
Abstract
Background:
Adherence to immunosuppressive medicine in lung transplant recipients is associated with improved long-term survival. Patient education and support from health care providers are key components. We investigated e-learning as a tool to improve lung transplant recipients' knowledge of post-transplant care such as hygiene, self-monitoring, travel precautions, vaccinations, and the importance of adherence to medication.
Objective:
To compare the effect of e-learning and conventional patient education with respect to level of knowledge and drug adherence. A single-center open randomized controlled trial design was used.
Methods:
Lung transplant recipients were randomized to an e-learning program or standard care. One month before a scheduled follow-up visit, the intervention group received a link by e-mail to a 15-min e-learning program. At the follow-up visit, all lung transplant recipients completed two drug adherence questionnaires (Basel Assessment of Adherence with Immunosuppressive medication Scales [BAASIS] and Transplant Adherence Questionnaire [TAQ]) and a questionnaire testing their knowledge of post-transplant care.
Results:
Fifty lung transplant recipients were randomized with 24 recipients in each group completing the study. Recipient adherence measured by BAASIS showed a tendency toward improved drug adherence in the intervention group compared with the control group (71% vs. 55%, p = 0.23). TAQ showed no difference between the two groups (p = 1.0). Recipients in the intervention group had a significantly higher number of correct answers to questions about transplant-friendly lifestyle (median 11 vs. 10, p = 0.02).
Conclusion:
A 15-min e-learning program is a simple and effective tool to improve lung transplant recipients' knowledge of post-transplant care.
Introduction
Lung transplantation is the ultimate treatment for severe chronic lung failure. Short-term survival of patients undergoing lung transplantation has increased during the past 20 years, but long-term survival has, however, remained unchanged with a median survival of 5.9 years in 2017. 1 The most frequent cause of reduced survival is chronic rejection. 1
Adherence to medication and a high level of self-care regarding hygiene, home monitoring, travel precautions, and vaccinations are important factors for long-term survival. 2 –5 Several studies show that adherence to immunosuppressive therapy regarding taking, dosing, and timing of medication is important. Even minor deviations from the prescribed immunosuppressive regimen, that is, taking <98% of the tablets or variability in timing of medication of >2 h, are related to increased risk of acute rejection, graft loss, and poor kidney function. 6 –10 Furthermore, transplant recipients tend to be less adherent over time 11,12 ; despite knowing this risk, nonadherence is common. 6
Several factors influence patient adherence: the number of drugs, the number of daily doses, and whether the drugs are free of charge or not, but also family relations and patients' coping ability play a role. 12,13 Challenges related to adherence among lung transplant recipients are similar to recipients of other solid organs. In addition, lung transplant recipients have to monitor their pulmonary function at home, which is difficult to remember for many patients. 3,6 Strategies to maximize adherence to both drugs and home monitoring are thus highly warranted. These strategies should be based on caregiver support with continuous and repeated efforts to improve adherence through education and supportive interventions.
Despite continuous patient education at follow-up visits, many patients remain nonadherent with respect to blood sampling, medication, and home monitoring. 14,15 A recent study showed self-reported nonadherence to immunosuppressive medication in 27.4% of lung transplant recipients. 16
All patients and their caregivers, enrolled in the Danish lung transplant program, are provided with a booklet made by the Danish transplant center at Rigshospitalet, Copenhagen. The booklet contains information about necessary precautions after lung transplantation and is handed out during recovery after transplantation. Before discharge from hospital and at every outpatient visit after lung transplantation, the patients receive repeated education of important topics, including sun protection, hygiene, the importance of taking and timing medication and blood sampling, peak flow home monitoring, symptoms, and how to react to these symptoms. 17 In a previous Danish study, individual interviews with five lung transplant recipients pointed at the importance of timing of patient education. 17 The aforementioned findings are supported by a mixed-method study from 2014, where lung transplant patients expressed a wish for education immediately before and after transplantation. However, there was a subset of topics that patients were interested in reviewing again. 18
In 2014, a randomized controlled trial showed that computer-based education was noninferior to conventional education and that computer-based education was a simple effective tool to improve adherence to immunosuppressive medication. 19
e-Learning has several advantages compared with conventional education. It is cost-effective and it is possible for the patients to gain information at their own pace and to go through the educational program when needed. Randomized studies in other patient groups have shown that e-learning at home after receiving conventional education significantly increased patients' knowledge. Patients with hemophilia increased their practical skills as well as their knowledge of the disease. 20 Patients with overactive bladder demonstrated increased knowledge, fewer symptoms, and increased empowerment after going through an e-learning program. 21 A study of two education methods in pretransplant patients showed a significantly higher knowledge of post-transplant care, less anxiety about transplant surgery, and a higher satisfaction with the education method for patients receiving computer-based multimedia education compared with conventional education. 22
Few studies have compared a conventional education program with an e-learning program in lung transplant recipients. The aim of this study was to investigate e-learning as a way to increase patients' knowledge of post-transplant care and increase adherence to immunosuppressive treatment.
Methods
Design
This was a single-center open randomized controlled intervention study. The study was approved by the Central Denmark Region Committee on Health Research Ethics (ID 1-16-02-497-14) and informed consent was obtained.
The E-Learning Program
An e-learning program was developed covering transplant topics from existing patient education materials used at transplant centers in Denmark. Topics included the importance of lung function monitoring by regular peak flow measurement, recognition of symptoms of rejection or infection, early contact to the transplant center in case of changes, adherence to immunosuppressive medication and blood tests, and knowledge of lifestyle recommendations, including sun protection, food, and vaccination (Table 1). The duration of the e-learning program was limited to 15 min to ensure focused attention from the patient.
Topics Included in the e-Learning Program for Lung Transplant Recipients
The e-learning program was developed by a transplant nurse (T.B.G.) and administered by e-mail to transplant recipients 1 month before participants in the intervention group had their next scheduled appointment at the transplant center. The program was developed as a PowerPoint presentation with voice-over narration.
The e-learning program was tested in three focus groups. Three lung transplant recipients from the Danish transplant center at Rigshospitalet in Copenhagen, Denmark, participated in the first focus group interview, and lung transplant nurses from Rigshospitalet and Aarhus University Hospital participated in the second and third interview (Fig. 1). The aim of the focus group interviews was to clarify if the e-learning program was sufficiently clear and understandable to patients, and to ensure the relevance of the topics. The interviews resulted in adding sections about sexuality and exercise. After the interviews, the e-learning program was approved by a lung transplant physician (E.B.) and a dermatology specialist. The e-learning program is shown as Supplementary Data S1.
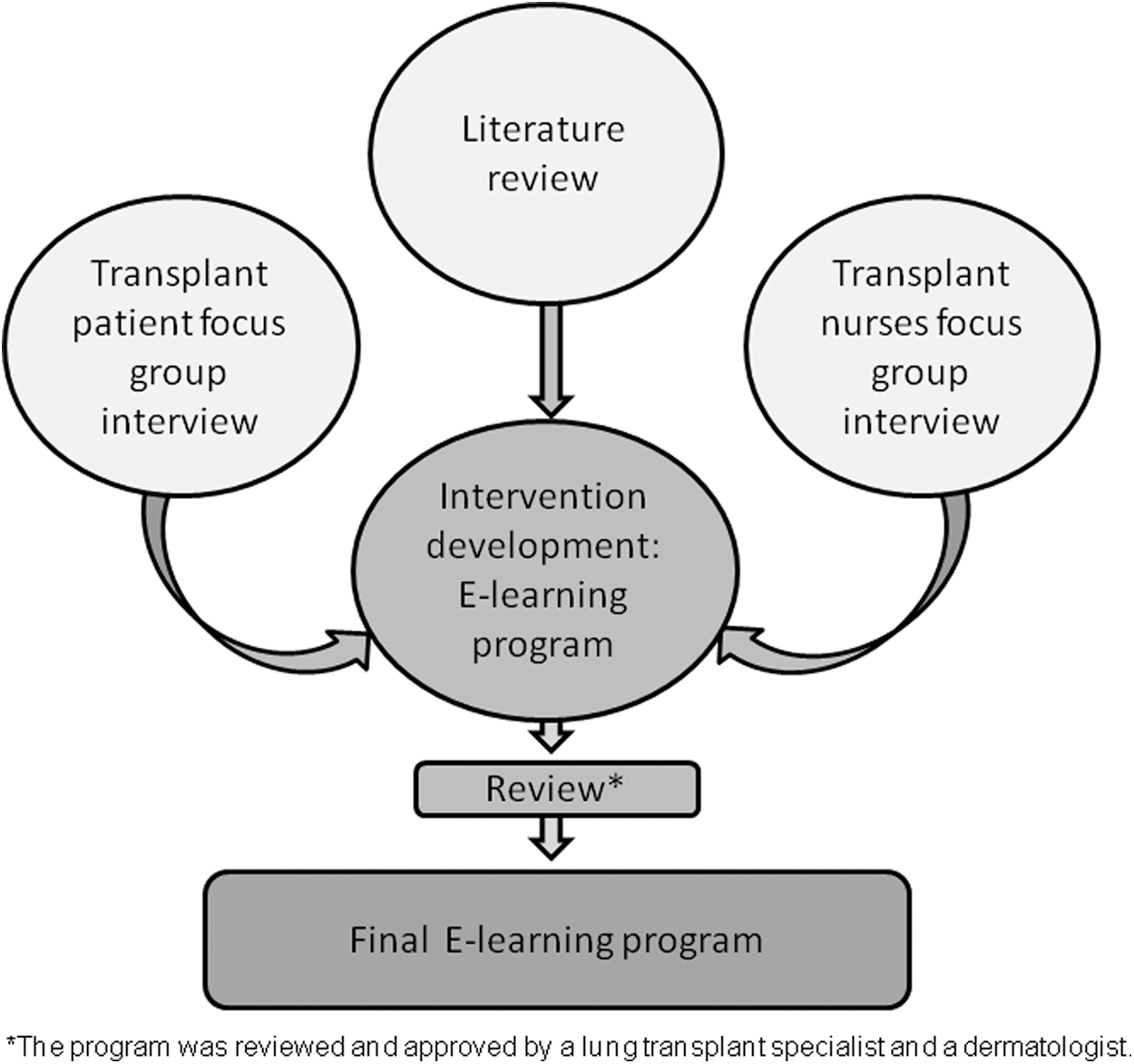
Development of the e-learning program.
Participants
Inclusion
All lung transplant recipients attending the post-transplant follow-up program at Department of Respiratory Diseases and Allergy, Aarhus University Hospital, Denmark, between January 2016 and August 2016 were invited to participate.
Eligible patients had received a lung transplantation >6 months before inclusion, they were >16 years of age, had access to a computer at home and an e-mail address, were able to speak Danish, and had a life expectancy of >6 months.
Patients were randomized in groups of 10 by random drawing of closed envelopes.
Information on age, gender, educational level, marital status, and time since transplantation was registered at the time of inclusion. Patients gave informed consent to participate in the e-learning program. One month before a scheduled follow-up visit, patients in the intervention group could access the e-learning program from home.
Follow up
At a follow-up visit after 1 month, all patients were asked to fill out three different questionnaires. All questionnaires were self-reported. Patients in the intervention group confirmed that they had seen the e-learning program and answered questions about their satisfaction with the e-learning program. The patients were treated by staff at the transplant center who were unaware of the randomization to either the intervention or the control group.
Questionnaires
Adherence to medication intake was assessed using the Basel Assessment of Adherence with Immunosuppressive Medication Scale (BAASIS) and the Transplant Adherence Questionnaire (TAQ), 3,10,23 which were completed by all participants. Both questionnaires are validated in patients with HIV; the BAASIS questionnaire has also been validated in renal transplant patients. 24 –26
The BAASIS questionnaire
The BAASIS questionnaire measures patients' taking, skipping, timing (>2 h from prescribed time) and dose reduction of drugs during the previous 4 weeks. BAASIS comprises four questions with a 6-point response scale ranging from never (0 points) to every day (5 points). 3,10 Scores 1–5 on any of the four items, (1) taking, (2) skipping, (3) timing, and (4) dose reduction, are considered as nonadherence. A score of 0 for each item is considered adherent. Overall adherence is scored in percentage on a visual analog scale.
The TAQ questionnaire
The TAQ questionnaire measures patients' taking, skipping, and timing of drugs during the past 4 days. 3,23 TAQ comprises six questions and patients are considered adherent if all doses are taken correctly.
Post-transplant care questionnaire
A new questionnaire examining patients' knowledge of post-transplant care and insight into the treatment was developed for the purpose of this study. It included questions related to the topics in the e-learning program (Supplementary Data S2). The questionnaire comprises 13 multiple choice questions and has been face validated 27 among lung transplant recipients from the transplant unit at Rigshospitalet, Copenhagen, Denmark.
Statistical Analysis
Data are presented as mean and standard deviation, median and range if continuous, or as frequencies if categorical. The number of patients with available data (n) was used in the calculation of summary statistics. Comparison was performed using the independent t-test, the Wilcoxon rank sum, or the chi-squared test as appropriate. The significance threshold was set at 0.05.
All analyses were performed using STATA statistical software (version 12.1; StataCorp, College Station, TX).
Results
A total of 48 patients completed the study. Fifty lung transplant recipients gave informed consent; one participant died and one withdrew consent. No patients declined participation. Demographic data and immunosuppressive treatment are presented in Table 2. No difference was seen with respect to age, gender, marital status, educational level, employment status, time since transplantation, and type of lung transplantation.
Baseline Demographics
LTX, lung transplantation; SD, standard deviation.
Adherence to Immunosuppressive Medication
A total of 71% of patients in the intervention group were adherent compared with 55% in the control group (p = 0.23) (Table 3).
Results of the BAASIS and TAQ questionnaires
BAASIS, Basel Assessment of Adherence with Immunosuppressive Medication Scales; TAQ, Transplant Adherence Questionnaire.
The most frequent aberration in the control group was timing that is, taking the drugs >2 h away from the prescribed time. This was reported by a significantly higher proportion of patients in the control group than in the intervention group (11 patients [46%] vs. 3 patients [13%], p = 0.012). Two patients in the intervention group (8%) reported that this happened more than once a week; nine patients in the control group (38%) reported the same (p = 0.017).
No difference in adherence according to BAASIS was seen between patients with time since transplant above median compared with patients with time since transplant below median (p = 0.12).
Five patients (21%) in the intervention group reported more serious deviations from the prescribed regimen, all stating that they had omitted a dose of immunosuppressive medication during the past 4 weeks, but only on a single occasion. Four patients in the control group (17%) reported the omission of a dose of immunosuppressive medication during the past 4 weeks. Three of these patients reported that the omission had only occurred once, but one patient reported skipping a dose four times. No so-called “drug holidays” were reported, that is, skipping several doses in a row. No patients reported to have taken less than the prescribed dose.
No patients in the intervention group failed more than one item. Seven patients (29%) in the control group failed in only one item. Four patients (17%) in the control group reported nonadherence in more than one of the four items of nonadherence.
Patients' Knowledge of Post-Transplant Care
Patients in the intervention group had a significantly higher number of correct answers to the author-constructed questionnaire on patients' knowledge of transplant-related topics compared with patients in the control group (median 11 vs. 10, p = 0.02).
A total of 88% of the patients in the intervention group found the e-learning program relevant and 71% wished to review the program annually as a reminder. A total of 25% reported that participating in the e-learning program had resulted in lifestyle changes. Among the patients, 63% would have liked to receive the e-learning program earlier and 88% believed that other lung transplant recipients would benefit from the e-learning program.
Discussion
Our study investigated the benefits of an e-learning program on knowledge of post-transplant care among lung transplant recipients. Assuming that more correct answers and better timing of immunosuppressive medicine in those who received the e-learning program compared with those who received standard education was not caused by bias or a chance finding, our study is the first to show that an e-learning program increases lung transplant recipients' knowledge of post-transplant care. Patients randomized to the e-learning program had significantly more correct answers and the majority of recipients found it relevant and wished to repeat it annually. Our results also suggest that the e-learning program might improve adherence compared with standard patient education provided at every follow-up visit. Thus, patients in the intervention group had better timing and failed in fewer items of nonadherence.
Nonadherence to the immunosuppressive drug regimen was high in our population, as 38% of the patients were nonadherent (29% in the intervention group and 45% in the control group). This is higher than previous reports of nonadherence where rates to the immunosuppressive medication adherence ranged from 13% to 37%. 2,5 We found no relationship between the time from transplantation and drug adherence, possibly due to the limited number of patients. We found some indications, although statistically nonsignificant, toward better adherence in the intervention group suggesting that a regular brush-up of patients' knowledge of post-transplant care can be ensured by a 15-min e-learning program. The lack of a statistical significance may be caused by a type two error. However, we found that the e-learning program resulted in improved adherence with regard to timing of the medication.
Nonadherence may be difficult to discover. The gold standard is the use of an electronic pill count that may provide a less biased estimate than self-reported questionnaires. 28 However, electronic pill counts are considered impractical and unrealistic in daily clinical use. 9 Several self-report instruments such as BAASIS and TAQ have been developed with the purpose of examining nonadherence. It has been suggested that self-report instruments, together with clinical judgement and blood sample analyses are key components for assessment of adherence in clinical practice. 2 In our study, we used the BAASIS and TAQ questionnaires and were able to show a trend for better adherence in the intervention group measured with BAASIS but no difference in TAQ. The BAASIS questionnaire measures adherence for a period of 4 weeks compared with 4 days in TAQ. Focusing on the previous 4 days only, probably results in less recall bias, but the longer time span assessed with BAASIS may provide a more truthful picture of patient behavior.
Computer-based education has been shown to be noninferior compared with conventional education. 19 e-Learning programs have resulted in increased patient knowledge in nontransplant patients, increased empowerment, and reporting of fewer symptoms. 21 Among health care personnel, a significantly higher adherence to alcohol-based hand rubbing has been demonstrated. 29 The advantages of e-learning are obvious as it is cost-effective compared with nurse-led conventional education. It also allows patients to go through the program at their own pace and to repeat it as needed. We did not include caregivers in the e-learning program although they may play a critical role in the education and support of transplant recipients. Involvement of caregivers may be advantageous and should be addressed in further studies.
In this study, we found a small, although statistically significant, difference between patients who used the e-learning program compared with those who followed the conventional education program. Our transplant recipients generally received the e-learning program well and they recommended it for an annual brush-up and as a part of the general education provided for all transplant recipients. Our e-learning program was developed by one of our transplant nurses (T.B.G.); it is short (15 min) and easily administered by e-mail to transplant recipients. Thus, it can easily be implemented at other transplant clinics.
Strengths and Limitations
The strength of the study is the randomized controlled design and the validation of the e-learning program by focus group interviews among patients and health professionals. However, there are several limitations to the study. It included a relatively small number of participants and only subjective self-reported data on adherence were used. Owing to the lack of a standardized validated questionnaire that measures patients' skills and knowledge of post-transplant care, a new questionnaire was developed for this study. This new questionnaire was only face validated. Self-reported measures can lead to bias that may be different between the intervention and the control group. Caregivers were not included in the study. Furthermore, self-reported adherence was not supported by objective measures, for instance, trough serum levels of immunosuppressive medication. Other parameters of interest are prevalence of chronic lung allograft dysfunction, hospitalization, renal function, quality of life, and survival.
Conclusions
A simple and patient-friendly 15-min e-learning program improves lung transplant recipients' skills and knowledge of post-transplant care. This study shows a tendency toward better adherence to immunosuppressive medication. E-Learning seems to be a valid and important supplement to standard education at every lung transplant follow-up visit. However, more research is warranted.
Footnotes
Authors' Contributions
T.B.G. and E.B. conceived the study idea and T.B.G. developed the e-learning program. T.B.G. collected the data. C.H. and O.H. performed the data analysis. E.B. organized the writing, and all authors critically revised the article for intellectual content and approved the final version before submission.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.