
Abstract
Background:
In the era of personalized medicine, there has been an increase in demand on cytopathology service to perform rapid onsite evaluation of touch imprints (ROSETIs) of needle core biopsies (NCBs) to ensure sample adequacy and provide preliminary diagnosis. Limited publications have addressed use of telecytopathology for ROSETIs. We present our experience with telecytopathology-guided ROSETIs of NCBs.
Materials and Methods:
Cytotechnologist onsite transmitted real-time images of Diff-QUIK stained touch imprints of NCBs using an Olympus digital camera through Ethernet to a pathologist. The preliminary diagnosis from telecytopathology-guided ROSETIs was compared with that of the final NCB for diagnostic accuracy. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated.
Results:
Of 186 cases, 163 (87%) were concordant and 23 (13%) were discordant. Of the 23 discordant cases, 14 (58%) were diagnosed as benign with final NCB diagnoses as malignant and 9 (41%) were suspicious on ROSETIs with final NCB diagnoses as benign. The causes of discordance among cases categorized as benign on preliminary and malignant on final included interpretative error (9) and sampling (6). Six cases categorized as suspicious on preliminary and negative on final biopsy diagnosis correlated with concurrent fine-needle aspiration, raising the possibility of loss of diagnostic areas in processed tissue cores. Remaining three cases in this category represented misinterpretation of reactive cells. Sensitivity, specificity, PPV, and NPV were 87.9%, 95.7%, 97.1%, and 82.7%, respectively.
Conclusions:
Telecytopathology-guided ROSETI yields high accuracy for preliminary interpretation of NCBs and may be utilized as an effective substitute for conventional microscopy.
Introduction
Fine-needle aspiration (FNA) biopsy of various body sites is a well-established safe technique for diagnosing a variety of benign and malignant lesions. 1 In recent years, there has been a surge in the needle core biopsies (NCBs) despite the comparable diagnostic yield and minimally invasive nature of FNA. 2 The preference for NCBs over FNA is attributable to better yield of tissue with the former that allows for ancillary studies such as immunohistochemistry, flow cytometry, and molecular studies that are critical for patient selection for targeted therapy. 3,4
The increase in volume in NCBs has also resulted in increased utilization of cytopathology service for rapid onsite evaluation of touch imprints (ROSETIs) of NCBs. This has resulted in an increased demand on pathologists at several institutions who play an important role in ROSETIs of NCBs to ensure adequate collection of specimens and render preliminary diagnosis. However, NCBs are time consuming and can occur simultaneously in different locations in the hospital campus, making it impossible for a single pathologist to cover these procedures. In addition, the wait time for a pathologist between different passes is not reimbursable and takes away significant time from reimbursable activities (e.g., sign out of cases, administrative responsibilities, academic activities, and teaching).
Dynamic telecytology is a cost- and time-effective approach allowing for cytotechnologists, senior residents, or cytology fellows onsite to prepare the slides and transmit live images using telecytology to the pathologists in the laboratory/office. 5 –8 The operator onsite is able to review the whole slide with the attending pathologist, thereby obviating the need for the pathologist to physically go to the site and perform rapid onsite evaluation (ROSE). It also allows the pathologist to do ROSE assessment at multiple sites simultaneously. Although telecytopathology is a well-documented procedure that is being increasingly used for ROSE of FNAs from various body sites in many sites, it has been underutilized for ROSETIs of NCBs. 8 –17 Recent College of American Pathologists survey revealed that pathologists rarely used telecytopathology (1.5%) for ROSETIs of NCBs. 18 This study reviews our experience using dynamic telecytology for ROSETIs of NCBs.
Materials and Methods
A retrospective analysis of all Diff-Quik (Mercedes Medical, Sarasota, FL) stained slides, prepared onsite for telecytopathology-guided ROSETIs of NCBs, was performed between January 2017 and April 2018. The touch imprints (TIs) were prepared by gently removing the NCBs from the biopsy needle and dragging it onto a glass slide. Telecytopathology-guided ROSETI was categorized into the following groups of diagnoses: benign, suspicious, and malignant. Telecytopathology-guided ROSETI diagnosis was compared with that of the final NCB diagnosis. Cases were considered concordant if the final NCB diagnosis was the same as the telecytopathology-guided ROSETI diagnosis, or if the final NCB diagnostic category was malignant when the telecytopathology-guided ROSETI diagnosis was suspicious. A diagnosis upgrade was given to cases that were considered benign on telecytopathology-guided ROSETI but received final NCB diagnosis of malignant. Conversely, a diagnosis downgrade was given to cases that were considered suspicious or malignant on telecytopathology-guided ROSETI but received final NCB diagnosis of benign. In all discordant cases wherein a telecytopathology-guided ROSETI diagnosis was malignant or suspicious and concurrent NCBs did not reveal any malignant cells, any cytologic or surgical tissue biopsy follow-up was also reviewed. Sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) for telecytology-guided ROSETI diagnoses were calculated using final NCB diagnosis or any concurrent FNA or subsequent tissue biopsy follow-up in a few discordant cases as gold standard.
Prior publications provide a detailed explanation of the telecytopathology system used in this study. 10,12,13,15,17 Concisely, the telecytopathology system (Fig. 1) comprised an Olympus (Olympus America, Center Valley, PA) CX41 microscope and a digital camera with NetCam software (Olympus). The cytotechnologist at the radiology suites prepared slides onsite and transmitted live video images through internet to the cytopathologist's desktop at a remote site. The interaction between cytopathologists and the cytotechnologists was established using a hand-free Vocera (San Jose, CA) voice communication system. Preliminary diagnosis was provided to the radiologist after the performance of telecytopathology-guided ROSETIs. Recommendations for collection of additional material for ancillary studies were made as considered necessary. The study was exempted from institutional board review.
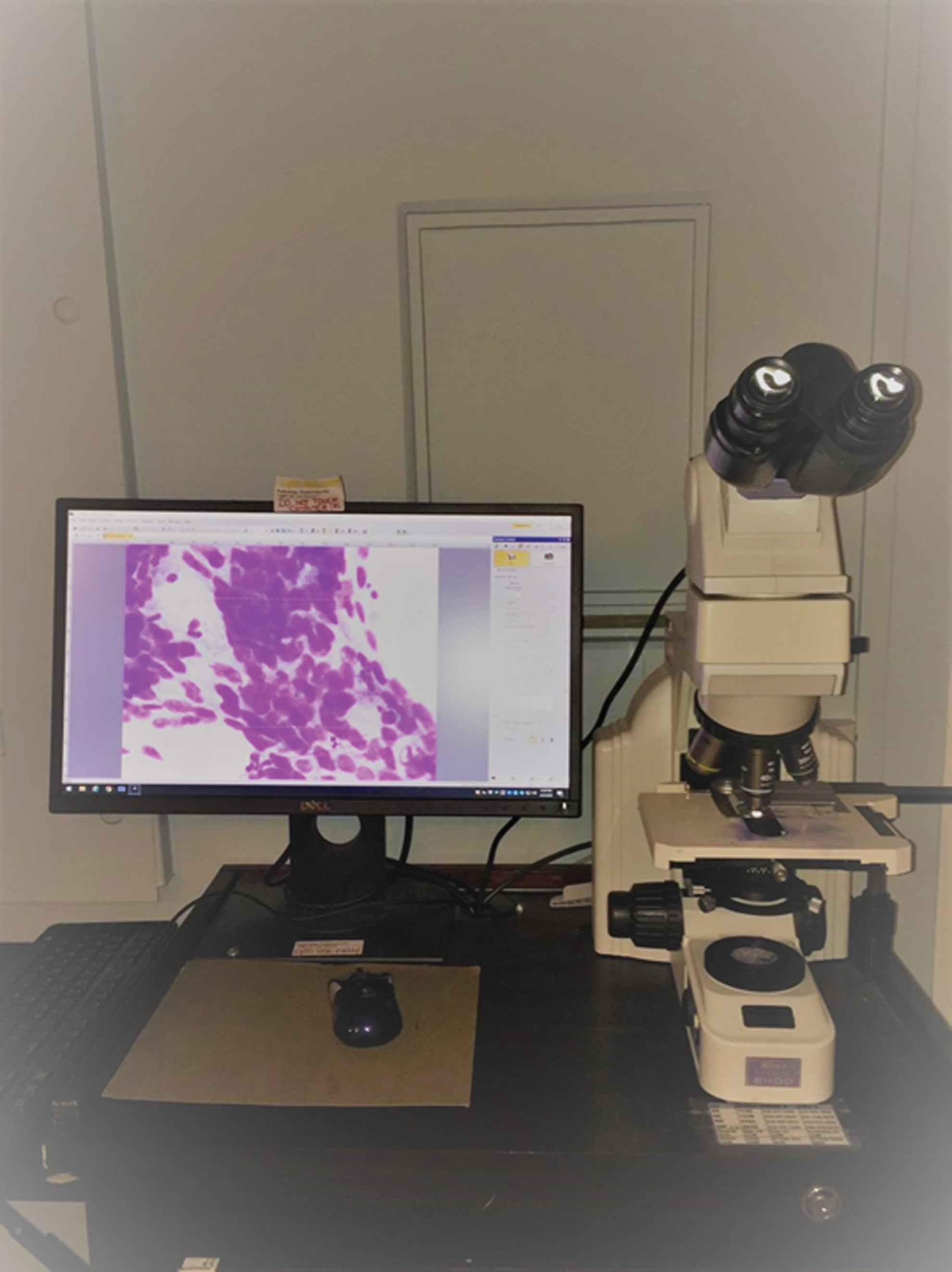
Telecytopathology system comprising microscope and monitor showing image of sheet of malignant tumor cells on TI. Color images are available online.
Results
Telecytopathology-guided ROSETI was performed on 186 NCBs obtained in radiology suites. Table 1 gives the follow-up NCB diagnosis on all telecytopathology-guided ROSETIs. All 52 cases with telecytopathology-guided ROSETI diagnoses of malignant correlated with NCB diagnoses of malignant. Of the 81 cases with telecytopathology-guided ROSETI benign diagnoses, 67 correlated with benign NCB diagnoses and remaining 14 cases received a malignant NCB diagnoses. Forty-two of the 53 cases with telecytopathology-guided ROSETI suspicious diagnoses correlated with malignant NCB diagnoses in 42 cases. Two cases corresponded with suspicious NCB diagnoses and the remaining nine cases received a benign NCB diagnoses. In summary, the final cytology diagnosis after using telecytopathology yielded a high concordance or accuracy rate of 88% (163/186). The upgraded and downgraded diagnosis rates were 7.5% (n = 14) and 4.8% (n = 9), respectively.
Follow-Up Final Needle Core Biopsy Diagnosis on All Telecytopathology-Guided Rapid Onsite Evaluation of Touch Imprints
NCBs, needle core biopsies; ROSETI, rapid onsite evaluation of touch imprint.
Figure 2 shows a flow chart with detailed analysis of 23 discordant cases. Of the 14 cases with telecytopathology-guided ROSETI diagnoses of benign and final NCB diagnoses of malignant, 9 were interpretive cytologic errors and 5 represented cases wherein malignant cells were identified only on NCBs and not on TIs. Of the nine cases with telecytopathology-guided ROSETI diagnosis of suspicious and final NCB diagnoses of benign, cytologic interpretative error was noted in three cases. In the remaining six cases, loss of diagnostic material was noted on NCBs. However, the follow-up concurrent FNA biopsy diagnoses in these six cases were malignant and correlated with the original telecytopathology-guided ROSETIs. The upgraded diagnosis rate was 7.5% (n = 14). The downgraded diagnosis rate was 0.02% (n = 3).
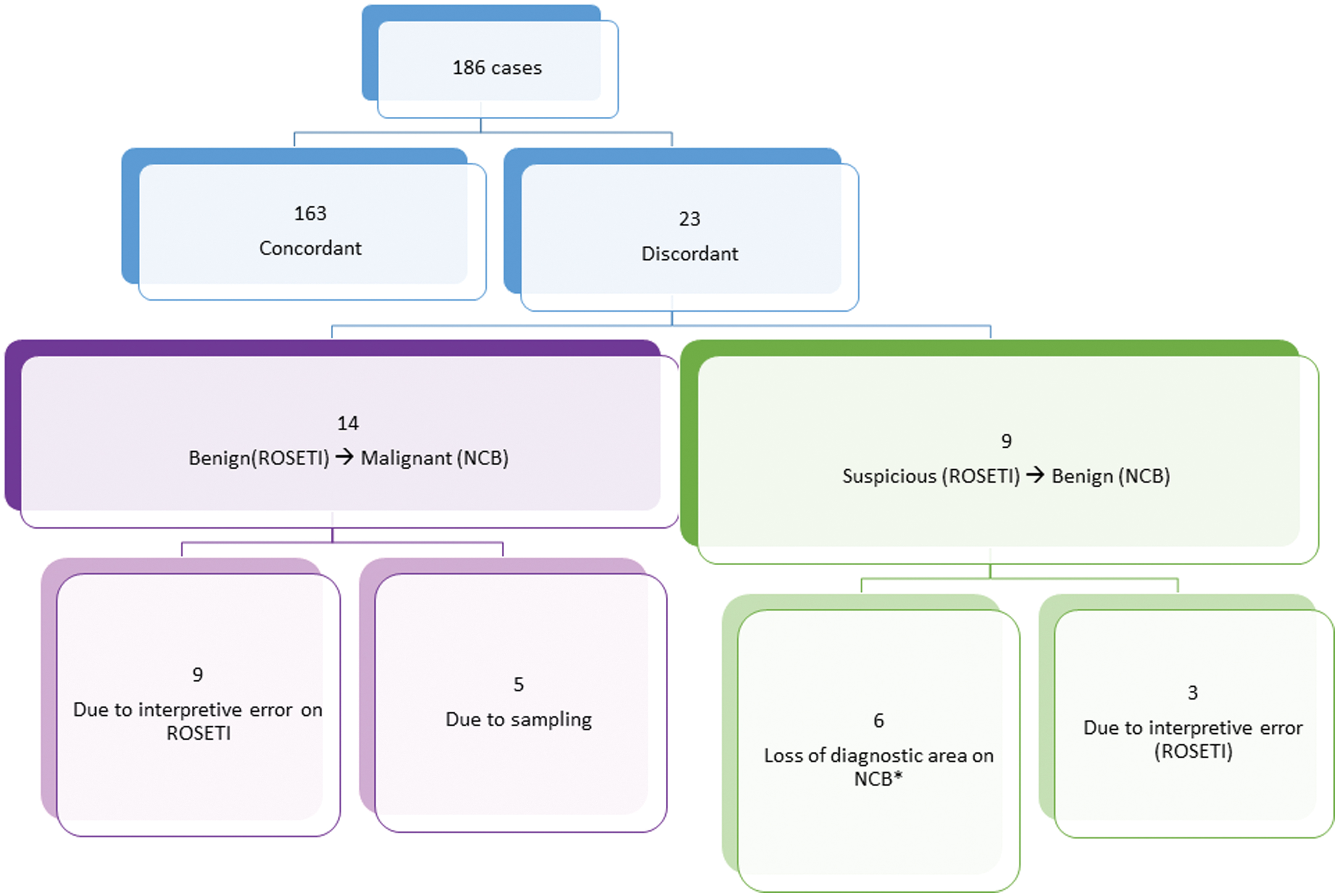
Flow chart of telecytopathology-guided rapid onsite evaluation of TI cases and their concordance with NCB diagnosis. A detailed analysis of 23 discordant cases is also shown. NCB, needle core biopsy; TI, touch imprint. Color images are available online.
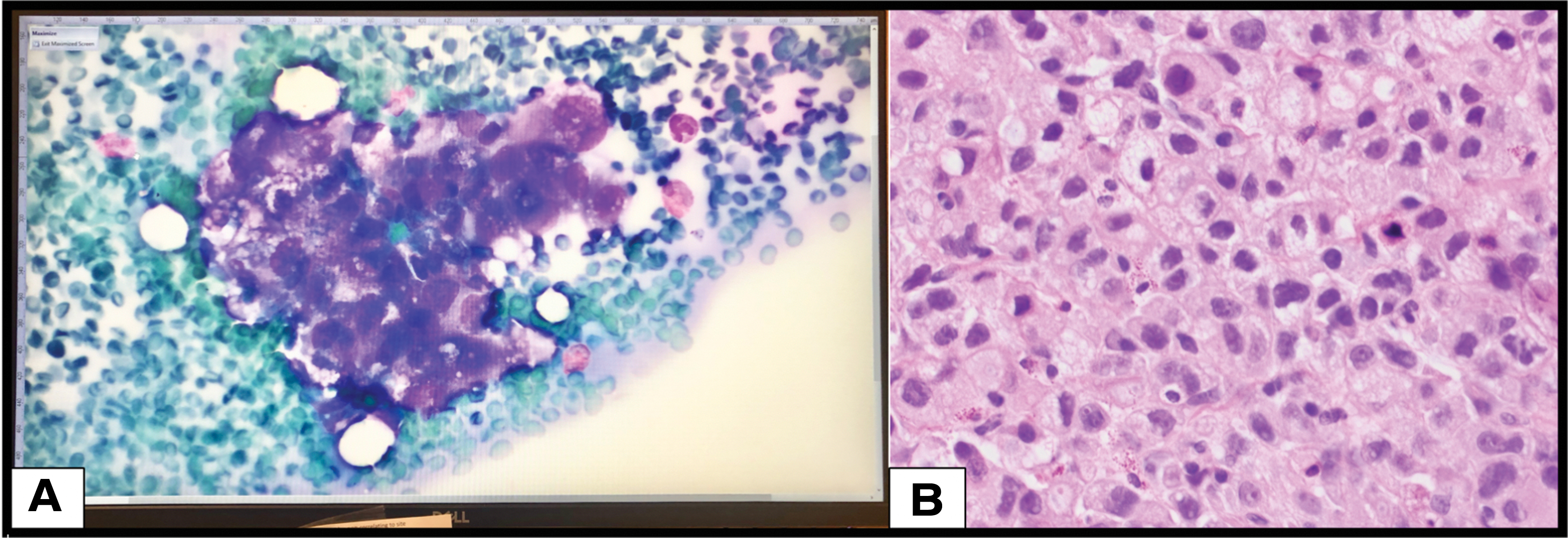
A detailed analysis of cytologic interpretive errors in 12 cases is provided in Table 2. Of the nine cases that were upgraded from benign to malignant on final NCB, tumor cells with foamy cytoplasm were interpreted as histocytes (two cases) (Fig. 3), metastatic adenocarcinoma was interpreted as benign reactive ductal cells (two cases) or reactive bronchial cells (one case), and squamous cell carcinoma was interpreted as metaplastic squamous epithelium (one case). TI cytology in two additional cases was misinterpreted as lymphocytes in a case of neuroendocrine tumor and rare atypical cell was overlooked in a case of adenocarcinoma. Lastly, chondroid material obscured by ultrasound gel on TI cytology was not recognized in a case of scapular chondrosarcoma. Review of three cases that were downgraded from suspicious on telecytopathology-guided ROSETIs to benign on final NCB diagnosis represented interpretive errors on ROSETIs where reactive pneumocytes were mistaken for suspicious tumor cells (two cases) and reactive fibroblasts were misinterpreted as spindle cell neoplasm (one case) (Fig. 4).

List of Cases with Explanation of Cytologic Interpretive Errors on Touch Imprints Resulting in Discordant Diagnosis Between the Telecytopathology-Guided Rapid Onsite Evaluation of Touch Imprints and Needle Core Biopsy
Sensitivity, specificity, PPV, and NPV for telecytology-assisted TIs were 87.9%, 95.7%, 97.1%, and 82.7%, respectively.
Discussion
Dynamic telecytology is widely used for ROSE of FNAs. However, its utilization for ROSETIs of NCBs remains low. At our institution, in addition to assessment and adequacy of telecytopathology-guided ROSETIs of NCBs, rendering a preliminary cytologic diagnosis by cytopathologist is part of our standard ROSE workflow. Our results support the utility of dynamic telecytology for ROSETIs of NCBs. Our diagnostic concordance rate of 88% using telecytology for ROSETIs and NCBs is within the reported range of 88% to 91% for ROSETIs using conventional microscopy requiring presence of pathologist onsite. 19 –21 To the best of our knowledge, this is the first study that has exclusively focused on diagnostic accuracy of dynamic telecytology-guided ROSETIs of NCBs. Lin et al. compared the preliminary adequacy assessment of telecytology-assisted TI with the adequate yield of NCBs for final diagnosis and found a concordance rate of 94.3%. 22 However, they did not render any preliminary cytologic diagnosis. Use of telecytopathology has obviated the need for pathologists to be physically present at the procedure site for ROSETIs and allowed support of multiple sites for ROSETIs at our institution.
In our study, dynamic telecytopathology-assisted ROSETI cytology on NCBs yielded sensitivity, specificity, PPV, and NPV of 87.9%, 95.7%, 97.1%, and 82.7%, respectively. Kubik et al. reported a higher sensitivity (94%) and a similar NPV (83%) using conventional microscopy that required presence of cytopathologist onsite. 23 In contrast to our study, their specificity (41%) and NPV (70%) were lower. In our series, we found that either TIs or NCBs may lack diagnostic cells in 7.52% of cases. Tong et al. demonstrated similar findings in 4.3% of their cases. 21
The upgraded diagnostic rate in our study was 7.5%. In five of our cases, malignant cells were present on NCBs and absent in TI cytology smears. We believe that absence of cells in TI smears is most likely related to increased tumor fibrosis, resulting in poor yield of cells on TI smears. Tong et al. made a similar inference in their study. 21 In addition, they also showed NCBs from bone and soft tissue were usually more cellular than TI. Three of our cases were biopsies of bone and soft tissue lesion. Remaining two cases were transbronchial lung NCBs that showed a small focus of adenocarcinoma. TI of these cases only showed benign bronchial cells and lacked tumor cells. As has been previously reported, small foci of tumor cells may not be sampled in TI cytology, giving a false negative diagnosis. 24 Core roll preparation where an NCB is simply rolled over the slide instead of just touching the slide may provide better sampling of the surface area, although small foci of tumor located deep within the tissue core may get missed by this method too. 25
In the remaining nine cases, interpretative errors that were identified represent diagnostic dilemmas often encountered in cytology practice. Review of such cases is always a useful learning exercise that helps improve diagnostic skills. These included misinterpretation of tumor cells as histiocytes (three cases), neuroendocrine tumor as lymphocytes (one case), adenocarcinoma of lung as reactive bronchial cells (one case), adenocarcinoma of pancreas as reactive ductal cells (two cases), squamous cell carcinoma as metaplastic squamous cells (one case), and obscuring ultrasound gel resulting in lack of recognition of chondroid material in a chondrosarcoma.
Of the nine cases that were considered suspicious on telecytopathology-guided ROSETIs, NCBs received a benign diagnosis in all nine cases. However, six of these cases on a subsequent FNA biopsy showed malignant cells. Our finding of 5.7% (6 out of 107) of malignant cases lacking tumor in NCB is comparable with 8.2% cases reported in a prior study using conventional microscopy for onsite slide evaluations. 26 As suggested by Moghadamfalahi et al., we believe tumor exhaustion in tissue core biopsy as a result of TI cytology is a pitfall of the procedure and gentle touch of core biopsy in most instances should prevent this. 26 In the remaining three cases, benign cells on ROSETIs were misinterpreted as malignant as has also been reported by Lin et al. 22 In two cases, reactive pneumocytes were mistaken for suspicious tumor cells, and in another case, reactive fibroblast was interpreted as suspicious for spindle cell neoplasm.
Onsite evaluation of TIs of NCBs by a pathologist using conventional microscopy has proven to assist in diagnosing the lesions with increased accuracy. 20 –25 However, with surge in volume of NCBs to procure tissue for ancillary testing has also placed an increased demand on cytopathologist for ROSE of core biopsies. NCB is a time-consuming procedure. Distance of the pathology laboratory from the procedure sites, time constraints, and poor reimbursement are some of the challenges that cytopathology laboratories are facing. Although telecytopathology has been widely accepted for ROSE of FNA cytology, a recent survey showed that it is being rarely used for ROSETIs of NCBs.
In our study, we have shown that dynamic telecytopathology-guided ROSETIs of NCBs yield high accuracy of preliminary diagnosis that is comparable with that of studies that have used presence of onsite cytopathologist for performing ROSETIs of NCBs using conventional microscopy. Traditionally, an onsite cytopathologist performing ROSETIs assists with the triage of NCBs for ancillary studies (e.g., flow cytometry, molecular studies, and cytogenetic analysis). Cytopathologist using dynamic telecytopathology could perform similar tasks remotely and work more efficiently. Monaco et al. showed that telecytopathology implementation decreased cytopathologist's work time per ROSE case from an average of 20.95 to 2.91 min per case (86% time savings). 27 Using dynamic telecytopathology and working remotely eliminate the travel time to distant sites and waiting time between evaluations of repeat core biopsy from same site or multiple sites on the same patient, thereby allowing the pathologist to utilize his or her time more judiciously in patient care, administrative, and educational activities.
Properly trained cytotechnologists, cytopathology fellows, or senior residents who attend the onsite NCB procedures and transmit real-time images and show significant findings during interaction with cytopathologist through vocera or phone are vital to the success of telecytopathology-assisted ROSETIs as have also been emphasized in other studies on dynamic telecytopathology-assisted ROSE of FNAs. 8,9 –17 In addition, it is essential that pathologists are familiarized with dynamic telecytopathology-assisted interpretation of real-time images. Telecytopathology system was introduced at our hospital in November 2009. Since we performed an internal validation testing protocol, at that time, on cytology aspirate smears similar to that described by McCarthy et al. before its use in a routine practice, we did not find it necessary to do a separate validation protocol for this study. 28
In conclusion, we have demonstrated that dynamic telecytopathology-guided ROSETI of NCB has a diagnostic accuracy that is comparable with ROSETI with conventional microscopy requiring presence of cytopathologists onsite. Implementation of telecytopathology-guided ROSETIs of NCBs in daily practice is an innovative way for augmenting the cytopathologists' efficiency, meeting the demands of increase involume and delivering optimal patient care without compromising the outcome.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this project.