operations. If physicians or medical staff need considerable training on using telemedicine systems and education on legal regulations and safety considerations, the burden of preparing and implementing education will inhibit the dissemination of telemedicine. Moreover, understanding of medical staff includes constructing relationships between the hospital and patients, among hospitals, and among staff. Staff development is necessary to avoid the resistance to change among medical staff.
UNDERSTANDING OF PATIENTS
Perceptions of telemedicine depend on the individual patient. Patients may consider telemedicine to be less secure than face-to-face practice. Inadequate understanding of patients becomes a factor inhibiting the dissemination of telemedicine.
Tables 1 and 2 show the adjacency matrix and reachability matrix of factors inhibiting the dissemination of telemedicine. Figure 1 shows the hierarchical structure of the factors inhibiting the dissemination of telemedicine in Japan, obtained through ISM analysis. The structure of factors inhibiting the dissemination of telemedicine are divided into nine levels starting with “(1) Initial and operation cost,” “(2) Research data,” and “(16) Risk for clinical safety” leading to “(17) Understanding of medical staff” and “(18) Understanding of patients.” Figure 2 shows the result of MICMAC analysis. Autonomous factors (Cluster I) were “(5) Usability,” “(7) Image quality,” “(9) Information security,” “(10) Technical limitation,” “(15) Respondence,” “(16) Risk for clinical safety,” and “(18) Understanding of patients,” which have weak driving and dependence power. Dependent factors (Cluster II) were “(12) Practice continuity,” “(13) Target use case,” and “(14) Burden for physicians,” which have a strong dependence power and weak driving power. There were no elements in Linkage Factors (Cluster III). Independent factors (Cluster IV) were “(1) Initial and operation cost,” “(2) Research data,” “(3) Legal development,” “(4) Profitability,” and “(6) Human resources,” which have a strong driving power and weak dependence power and are independent of these relationships. “(11) Restriction for clinical practice” and “(17) Understanding of medical staff” were on the border between Clusters I and II. “(8) Network speed” was on the border between Clusters I and IV.

Hierarchical structure chart of the factors inhibiting the dissemination of telemedicine.
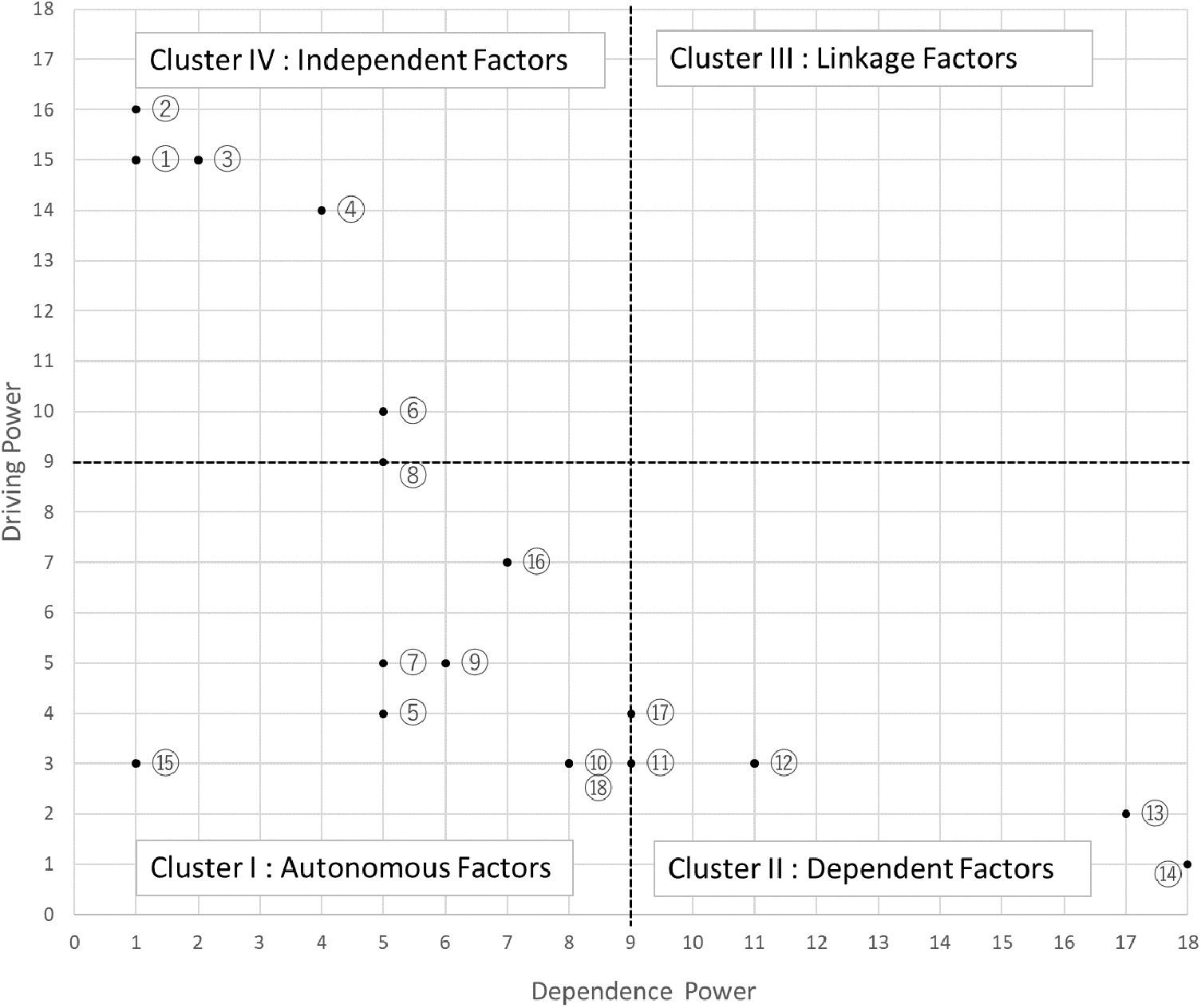
Method and cross-impact matrix multiplication applied to classification analysis of factors inhibiting the dissemination of telemedicine.
Reachability Matrix of Factors Inhibiting the Dissemination of Telemedicine
Adjacency Matrix of Factors Inhibiting the Dissemination of Telemedicine
Discussion
As a sociomedical background in Japan, principles of face-to-face care were stipulated in the Doctors' Act in 1948, and telemedicine was virtually forbidden in Japan. In 1997, the Ministry of Health, Labour and Welfare in Japan (MHLW) established the telemedicine in isolated islands, isolated districts, and mountainous areas. In 2003, the MHLW initiated telemedicine for certain chronic diseases. However, medical personnel understood the statement as white list and the face-to-face care is still forbidden in first medical care. In 2015, MHLW revealed a new definition of telemedicine, which admitted that former statement such as those on chronic diseases are an example. At present, the Japanese government views telemedicine as an area for strengthening development, and the number of venture companies and medical institutions that provide telemedicine is increasing compared with the past. In the medical insurance fee chart, which is revised every 2 years, the coverage of online practice is expanding. However, the use of telemedicine is not sufficient enough in Japan.
This study extracted numerous factors inhibiting the dissemination of telemedicine. The results show the hierarchical structure of such factors in Japan. We found that the underlying factors at level 1 were high implementation and operation costs, low research data, and risks for clinical safety. Moreover, levels 2 and 3 had legal development and profitability. Particularly, implementation and operation costs, research data, legal development, and profitability have high driving power; thus, the elimination of these inhibiting factors is expected to lead to the dissemination of telemedicine.
The following measures are conceivable for addressing the inhibiting factors. To reduce implementation and operation costs, standardization and certification systems are effective. Proper security measures are important in telemedicine use. The security guideline should be built as a minimum requirement, and the product certification based on the guideline prevents users from incurring unnecessary costs. Developmental costs can be reduced through communication between the electronic medical record and the picture archiving and communication system using standard mechanisms. Despite empirical research on Japan's basic technologies, there are insufficient reports on the cost-effectiveness and safety of telemedicine. 19,20 The barriers to telemedicine can be overcome by investigating patient needs and conducting research to verify the safety and effectiveness of applying telemedicine to areas with a high need for it. Legal development needs to define the responsibilities of health care and medical providers and facilities assuming the use of telemedicine.
In terms of profitability, to operate telemedicine, communication equipment and a medical information system are required. In addition, communication and human resource costs for system maintenance are incurred as regular costs. Particularly, to operate telemedicine, it is necessary to train and deploy human resources who understand medical knowledge, IT, and information security. Telemedicine needs a billing mechanism that can cover these costs, but it has a low priority in the national budget for medical expenses; it is thus difficult to provide sufficient medical fees for telemedicine now in Japan. However, in Japan, where the population is aging rapidly and countryside is depopulated, telemedicine could be the infrastructure supporting community medicine. As Japanese government views telemedicine as a growth area, research showing the health-economic benefits of the introduction of telemedicine is important for profitability.
LIMITATION
In this study, the inhibiting factors were extracted and related by brainstorming from four researchers belonging to universities and hospitals in Japan. Because brainstorming includes subjective factors, the result of factors and associations might be changed depending on the targets' domain or position. As there are various modes of telecommunication, including telephone and real-time video in telemedicine, future research is necessary to identify the variations in the inhibiting factors for each mode.
Conclusions
This study applied the ISM method and MICMAC analysis to analyze and visualize relationships among factors inhibiting the dissemination of telemedicine. Such factors in Japan were extracted by literature review and hearing from four medical informatics experts belonging to a university or hospital using KJ method. Based on the result, 18 factors were extracted as factors inhibiting the dissemination of telemedicine service in Japan. The hierarchical structure chart showed a nine-level structure and the cross-impact matrix showed the relationship among factors and classification of them inhibiting the dissemination of telemedicine. There are many kinds of factors inhibiting the dissemination of telemedicine in Japan. The result of this study showed the structure of these factors visually and could be useful to solve the problem inhibiting the dissemination of telemedicine effectively and efficiently.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.