
Abstract
Introduction:
The coronavirus 2019 (COVID-19) pandemic has become a major world health problem. All U.S. states have advised their cystic fibrosis (CF) populations to socially isolate. Major health care payors such as Medicare and most private insurance companies have agreed to reimburse health care providers for telemedicine and telephone visits.
Methods:
The CF adult team at the University of Virginia (UVA) transitioned from face-to-face clinics to multidisciplinary telemedicine clinics by using WebEx® (Cisco Systems, San Jose, CA), a Health Insurance Portability and Accountability Act of 1996 (HIPAA) compliant platform.
Interventions:
Patients were contacted before scheduled visits and triaged into: (1) patients eligible for the multidisciplinary telemedicine clinic, (2) patients to be seen in clinic urgently due to acute needs, and (3) stable patients who can be rescheduled at a later time. Ineligible patients for the telemedicine clinic due to lack of access to technology were followed up via telephone.
Results:
A total of 63 patients were scheduled to be seen in the UVA clinic over 4 weeks, 10 clinic days. Of these patients, 20 (32%) rescheduled their appointment. In addition, 2 patients (3%) were seen in clinic for acute needs and 38 (60%) were seen by the multidisciplinary team through telemedicine.
Conclusions:
In the context of the COVID-19 pandemic, implementing a telemedicine clinic process that serves the needs of a multidisciplinary care team is paramount to preserving the CF care model. Through a systematic design and test process, a feasible and sustainable program was created that can be utilized by other multidisciplinary programs to adapt to their context.
Background
Cystic fibrosis (CF) is a systemic genetic disorder affecting ∼30,000 people in the United States 1 and at least 70,000 people worldwide. 2 CF is caused by abnormal function of the cystic fibrosis transmembrane conductance regulator (CFTR). 3 CFTR dysfunction leads to systemic changes in mucus viscosity, with multiple organs being involved, most commonly affecting the lungs, pancreas, and liver. Lung involvement is characterized by chronic infection and inflammation and results in progressive lung disease and premature death due to respiratory failure. Early identification of acute lung infections or CF exacerbation can restore lung function and improve lung function decline. 4 Cystic Fibrosis Foundation (CFF) care guidelines recommend close monitoring of forced expiratory volume in one second (FEV1) in clinic every 3 months. Our patient data (not published) also showed that low quarterly clinic visit compliance is associated with increased exacerbation rates and low FEV1; we suspect patients who do not regularly present to clinic to develop exacerbations that are not identified in a timely manner, and to often end up reaching out for care only through hospitalization. Many patients with CF travel a long distance to reach a specialized CFF accredited center. One-third of patients seen in our clinic travel more than 100 miles for their appointment. The travel distance leads to increased transportation and lodging cost as well as patients and caregivers needing to take days off work for a clinic visit. This is the norm worldwide.
Telemedicine has been used across the world to minimize cost and improve access to care for CF patients who are located at long distances from their closest CF specialized center. 5 –13 Jamie Woods' group showed increased clinic participation and early detection of CF exacerbations when telemedicine was introduced in lieu of clinic visits in Western Australia. 12 Telemedicine has been used to improve physical activity and nutrition in CF patients with some success; it has been shown to decrease the cost of clinical trials when employed for monitoring of FEV1 and side effects 14 –16 and to be a good tool for pre- and post-transplantation evaluation of respiratory symptoms, anxiety, and lung function decline. 9,17 However, data related to patient outcomes are scarce; most of these telemedicine studies are pilot and feasibility studies and lack long-term data in lung function stability and survival.
The coronavirus 2019 (COVID-19) pandemic has become a major world health problem. Multiple countries have recommended social distancing as part of a global effort to decrease person-to-person transmission of COVID-19. All U.S. states have advised their population to stay indoors, and major health care payors such as Medicare and most private insurance companies have agreed to reimburse health care providers for telemedicine and telephone visits. Health Insurance Portability and Accountability Act of 1996 (HIPAA) compliance lenience policies related to telemedicine utilization have been introduced in an effort to decrease health care-related COVID-19 spread, and as a result, multiple organizations have been working diligently on transitioning face-to-face clinics to telemedicine clinics. To continue quarterly FEV1 and symptom monitoring as recommended by the CFF and to timely identify episodes of exacerbation, our team has instituted a protocol to transition to telemedicine clinics.
The process of transitioning to telemedicine clinics for regular patient follow-up is complex for multidisciplinary teams who work with chronically ill patients, such as CF patients, especially in the context of social distancing imposed by the COVID-19 pandemic with multiple health care providers working from home. We describe our protocol as an example that could be employed by other clinics.
Aim
Our aim was to develop a standardized and sustainable process to transition from face-to-face clinic visits to telemedicine visits in the adult CF clinic at University of Virginia (UVA). It was important to work on this urgently to minimize patient contact and risk of infection, and to encourage and promote social distancing for CF patients in the context of the COVID-19 pandemic.
Methods
Pre-Clinic
At the beginning of the week, patients who are scheduled to be seen in the regular clinic that week are called by the clinic coordinator (multiple team members divide the work) to discuss the upcoming clinic visit. They are screened for pulmonary symptoms suggestive of COVID-19 or CF exacerbation (patients are asked whether their respiratory symptoms are at baseline or whether they have any of the following: fever, cough or shortness of breath, or any other health issues) and technological capability. A device with camera/microphone and strong internet connectivity is required for telemedicine. Any of the following devices are acceptable: iPad, smart phone, personal computer, laptop, etc.
If the patient is deemed clinically stable and owns appropriate technology for a telemedicine visit, the patient is asked whether they would like to transition their visit to telemedicine or reschedule the standard visit to a later time; they are encouraged to participate in telemedicine. Further consent for participation in telemedicine encounter is obtained at the beginning of the telemedicine visit.
If the patient reports respiratory symptoms, the clinic nurse coordinator screens for whether they should come in person to clinic or whether there is a reason for them to be evaluated in a specially designed COVID clinic or to present to the Emergency Department for further evaluation. If necessary, she consults with the physician.
If the patient has no respiratory symptoms and is deemed clinically stable, but he or she does not own the technology required for telemedicine, the clinic coordinator reschedules the patient for a routine visit at a later time.
If necessary, the physician will call the patient and will document a telephone encounter.
Subsequently, the clinic coordinator sends a list of patients to the telemedicine coordinator to create WebEx® (Cisco Systems, San Jose, CA) invitations for patients who are going to participate in the telemedicine clinic. This is an HIPAA-compliant platform supported by our organization's information technology (IT) group.
The telemedicine coordinator (multiple team members share this role) sends WebEx invitation to patients and team members by using appointment time and patient initials as identifiers.
The clinic schedulers are informed to keep the patients active on the EPIC® (Epic Systems Corporation, Verona, WI) schedule for a telemedicine visit as they would for their regular clinic visit (Fig. 1).
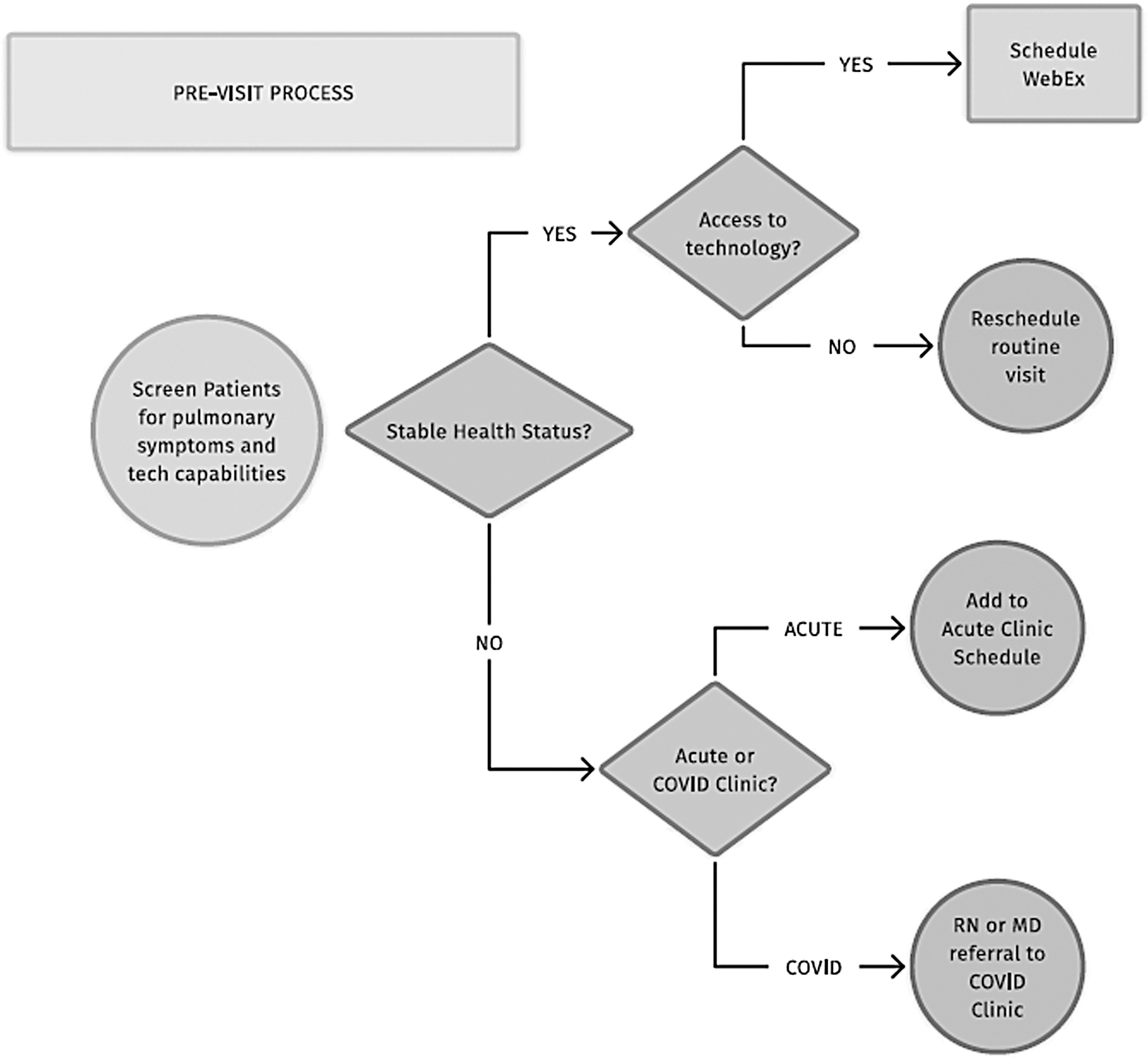
UVA CF adult pre-clinic process map; starts with screening patient for type of visit and finishes with patient schedule for encounter. CF, cystic fibrosis; HIPAA, Health Insurance Portability and Accountability Act of 1996; HIPAA compliant COVID clinic, designated clinic to test and triage patients suspected being COVID positive; MD, Medical Doctor; RN, Registered Nurse; UVA, University of Virginia; WebEx®, virtual platform.
Day of Clinic
The team members huddle in a virtual WebEx Workroom and fill out a clinic flow sheet/or patient tracking sheet (maintained in a shared Google® doc [Google, Inc., Menlo Park, CA] without patient identifiers) with subspecialty members who will see the patients (respiratory therapist [RT], registered dietitian [RD], social worker [SW], nurse coordinator, and PsyD in addition to the physician); this process is very similar to the process created at UVA for a regular in-person clinic day.
The team shares the patient tracking sheet with the MDs so they are aware of who else requests to see the patient.
The telemedicine coordinator (this role is shared between several team members and WebEx access) starts patient WebEx meetings 15 min before appointment time and monitors the virtual “room” for patient arrival.
On patient arrival in the virtual WebEx room: a. The telemedicine coordinator sends the team group text notification. b. The flow coordinator notifies the clinic schedulers to check in the patient as they would do if the patient is present in clinic. They also schedule the patient under a different encounter type created by the organization called Prof Remote Visit.
The telemedicine coordinator has the first clinical encounter to gather intake data, present a visit itinerary to the patient, and ask whether they want to see other subspecialty team members. Once the itinerary is finalized with the patient's input, the telemedicine coordinator types in the itinerary in the patient's chat box and into the team members' flow sheet/communication board.
The clinic respiratory therapist (RT) enters the virtual encounter next (if they are not also the telemedicine coordinator), coaches the patient on performing spirometry, collects spirometry data, sends a group text notification when finished with the patient, and returns to the workroom to update the Google flowsheet and prompt the next team member to enter the patient's WebEx virtual room. She also notifies the team regarding FEV1 levels, if the patient owns a spirometer.
Subsequent team members enter times in and out in the Google sheets and send group texts when going in and out of the patient's WebEx room.
When the visit is concluded, the last team member informs the patient whether the appointment is concluded and that they can log off.
The physician writes the note, bills for telemedicine visit, closes the note, and communicates via EPIC with the nurse coordinator regarding follow-up laboratory tests and follow-up visits (Fig. 2).
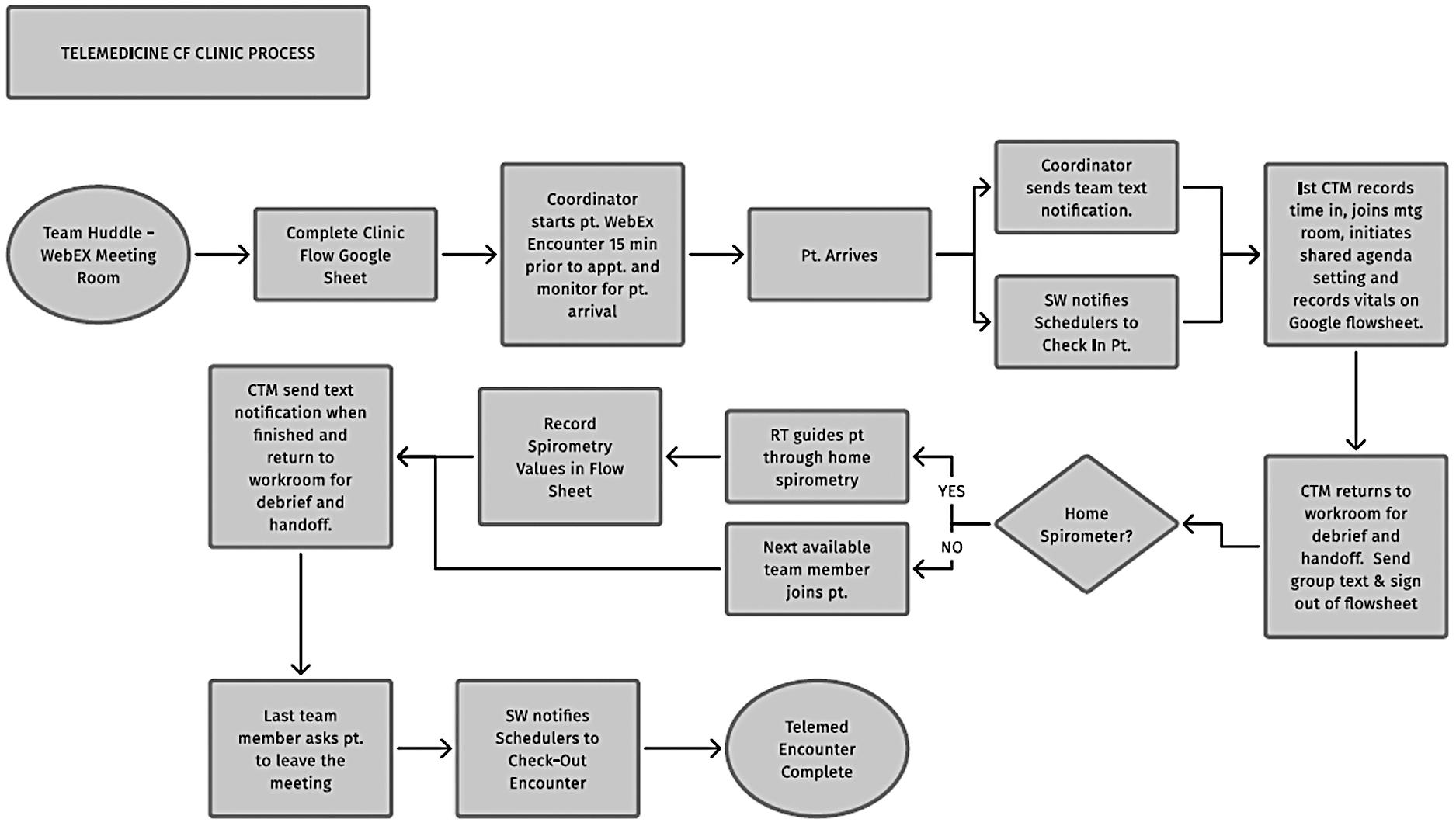
UVA CF adult clinic process map; starts with huddle in the team WebEx work room and finishes with completion of patient encounter. CTM, care team member; RT, respiratory therapist; SW, social worker.
Post-Clinic
The nurse coordinator communicates with the patient, arranges for follow-up laboratory tests, and coordinates a follow-up appointment with the clinic.
The team discusses the process, idea for improvement, and implementation with next visit. The organization changes for the telemedicine process are taken under consideration.
Measures
We recorded patient data in a health information and technology (HIT) organization-maintained HIPAA-protected server. All data are collected with each visit, in real time. We ran multiple Plan Do Study Act (PDSA) cycles, and we adapted and perfected our process with each visit (Fig. 3).

Plan-Do-Study-Act schematic of the Cystic Fibrosis Adult Clinic; with each clinic visit, the process is perfected by the team. At the end of the clinic and at the end of the week, we discuss the process and idea of improvement.
Data collected
The number of patients originally scheduled in clinic each clinic session, number of patients who decided to reschedule and refused a telemedicine encounter, number of patients who consented to telemedicine, number of patients ineligible to telemedicine due to lack of technology, number of patients eligible for telemedicine who tried to participate but had technical difficulties, number of patients seen with telemedicine and stable or unstable who required further interventions, spirometry data if available, and number of patients seen for acute needs in face-to-face clinics were assessed.
Results
A total of 63 CF patients were scheduled to be seen in regular clinic at UVA over 4 weeks, 10 separate days. Of these patients, 20 (32%) rescheduled their appointment either due to their preference (18 patients) or due to lack of technology (2). In addition, 2 patients (3%) were seen in clinic for acute needs and 38 (60%) were seen by the multidisciplinary team through telemedicine. Spirometry results were available for 12 out of 38 (32%) patients, and FEV1 was stable in all these patients. Four of the 38 patients had issues with connectivity, and the telemedicine visit was transformed into a telephone encounter. One patient was identified to have moderate exacerbation and was directed to the Emergency Department for further evaluation. Two patients had symptoms of mild CF and asthma exacerbation and were prescribed oral antibiotics and prednisone taper.
Discussion
Telemedicine implementation is feasible in the context of the COVID-19 pandemic for clinically stable patients and patients who have access to appropriate technology. Despite a thorough triage process to identify potential patients with acute health needs, with the telemedicine visits we identified a patient who needed acute care and immediate admission to the hospital. This patient received the intervention he needed and the telemedicine visit was, in fact, beneficial for his care.
Telemedicine has been used in time of crises in multiple different instances: during hurricanes Harvey and Irma, during the SARS (Severe Acute Respiratory Syndrome) pandemic in China in 2003, and in Australia during long periods of droughts. In a similar manner, changing regular clinics to telemedicine clinics could be beneficial for U.S. medical systems in the context of the COVID-19 pandemic when implemented strategically through a well-designed process and incorporating appropriate HIPAA-compliant platforms, organizational support, and insurance reimbursement. 18
With the state and federal imposed social distancing to reduce spread of COVID-19 infection, multiple regular clinics closed, causing financial hardship among multiple medical entities. On March 27, 2020, the USA Critical Care Society Collaborative (The American Thoracic Society, The American College of Chest Physicians, The American Association of Critical Care Nurses, and The Society of Critical Care Medicine) urged the federal administration to strengthen the social distancing requirements in a continuous effort to contain the viral spread. These restrictions can lead to further financial loss for medical organizations. With expanded Medicaid, Medicare, and private insurance reimbursement for telehealth, the introduction of telemedicine will partially offset the financial loss and medical practices may remain functional. This will allow organizations to continue to support their employees, allow employees to work effectively from home, and cover health care benefits, which will ultimately lead to a gain for the medical society and community overall. In addition, patients and team members will have reduced exposure to infection, subsequently decreasing the hospitalization and health care cost overall. Through telemedicine, chronic disease patients may continue to receive regular health monitoring in the context of social distancing. However, patient buy-in is very important and it is currently a limiting factor to utilizing telehealth. As seen in our results, 32% of our patients preferred to reschedule to a future regular face-to-face visit rather than participate in virtual clinics. This is a new health care modality and it will require time for patient and team adaptability.
Technology seems to be another limiting factor in further utilizing telemedicine. We are currently collecting extensive data on technology needs in our CF adult patients to implement telemedicine across the entire population. Residents of rural areas could have the necessary equipment but might lack access to high-performance internet access. Despite having a computer, camera, and microphone, the internet connection quality needs to be appropriate for the teleconference to be successful. In the context of the COVID-19 pandemic, telemedicine will most likely become a standardized way of monitoring patients with chronic disorders and ensure their disease control without exposing them to the risk of COVID infection. Employing IT expertise on expending internet access in rural underserved areas in the United States would increase IT jobs, ensure job stability for people with this expertise, and support the economy in these areas. In addition, encouraging large enterprises such as Apple and Samsung to support this effort through charity (e.g., donating smart phones) would further increase the use of telehealth.
A standardized approach to care and access to technology is necessary to ensure a smooth clinic operation. One of the most important factors in running a multidisciplinary telemedicine clinic is communication via an HIPAA-compliant platform, either chat or a virtual work room. Organizational support and stakeholder buy-in are paramount for this operation to be successful. Multiple specialty members need to communicate and collaborate regarding patients' specific needs. Having a safe HIPAA compliant work room in which members can chat is important for team care.
More so, standardization and sustainability/reproducibility of telehealth process is very important. We do not recommend reinventing the wheel with each clinic day, but rather establishing a process that can be reproduced easily each time. We have diligently worked on perfecting our process by using the quality improvement (QI) tool of PDSA cycles. This CF multidisciplinary clinic model can be implemented by other CF multidisciplinary clinics and other multidisciplinary groups working with other patient populations such as Interstitial Lung Disease, Amyotrophic Lateral Sclerosis, etc.
Future Plans
Our UVA CF adult team applied for organizational grant support to obtain the technology required for future telemedicine clinics. In addition, spirometers for all eligible patients were ordered through grant support and are expected to be delivered to patients in the next couple of weeks. The access to home spirometry results will enable us to remotely monitor FEV1 stability in CF patients and identify early changes.
Conclusion
Urgently implementing a telemedicine clinic in the context of the COVID-19 pandemic crisis in the CF multidisciplinary clinic through a standardized process and using established QI tools is a feasible and sustainable process that can be utilized by other multidisciplinary programs. Having the organizational support in HIT to allow for implementation and billing of telemedicine visits is crucial to the success of this endeavor. Further studies are needed to evaluate patient outcomes when transitioning from face-to-face clinics to telemedicine clinics.
Footnotes
Acknowledgments
The authors would like to thank the UVA telemedicine group for their IT support with the clinic, their patient family partners Lauren Williamson and Jason Conyers for their input on creating the clinic flow, and Dr. Bruce Marshall and CFF and CFLN for their continuous support.
Disclosure Statement
Dana Albon has received grant funding from Vertex Pharmaceutical and has been consulting for Gilead and Vertex pharmaceuticals. For all other authors, no competing financial interests exist.
Funding Information
Cystic Fibrosis Foundation Care Center Grant (CFF CC043-AD): supported salaries for our Quality Improvement coordinators and principle investigator.
Cystic Fibrosis Learning Network Grant (CFLN SEID16AB0): supported salaries for our Quality Improvement coordinators.
Vertex Circle of Care Grant (CG-2016-105531): supported spirometers for home use in our CF clinic for 1/3 of our patients.
The funding organizations had no role in the design, implementation, interpretation, and reporting of these data.