
Abstract
Objective:
During the current coronavirus disease 2019 (COVID-19) pandemic, telemedicine has been brought to the forefront of attention. This report aimed to assess psychiatric comorbidities in COVID-19 patients by utilizing telepsychiatry.
Methods:
COVID-19 patients admitted in Fasa University Hospital and nonhospitalized outpatients of Fasa city were interviewed by a psychiatrist through video chat for a 1-month period (March–April, 2020). Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder Assessment (GAD-7), and Perceived Stress Scale-14 (PSS 14) questionnaires were administered for all patients. Each patient's mental status was recorded, and if any psychiatric problem was diagnosed, supportive psychotherapy, pharmacotherapy, and follow-up visits based on the patient's condition were started.
Result:
From a total of 82 COVID-19 patients who entered the study, 32 (39.03%) and 50 (60.97%) subjects were inpatients and outpatients, respectively. Moreover, 32 (39.03%) subjects were male and 50 (60.97%) were female. Insomnia seen in 24 (29.3%) patients and adjustment disorder in 13 (15.9%) patients were the most common psychiatric disorders among a total of 33 (40.2%) patients suffering from mental illness. Female and hospitalized patients presented significantly more frequent comorbidities than males and outpatients.
Conclusions:
Psychiatric disorders were significantly more common in patients with hospital admission than those without and more frequent in female versus male subjects. There were no significant differences between male and female subjects with and without admission according to the PHQ-9, GAD-7, and PSS-14 scores. It was concluded that telepsychiatry in the early stages of mental problems during a catastrophic event like the coronavirus pandemic, can be an efficient instrument for the screening of psychosomatic comorbidities, so that pharmacological treatment (considering possible drug interactions with COVID-19 medications) and psychotherapeutic intervention can be optimized by psychiatrists.
Introduction
Telepsychiatry is a known method for the psychiatric interview, assessment, diagnosis, and, if necessary, pharmacological and psychological management of patients experiencing difficulties with in-person visits. Although it is not a new technology, telemedicine can be used more efficiently today due to the accessibility to high-speed internet and availability of user-friendly devices and applications. 1 In the recent pandemic of coronavirus disease 2019 (COVID-19), the use of telepsychiatry was valuable because of the psychological complications of the disease imposed on patients, medical staff, and the quarantined general population. 2,3
Considering the psychiatric issues that emerged in COVID-19 patients, it was recommended that they be visited by a psychiatrist because of the similarity between psychiatric comorbidities and some complications of COVID-19 diseases (changes in appetite and sleep pattern, loss of energy, etc.). A psychiatrist can more accurately evaluate whether the origin of these symptoms is a disease complication or a psychiatric comorbidity. Moreover, a psychiatrist can better treat patients' psychological problems with psycho/pharmacotherapy. The possibility of interactions between psychotropic medications and many of the drugs used to treat COVID-19 is another important issue that can optimally be considered by a psychiatrist. 4
The shortage of personal protective equipment for staff, lack of trained personnel in the field of psychiatric nursing, and the overwhelming number of admissions of COVID-19 are some reasons to use telepsychiatry. 5 A real concern regarding in-person psychiatric interviews with patients is that they are believed to be essential for better psychiatric care; thus, the implementation of video chat is highly recommended. 6 Epidemiologic assessments of the prevalence of psychosomatic problems in COVID-19 patients can be achieved using this technology. The current telepsychiatry study purposed to report on the prevalence of psychiatric comorbidities in COVID-19 patients and evaluate their needs for further psychiatric support.
Methods
Population
In this cross-sectional study, all COVID-19 patients in Fasa city from March 18 to April 17, 2020, were diagnosed by real-time polymerase chain reaction for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Critically ill patients (those intubated or deceased), children <10 years of age, and patients who expressed an unwillingness to participate in the survey were excluded (Fig. 1). The study was approved by the local and national ethics committee (IR.FUMS.REC.1398.200).
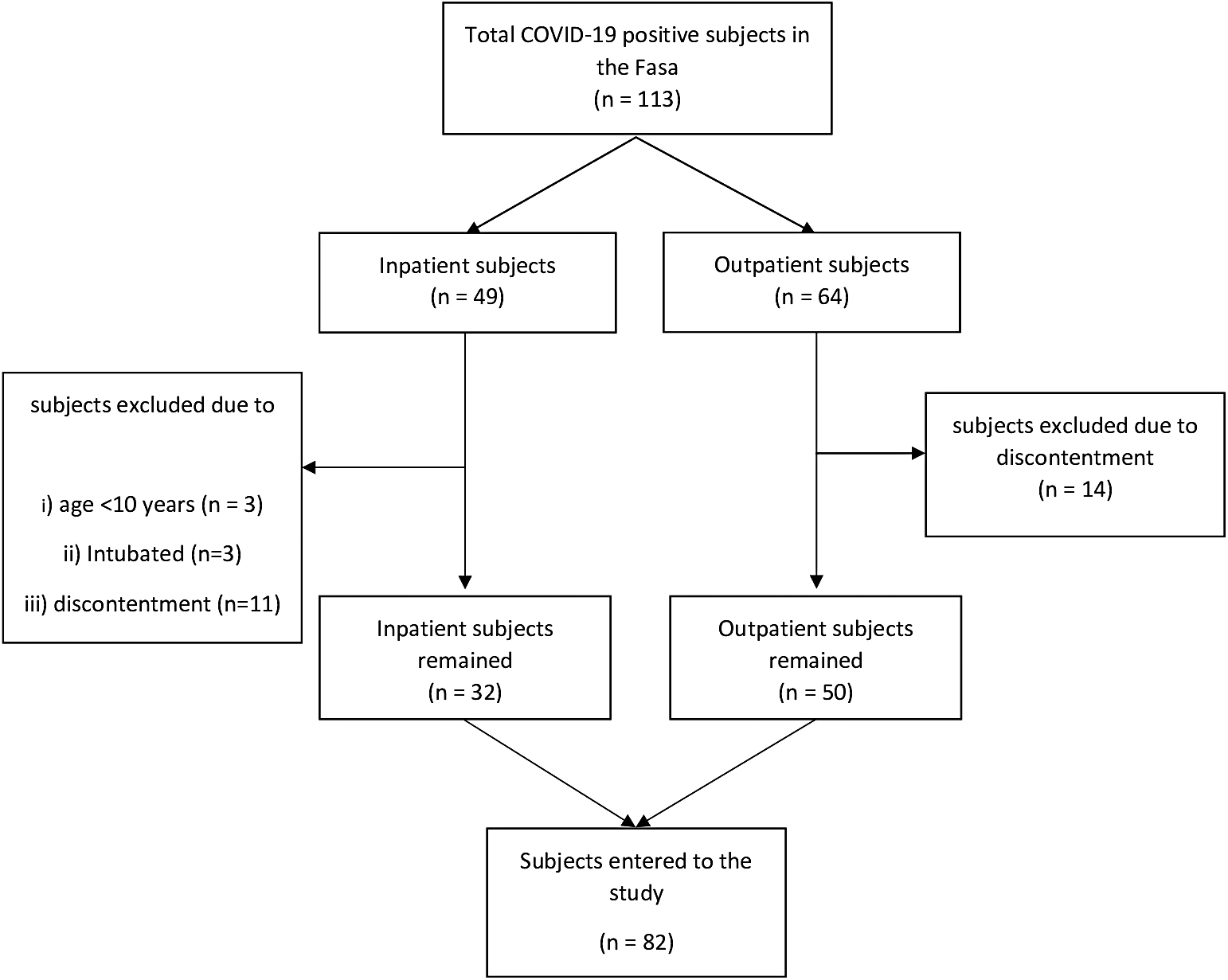
Flowchart of participants. COVID-19, coronavirus disease 2019.
Psychiatric Interview
A semistructured psychiatric interview (identifying data, current mental status, psychiatric history, family history, and medical history) was conducted by video chat with COVID-19 patients admitted to Fasa University Hospital and with affected patients with mild symptoms quarantined at home by psychiatrists using a tablet for hospitalized patients and personal cell phones for outpatient cases.
Three psychiatric questionnaires (reliable and validated in Persian), 7 –9 the Patient Health Questionnaire (PHQ-9 score >5 for depression), 10 Generalized Anxiety Disorder Assessment (GAD-7 > 5 for general anxiety disorder), 11 and Perceived Stress Scale-14 (PSS-14 higher scores predicts more perceived stress), were administered. 12
Follow-ups
If any psychiatric problem was detected, daily psychiatric follow-up and a brief period of supportive psychotherapy were implemented to reduce patient symptoms and improve patients' coping skills. The techniques used included empathy, reassurance, normalizing and destigmatizing, and enhancing adaptive skills, and medication was initiated if needed. 13 For all subjects, 1 and 6-month follow-ups were planned, and for subjects with diagnosed psychiatric problems, closer follow-ups were arranged based upon their needs. For outpatient subjects, an electronic prescription was administered and close follow-ups were scheduled if needed. Patients were allowed to call the psychiatrist whenever they needed help. The follow-up data will be published in the future by longitudinal design.
Statistical Analysis
Data are presented as mean ± standard deviation and number (percent). For comparisons between categorical groups, the chi-square test was performed, and for continuous variables, the independent sample t test was used to compare subjects. Logistic regression was used to calculate the odds ratios (ORs) and 95% confidence intervals (CIs). All statistical analyses were performed in SPSS® 22.0 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.), and a p-value <0.05 was considered as statistically significant.
Results
From a total of 82 COVID-19 patients who entered the study, 32 (39.03%) subjects were inpatients and 50 (60.97%) subjects were outpatients; 32 (39.03%) subjects were male and 50 (60.97%) subjects were female. Patients in this survey ranged from 17 to 80 years of age. The mean age of the hospitalized patients was 40.34 ± 14.39 years and that for nonhospitalized patients was 43.62 ± 15.81 years.
Totally, 33 patients (40.2%) suffered from psychiatric illness; 13 patients had adjustment disorder (15.9%), 24 patients had insomnia (29.3%), 3 patients had major depressive disorder (3.7%), and 5 patients had GAD (6.1%). Among these patients, 13 (15.9%) had two psychiatric illnesses at once. Moreover, 17 (20.7%) patients had a history of psychiatric illness and 4 of them consumed psychiatric medications before admission, at which time any necessary dose adjustment was done. Sessions of supportive psychotherapy were conducted for 33 patients, based on the severity of their psychiatric problem, and psychotropic medication was started for 5 (15.15%) patients. These cases are currently under close telepsychiatric follow-up.
After categorizing subjects into two groups, namely those with and those without hospital admission, it was observed that the frequency of mental illness in those with hospital admission (n = 18; 60%) was much higher than in those without hospital admission (n = 15; 28.8%). Nine patients (17.30%) in the nonhospitalized patients compared with eight patients (26.66%) in the hospitalized group had a history of psychiatric disorders. Table 1 presents the results regarding current and past psychiatry disorders according to gender and admission status. There were significant differences between frequencies of the total psychiatry disorders, insomnia, and adjustment disorder between genders and admission status. A significant difference between males and females (p-value = 0.042) was also seen in cases with past psychiatric disorders.
Comparison of Current and Past Psychiatry Disorders According to Gender and Admission Status
Significant p values are shown in bold.
GAD, general anxiety disorder; MDD, major depressive disorder.
In total, 31 (37.3) patients had a PHQ score >5 and 24 (28.9) patients had a GAD score >5. The mean PSS score was 10.74 ± 8.39 in the total population. Table 2 presents the frequencies of subjects with PHQ >5 and GAD >5 and the mean PSS score according to gender and admission status. There were no significant differences between groups in the results of the three previously mentioned questionnaires.
Comparison of PHQ-9, GAD-7, and PSS-14 Scores According to Gender and Admission Status
GAD-7, Generalized Anxiety Disorder Assessment; PHQ-9, Patient Health Questionnaire; PSS-14, Perceived Stress Scale-14.
Table 3 presents the OR (95% CI) of having a current psychiatry disorder and a past psychiatry disorder in the four groups according to gender and admission status. There were just two significant ORs in having a current psychiatry disorder, which were related to females with hospital admission and males without it. Although the OR of males with admission was higher than the reference group, the difference was not statistically significant.
Age-Adjusted Associations of Current Psychiatry Disorder and Past Psychiatry Disorder According to Gender and Admission Status
Significant p values are shown in bold.
CI, confidence interval; OR, odds ratio.
Discussion
The main findings of this study were (1) >40% of subjects had current psychiatric issues; insomnia with a frequency of 29.3% and adjustment disorders with a frequency ∼16% were ranked first and second, respectively; (2) females had significantly higher frequencies in current/past psychiatry problems. Among psychiatric disorders, insomnia and adjustment disorders had significant differences between males and females; (3) psychiatric disorders were more common in patients with (60%) than in those without (28.8%) hospital admission. Just as with the differences between genders, insomnia and adjustment disorders were observed to be two significant variables that differed between the two groups of admission status; (4) there were no significant differences between males and females or subjects with and without admission based on PHQ-9, GAD-7, and PSS-14 scores. Also, it seems that GAD-7 underestimated the prevalence of GAD based on differences between the psychiatrist assessment in this study and the GAD-7 score; (5) it seems that admission can increase the chance of having psychiatric disorders in both genders but significantly more in females. Male patients without a hospital admission had a significantly lower association with psychiatric disorders than females without admission.
In a general population of >72,000 Iranian adults, prevalence rates of psychiatric disorders were reported as 31.03% and 25.42% diagnosed using a screening tool and through clinical assessment, respectively. 14 In this study, however, the prevalence of psychiatric problems in COVID-19 patients was found to be ∼40% using both assessment methods. It seems that the frequency of psychiatric problems may be higher in COVID-19 patients than in the normal population.
Importantly, in the early stages of mental problems during a catastrophic event like the corona pandemic, telepsychiatry can be an efficient instrument for providing psychotherapeutic intervention. To the best of the authors' knowledge, there is little data regarding the prevalence of different psychiatric comorbidities in COVID-19 patients during pandemics. Moreover, the few published studies have focused on clinically stable patients with online surveys. 15
Some signs and symptoms of patients with a physical illness, like a viral infection, can be similar to some of the DSM criteria for depression or anxiety. Inventories of psychiatric evaluation, however, ask some questions that can be commonly answered during a physical illness like COVID-19. Therefore, only a psychiatrist can distinguish the etiology of such complaints. Furthermore, the outcome of psychiatric comorbidities would be improved by accurate and early diagnosis of the origin of symptoms. 16 Importantly, cytochrome drug interactions between psychotropic medications and antiviral agents and drugs currently used in treating COVID-19 are a matter of concern that can be considered by a psychiatrist. 4
In this study, the existence of psychiatric comorbidities is briefly reported, although the data are among the most novel findings since the emergence of the COVID-19 pandemic. Although this study found psychiatric problems to be more frequent in women and hospitalized COVID-19 patients, it cannot be concluded that COVID-19 is a predisposing factor for mental illness or that mental illness can worsen the prognosis of COVID-19.
This study has some limitations, including its low sample size and single city data, considering the worldwide pandemic of COVID-19 and the mild disease course in a great majority of patients. This study is currently being continued and will be updated in the future with longitudinal data.
In conclusion, all COVID-19 patients need to be visited by a psychiatrist, because patients might have a history of psychiatric illness that can be exacerbated by an infectious disease. Moreover, patients are very likely to encounter psychiatric symptoms during the stressful period of viral respiratory disease.
Footnotes
Acknowledgments
The authors acknowledge the efforts of the personnel of the Vali-Asr Hospital who were involved in managing and helping the COVID-19 patients.
Statement of Ethics
In this study, the patients have given their written informed consent and that the study protocol was approved by the regional and national research ethics committees (the equivalent of institutional review boards) of FUMS, (reference no. IR.FUMS.REC.1398.200).
Authors' Contributions
The study was conceptualized by B.F., A.Z., and M.F.; the study methodology was by K.H. and B.F.; software was performed by M.H.Y.; the study validation was by K.H. and M.H.Y.; formal analysis was carried out by M.H.Y.; investigation was performed by A.Z. and B.F.; resources of the study was taken care of B.F. and A.Z.; data curation was done by B.F. and K.H.; original draft was prepared by B.F. and M.F.; review and editing of the article were by A.Z. and K.H.; visualization was done by M.H.Y and M.F.; and B.F. supervised the study and was involved in project administration.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors did not receive any specific funding for this article.