
Abstract
Background:
Coronavirus disease 2019 (COVID-19) has led to a national health care emergency in the United States and exposed resource shortages, particularly of health care providers trained to provide critical or intensive care. This article describes how digital health technologies are being or could be used for COVID-19 mitigation. It then proposes the National Emergency Tele-Critical Care Network (NETCCN), which would combine digital health technologies to address this and future crises.
Methods:
Subject matter experts from the Society of Critical Care Medicine and the Telemedicine and Advanced Technology Research Center examined the peer-reviewed literature and science/technology news to see what digital health technologies have already been or could be implemented to (1) support patients while limiting COVID-19 transmission, (2) increase health care providers' capability and capacity, and (3) predict/prevent future outbreaks.
Results:
Major technologies identified included telemedicine and mobile care (for COVID-19 as well as routine care), tiered telementoring, telecritical care, robotics, and artificial intelligence for monitoring. Several of these could be assimilated to form an interoperable scalable NETCCN. NETCCN would assist health care providers, wherever they are located, by obtaining real-time patient and supplies data and disseminating critical care expertise. NETCCN capabilities should be maintained between disasters and regularly tested to ensure continual readiness.
Conclusions:
COVID-19 has demonstrated the impact of a large-scale health emergency on the existing infrastructures. Short term, an approach to meeting this challenge is to adopt existing digital health technologies. Long term, developing a NETCCN may ensure that the necessary ecosystem is available to respond to future emergencies.
Introduction
Major disasters and health care emergencies have previously exposed gaps in health care systems at local, regional, and national levels. 1 –3 The spread of the current coronavirus disease 2019 (COVID-19) has led to a national health care emergency in the United States and focused attention on multiple resource limitations. 4 Given its potential to cause acute respiratory and organ failure, a substantial number of COVID-19 patients will require hospitalization (28%) and critical care (6%). 5 However, more than half of all counties in the U.S. do not have intensive care beds. 6 Current forecasts suggest that even large metropolitan areas are likely to see demand for critical care services exceed supply. 4 Although some physical resources (beds, ventilators, personal protective equipment, etc.) can be manufactured rapidly, 7 preparation and training of skilled clinicians who can provide critical care (critical care nurses, intensivist physicians, respiratory therapists, etc.) take time. Health care providers are also at increased risk of contracting COVID-19, further reducing the pool of skilled clinicians. When health care resources are strained to the breaking point, patient care may be compromised, which is associated with increased mortality rates. 8,9
The current pandemic provides opportunities to expand and integrate digital health technologies across the U.S. health care system so that on-demand medical resources can be efficiently applied to the correct location at the correct time. Likewise, the U.S. military has expanded telemedicine support to austere medicine and disaster response using low cost mobile health technologies. 10 Digital health tools include, but are not limited to, telemedicine/telehealth, electronic health records, public health surveillance using “big data” and artificial intelligence (AI) algorithms, wireless health sensors, imaging, mobile health, and health analytics for clinical decision making.
This article initially reviews the literature and describes available digital health tools used for COVID-19–related care that augment critical care as well as maintain routine and specialty care services. Health care systems and clinics could feasibly adopt several of these tools rapidly. However, the near and distant future requires a cohesive model that incorporates multiple technologies to solve the problem of critical provider shortages. This article then outlines a model—the National Emergency Tele-Critical Care Network (NETCCN)—that allows a rapid, flexible, and expansive response that can scale quickly in times of disaster. Further research efforts are then outlined to make the model a reality.
Current Digital Health Tools
Owing to the rapidly changing scenario with COVID-19 and digital health adaptations to address it, our subject matter experts from the Society of Critical Care Medicine (SCCM) and the Telemedicine and Advanced Technology Research Center (TATRC) examined the science/technology news as well as the peer-reviewed literature to explore digital health technologies that have already been or could be implemented. Several of the technologies have been shown to be efficacious for other health care issues (before COVID-19), whereas several are new and applied specifically to address COVID-19 even without having been tested in rigorous controlled trials.
Telemedicine
Established nationally distributed programs have shown that telemedicine can increase access to routine and specialty care, even in low-resource, austere, and military operational contexts. 10 –13 Telemedicine is also known to be effective in numerous types of disasters, including health care emergencies and public health disasters, with several telemedicine/telehealth disaster response roadmaps published over the past 2 decades. 14 –18
Hollander and Carr succinctly identify the value of telemedicine and need to leverage existing systems for COVID-19 response. 19 One first-line approach is to transition all appropriate routine outpatient care to telemedicine encounters, as the Veterans Health Administration (VHA), Jefferson Health, and other organizations are doing. 19,20 This reduces the number of patients unnecessarily entering facilities, allowing hospitals to focus attention on the most acute or critically ill patients. The VHA and other organizations are also having patients with cold, flu, or COVID-19 symptoms call ahead for “forward triage,” which is the sorting of patients before they present for emergency care. 19,20 For patients with a diagnosis of COVID-19 and mild symptoms, the VHA is providing telehealth support so that patients can be monitored while they recover at home. 20 These measures will keep uninfected patients and health care providers safer. This approach frees physical resources for direct care when it is critically needed. 19
For health care systems or practices that have not previously used telemedicine, the Centers for Medicare and Medicaid Services (CMS) made several changes in March 2020 to facilitate rapid adoption and keep patients, providers, and communities safe. 21 Among other things, they broadened the range of providers who could deliver care through telemedicine and relaxed the rules about patient eligibility and audiovisual equipment requirements. 21 The American Academy of Family Physicians and the SCCM have practical guidance for systems and individual practices on how to quickly adopt telemedicine in response to COVID-19. 22,23
Telecritical Care
Telecritical care (TCC), which refers to technology-enabled critical care services, 24 can make COVID-19 critical care more available outside of the traditional intensive care unit (ICU) as well as safer and more efficient within it. TCC can make it possible to care for critically ill patients in hospitals without intensivists, thereby preventing costly and disruptive transfers of these patients. 25 In the current crisis, reducing transfers preserves personal protective equipment and reduces exposure for transport teams and vehicles. In hospitals with ICUs, TCC can be an important tool in rapid triage of the critically ill, ICU bed management, and early recognition of impending respiratory or hemodynamic decompensation. Remote monitoring and TCC software can help health care providers monitor numerous patients distributed among multiple ICUs. 19
Although predating COVID-19, systematic reviews have reported that TCC can reduce the length of time patients need to remain in the ICU and lower patient mortality. 24,26 Reduction in length of stays is necessary given the anticipated stress on the health care system due to the relatively large number of COVID-19 patients needing to be admitted to ICUs rapidly and in a compressed period of time.
Tiered Telementoring
Similar to tiered staffing models (defined by SCCM as a multidisciplinary team headed by an experienced critical care physician who oversees several non-ICU physicians and who, in turn, each oversees several ICU and non-ICU nurses, advanced practice providers, and other staff), 4 tiered telementoring can extend patients' access to clinical expertise even if they live in areas with limited providers and specialists. Or in crises when demand for specialty care is variable over time and space, telementoring can shift the expertise from areas of low demand to areas of high demand. Project Extension for Community Healthcare Outcomes (ECHO) is a telementoring network designed for continuing professional development and improving patient outcomes. 27 Operating in 34 countries, Project ECHO uses ongoing telementoring to equip primary care practitioners in rural areas with the knowledge they need to provide high-quality specialty care.
Development time and high costs are potential barriers to adoption of a telementoring system; however, there are several notable examples of implementing telementoring while containing costs. The U.S. Army's TATRC and Womack Army Medical Center demonstrated the use of “commercial-off-the-shelf” hardware and software to provide real-time telementoring and surgical expertise to remote caregivers (often with no more than an emergency medical technician's skill set) using phone calls and augmented reality with telestration. 28,29 Similarly, in Syria where years of war created a major health care crisis, North American and European intensivists worked with locals to create the “Syria teleICU,” also using “off-the-shelf” video cameras as well as free social media applications, a cloud-based electronic medical record (EMR), and virtual chat rooms. 30 For prolonged field care, which often involves caring for a critically injured person at or near the point of injury, an on-demand virtual critical care consult (VC3) service was created to support special operation forces medics. 31 Medics have telephone and e-mail access to intensive care doctors at all times, thereby increasing their capability to deliver complex care beyond their traditional scope of practice.
With respect to COVID-19 care, tiered telementoring allows experienced intensivists to provide consultation and support in the event of high volumes of patients who have or are at high risk of acute respiratory and organ failure. It has generally been estimated that one telemedicine intensivist can oversee 100–250 patients. 32 Although this ratio needs to be adjusted downward for inexperienced teleintensivists and new TCC programs, tiered telementoring still allows for care of more patients than does traditional bedside team models. Similar ratios have been estimated for TCC nurses. 32
Devices that enable Low-Contact Care, Communication, and Isolation
A key strategy in mitigating spread of infectious diseases, including COVID-19, is creating physical distance between providers, staff, and patients whenever possible. Within ambulatory clinics and hospital wards, mobile devices are being used for this purpose. Hollander and Carr describe the “two-tablet approach,” in which providers give COVID-19 patients (suspected or confirmed) a paired tablet when they arrive at the clinic, isolate them in a dedicated examination room, and then use the second tablet of the pair for provider–patient communication. 19 Robotics can also create distance between providers and patients, as in China and South Korea, where they have been used for ultraviolet surface disinfection of patient care areas. 33 “Smart” bracelets and rings, connected with a cloud-based AI platform, are being used to monitor vital signs and patient activity levels. 34
Near future mobile tools for COVID-19 low-contact care and isolation include the use of robotics for mobile monitoring of temperatures in areas of hospitals, nasopharyngeal and oropharyngeal swabbing, venipuncture, multiplex real-time assays, COVID-19 test sample transfer, and delivery of medicines to infected patients. 33 Smart tools designed for testing may also make it possible to test for COVID-19 infection at home, followed by a phone or video session with a provider to discuss results and next steps. 35,36
Information for Decision Making
Digital health tools and technologies make it possible to collect and analyze data rapidly and easily. The extraction and analysis of unstructured text data with natural language processing can be used to forecast disease outbreaks and spread. For example, a commercial digital health surveillance company used its AI algorithms that automatically collected and analyzed disparate data sets such as international news reports, airline data, and reports of animal-related illnesses to detect the emergence of COVID-19 weeks before the Chinese government announced travel restrictions. 37 Other AI systems that perform passive public health surveillance certainly exist. 38,39 One issue now is to train AI tools appropriately. However, the absence of clean and large amounts of data typically required for such systems is making this a challenge at the present time. 40
Mobile phones have been used for quite some time for surveillance of risks to health. This is often done by using the communication functions of the phones and relying on individual and organizational reporting. 41,42 For COVID-19, mobile phone global positioning system data have been used to show the travels of a known infected person (i.e., “contact tracing”); this information can be used to warn others known to have been in the same locations. 43,44 Implementation in the U.S., however, will require changes in privacy policies, laws, and comprehensive COVID-19 testing. 45 –47
At the patient level, mobile applications have been used for several decades to support patient self-care behaviors and dissemination of health interventions. 48 Bluetooth-connected monitoring devices can send patient health data to remote providers, and short health questionnaires administered to patients through mobile applications can regularly apprise providers of patients' symptoms and psychosocial well-being. 49,50 By avoiding patient travel to health care facilities, use of mobile applications might make it possible to monitor COVID-19 patients remotely, quickly determine whether they exhibit COVID-19 symptoms, and potentially manage their care in place (i.e., at their home), even when traditional paradigms might lead to a hospital admission.
Future Application of Digital Health Tools for Major Crises: The National Emergency Telecritical Care Network Concept
Overview
Although the aforementioned strategies, tools, and technologies may significantly enhance current capabilities for COVID-19 treatment and decrease spread of the disease, a broader long-term strategy is needed to increase the capacity of critical care assets in future times of need. Therefore, a NETCCN should be developed through public–private partnerships and implemented for future health care emergencies. NETCCN would combine and build upon the existing telemedicine approaches and other digital health technologies as well as provide the flexibility to incorporate new technologies as they become available.
The NETCCN would be a cloud-based low-resource stand-alone health information management system for the creation and coordination of flexible and extendable “virtual critical care wards.” This system would continually monitor and classify populations according to health status and predict population risks. These virtual wards would bring high-quality critical care capabilities to nearly every bedside irrespective of location (Fig. 1).
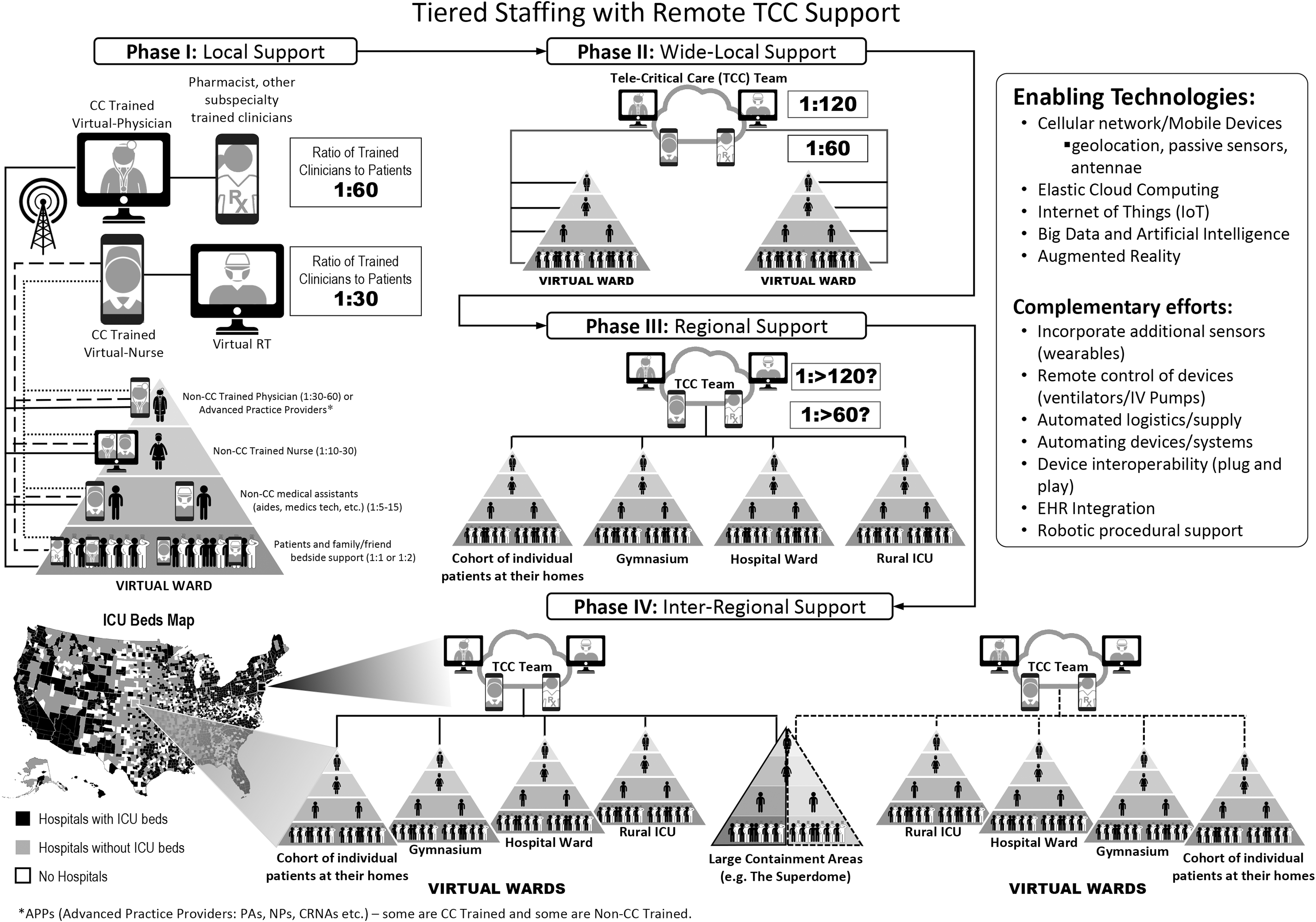
National emergency telecritical care network concept. CC, critical care; CRNE, Certified Registered Nurse Anesthetist; EHR, electronic health record; ICU, intensive care unit; NP, Nurse Practitioner; PA, physician's assistant; RT, respiratory therapist; TCC, telecritical care.
At the system level, combining digital health tools with real-time audiovisual communications will allow on-demand geographic expansion of limited critical care expertise and extension of expert specialist management. The NETCCN concept may provide a critical backbone during future health care emergencies. For example, in the event of another novel infectious disease, NETCCN would reduce the need for transfers of patients and specialty health care professionals between regions and facilities. Advances in analytics, AI, and data visualization and reporting would provide tools for rapidly deployable command and coordination structures that use real-time feedback to inform both resource allocation and decision making. Best practices and lessons learned can be fed forward to drive iterative process improvement at every level.
For NETCNN Phases I and II, the system would operate within one geographic area, typically with just one or two virtual wards, for use by local clinicians and other local personnel licensed by that state to provide telemedicine and other services. For NETCCN Phases III, the system would operate across multiple states, and for Phase IV, it would operate across all 50 states and territories. There are multiple “wards” in these phases, in a variety of settings, some of which may be temporary (gymnasium, convention center, etc.). NETCCN Phases III and IV require the extension of telemedicine services in most or all states and the authorization of out-of-state providers to give care (telemedicine or in person), even to patients they have not previously met in person. 51
Challenges to Implementation
Preparing to adapt telemedicine and digital health modalities to support NETCCN has numerous technical, administrative, and legal obstacles that must be surmounted.
Technical challenges include a range of hardware, software, and communications concerns. Clinics, units, and care provider facilities have traditionally purchased specific types of equipment and software, often at great expense, to build a telemedicine program. These tools may not be available during a disaster and can be difficult to scale rapidly or to volume. Mobile health, within the context of the NETCCN, offers a compelling solution to these challenges by using multiple channels of communication such as low-cost synchronous audio/video, asynchronous messaging, and the ability to continuously monitor health. These solutions are ubiquitous, easy to scale, and easy to establish/maintain in very austere settings (Syria, hurricanes Maria and Harvey, etc.).
Siloed, proprietary medical devices, and EMRs also encumber the ability to share information beyond a health care system's own network. Interoperability and communication across major existing EMR systems and medical devices are necessary for a model such as the NETCCN to be successful. Secure HIPAA compliant services such as the Office of the National Coordinator for Health Information's Health Information Exchange can help bridge these gaps in the short term until a national secure standards-based internet of things framework can be put in place. 52 –54 Given the probable demands that will be placed on clinician time during a disaster, the NETCCN needs the ability to simply and efficiently document in real time. Automated data collection functions that could be enabled through device interoperability would allow the NETCCN solution to work anywhere at any time with “plug-and-play” convenience. Cloud-based information storage, including ability for later offloading medical data (through PDF or HL7), would facilitate reporting and inclusion of emergency documentation into patients' medical records.
Licensing and credentialing barriers must also be addressed. Default medical credentials limit care to the state in which a provider is licensed to practice medicine. Policy and regulatory requirements restricting the type and mode of care often lack the language to account for telemedicine. Many states, however, have recently established reciprocity agreements in the midst of this national emergency to allow providers to expand their care footprint beyond their own state. In addition, telemedicine/telehealth services are explicitly mentioned as authorized modes of care in most states. 51 These new requirements would need to be expanded further and aligned across all states and territories.
Administrative and policy concerns include reimbursement for care provided. 2,3,21,51 –53 CMS defines the billing and regulatory requirements for Medicaid eligible recipients. As already stated, CMS has eased the regulations for telemedicine in response to the COVID-19 pandemic. Moreover, clinics can submit for a waiver to expand what covered services can be reimbursed, allowing the state to provide care for people who might not otherwise be eligible under Medicaid.
Summary
Recent national and global events have demonstrated the impact of a large-scale health care emergency on the existing health care infrastructures and the challenges faced by health care facilities to surge to meet these demands. One approach to meeting these challenges is to leverage existing telemedicine and other digital health technologies to expand local, regional, and national health care capability and capacity. Developing a flexible, scalable, resilient, and, most importantly, interoperable NETCCN is essential to ensuring that the necessary digital health ecosystem is present to respond when future disasters or emergencies strike. The capacity and capabilities gained from a sustained NETCCN, now and between crises, would allow for enhanced care provision, distribution, and rapid deployment at scale to make our nation safer.
Footnotes
Acknowledgments
The views expressed are those of the authors and do not reflect the official policy or position of the U.S. Army Medical Department, Department of the Army, Department of the Air Force, Department of the Navy, Department of Defense, or the U.S. Government. The authors wish to thank LTC(P) Justin Stewart, DO, MBA, MHA, and Jeanette Little, MS, for their organizational support and insights during the development of this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.