
Abstract
Background:
Many e-health services were launched after countries relaxed their telehealth regulations to combat the coronavirus disease 2019 (COVID-19) pandemic. e-Health technologies that support person-centered health care are crucial for the patient's needs. In this systematic review, we examined how e-health applications are used to support person-centered health care at the time of COVID-19.
Methodology:
Literature was systematically searched without language restriction and publication status between January 1 and May 25, 2020, to describe e-health's support on the person-centered health care to control the COVID-19 pandemic. PubMed, ScienceDirect, and CINAHL, MedRxiv, and Web of Science were used. Two researchers independently assessed the eligibility of each retrieved record. All included studies were subsequently rescreened by the researchers. The systematic review was conducted in accordance with preferred reporting items for systematic reviews and meta-analyses guidelines.
Results:
We identified 60 articles and selected 8 studies that met the inclusion criteria. Most of the studies used e-health technologies to facilitate clinical decision support and team care. Patient's engagement and access to health care from their homes were enhanced using telehealth and mobile health. Electronic health records were used to avail reliable data to health care providers and health authorities to make evidence-based decisions.
Conclusion:
Although there are limited studies to evaluate the effectiveness of e-health technologies for person-centered health care, the reviewed studies indicated e-health's potentials to improve the quality of health care and personalized health systems during COVID-19 pandemic. Further research should be done to better understand applications of e-health to improve the quality of health care and patients' outcomes and evaluate its cost-effectiveness.
Introduction
On December 31, 2019, clusters of cases of coronavirus disease 2019 (COVID-19) were officially reported from Wuhan, Hubei Province, China. 1 COVID-19 is an illness caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 2 Owing to the rapid increase in the number of cases outside of China, the World Health Organizatoin (WHO) officially declared the outbreak a pandemic on March 11, 2020. 3 There was an urgent need to reduce exposure to SARS-CoV-2 by enabling both patients and clinicians to interact and, at the same time, reduce the spread of the virus in health care settings. Electronic health (e-health) applications are used as solution to support person-centered health care and control the spread of COVID-19.
The current pandemic has caused digitization to flourish in the health care sector. e-Health, which is a combined use of electronic information and communication technology in the health sector, 4 has a high potential for optimizations and savings in the majority of health care systems worldwide. e-Health solutions can support care and treatment by exchanging treatment-relevant data among health care providers or between patients and health care providers in compliance with data protection regulations and by providing documents that are specially tailored to the needs of teleintensive care of COVID-19 patients.
The utilization of advanced technologies might also be required by the health care systems to enhance patient-centered health care. Essential components of such a virtual hospital consist of both telehealth and electronic health records (EHRs). A patient-centered health system is a system focusing on patients' needs without introducing adverse effects. Virtual visits are one way of creating a more patient-centered health system. 5
Telehealth, a component of e-health, includes telemedicine, mobile health (m-health), and electronic medial record (EMR) or EHR. 6 m-Health involves the use of mobile communication systems to manage health care activities, share medical data, analyze health information, and improve overall patient outcomes and experience. 7,8 Telehealth strengthens patient-centered medical consultations of patients in their homes and increases their access to medical advice. Thus, it functions as a connector between the patient's health care team and self-care. 8 m-Health involves the use of mobile communication systems to manage health care activities, share medical data, analyze health information, and improve overall patient experience, such as their short-term outcomes. 9,10 Such improved health care access is one of the main principles of patient-centered medical homes.
Informatics being part of e-health has the potential to support patient-centered care. 10 Working toward the preferences and values of patients is person-centered health care. 11 In person-centered health care, patients are involved in understanding their interests while deciding on treatment options. Person-centered health care incorporates most of the aims and tasks of health care systems identified by the WHO. 12 Evolution in informatics areas within patient-centered health care encompasses clinical decision support, registries, team care, care transitions, personal health records, telehealth, and medical measurement. As identified by Bates and Bitton, these significant areas support the comprehensive system of patient-centered medical homes. 13 Among these areas, team care and care transitions are goals of patient-centered care, whereas clinical decision support, personal health records, and telehealth are ways to attain those goals. Registries and measurements are ways to handle quality improvement. 10
Bates and Bitton supported new communication tools to connect patients to their health care team and classified care tasks among patient-centered medical home providers. 13 During disease epidemics, new technologies may be designed, or the available technologies can be used to support patients, families, and health professionals. 10 Even if many studies are done on the use of e-health technologies during the COVID-19 pandemic, it is vital to identify those particular studies on e-health applications that support person-centered health care. In this review, we have summarized the findings of the studies to produce reliable evidence to inform health care providers during public health emergencies to improve patient-centered care.
Objective
To review literature that describes how e-health can be used to support the person-centered health care at the time of COVID-19.
METHODOLOGY
Literature search
Literature was systematically searched without language restriction and publication status between January 1, 2020, and May 25, 2020, to describe e-health's support on the person-centered health care to control the COVID-19 pandemic. PubMed/MEDLINE, ScienceDirect, and CINAHL were used. Furthermore, MedRxiv and Web of Science (ISI Web of Knowledge) were used for searching. Words used for searching included e-health, internet, telemedicine, telehealth, m-health, smartphones, electronic health record, patient-centered medical home, person-centered health care, severe acute respiratory syndrome coronavirus 2, SARS-COV-2, 2019 novel coronavirus, 2019-nCoV, and COVID-19. Both qualitative and quantitative studies were reviewed. MeSH descriptors and the corresponding number of hits per database are presented in Appendix A1.
Study inclusion
Two researchers independently assessed the eligibility of each retrieved record based on the title and abstract. If the information was unclear, the full-text article was screened. All included studies were subsequently rescreened (i.e., double screened) by the researchers (Appendix A2). The included studies were required to meet the following inclusion criteria: It must be published as an article It must be written in English language It must be published from January 1 to May 25, 2020 SARS-COV-2 OR COVID-19 and internet and related to person-centered health care SARS-COV-2 OR COVID-19 and e-health and related to person-centered health care SARS-COV-2 OR COVID-19 and telemedicine/telehealth and related to person-centered health care SARS-COV-2 OR COVID-19 and m-health and related to person-centered health care SARS-COV-2 OR COVID-19 and smartphones and related to person-centered health care SARS-COV-2 OR COVID-19 and EHR/EMR and related to person-centered health care.
The systematic review was conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses guidelines.
Results
MAIN FINDINGS
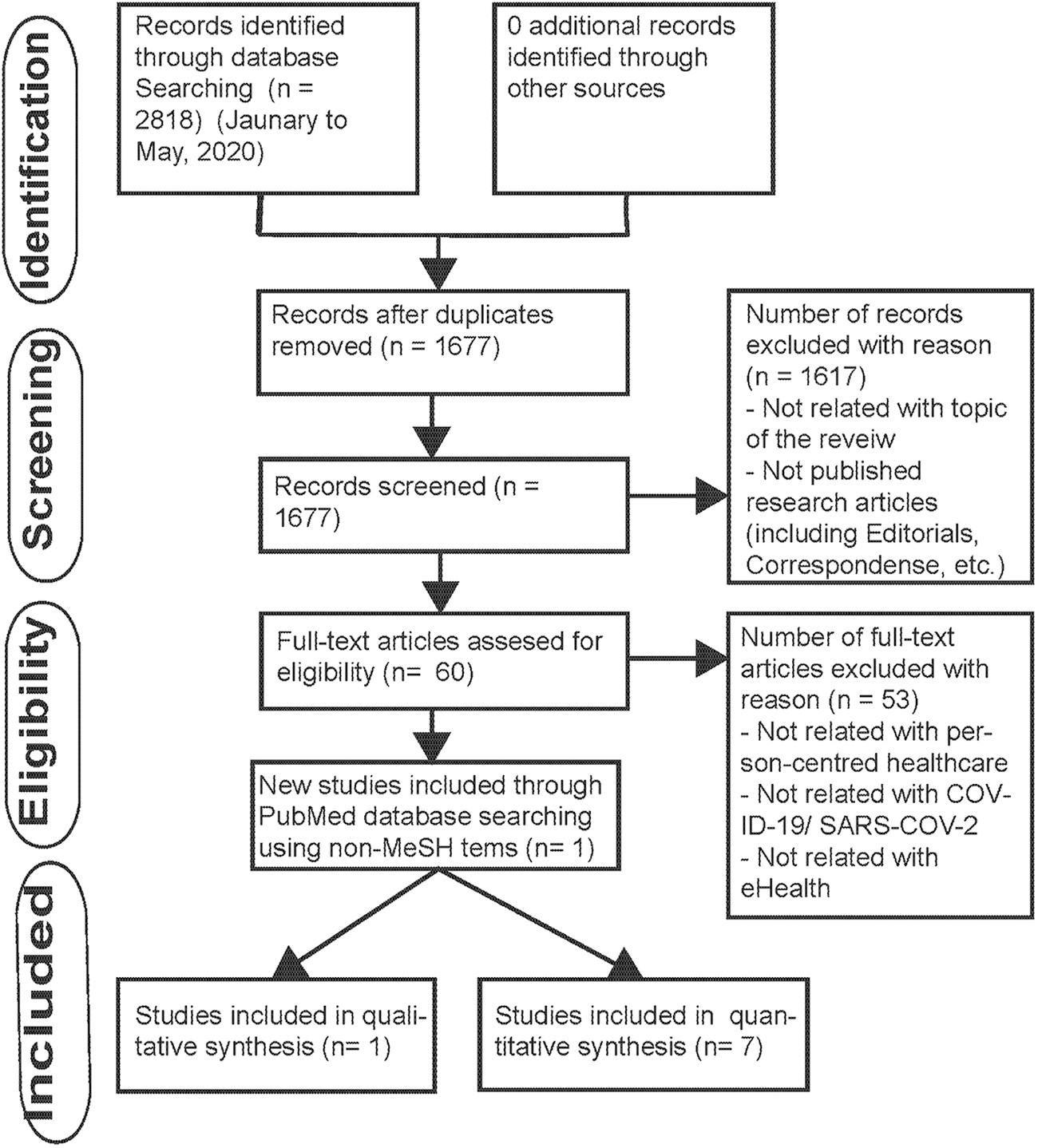
After searching on the databases, we were able to identify 2,818 sources. The flowchart, displaying the results of the literature selection process, is shown in Figure 1. Of the original identified sources, 1,677 sources remained after the removal of duplicates. Then, 60 articles were selected after examination of the full texts from the remained sources. Finally, we included eight studies that aim to show applications of e-health to support person-centered health care during the COVID-19 pandemic. The features of the eight publications that fulfilled the inclusion criteria are summarized in table 1 and are discussed hereunder in detail.
PICO-diagram, defining the Population, Indicator, Comparator, and Outcome.
Summary of the Findings of the Selected Studies
COVID-19, Coronavirus disease 2019; EHR, electronic health record; EMR, electronic medical record; GIS, geographical information system; m-health, mobile health; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; UCSF, University of California, San Francisco.
KEY CHARACTERISTICS OF THE SELECTED STUDIES
e-Health technologies used to support the goals of person-centered health care (team care and care transitions) and the other informatics areas telehealth, personal health records, registries, measurement, and clinical decision support are explained by different authors of the following selected articles based on their aims. Since most of the studies we reviewed paired EHRs, personal health records, and telehealth with person-centered health care, we did not mention them separately while making classifications in this section.
E- HEALTH SUPPORTING REGISTRIES AND CLINICAL DECISION SUPPORT IN PERSON-CENTERED HEALTH CARE DURING THE COVID-19 PANDEMIC
EHRs have a variety of applications in the health care system in clinical care, administration, clinical research, and finance. 14 Judson et al. deployed a digital self-triage and self-scheduling tool with coronavirus symptom checker prepared from an EHR. The tool was used by all primary care patients in a large academic health system University of California, San Francisco (UCSF), to address the COVID-19 pandemic. The tool has high sensitivity (87.5%) for identifying emergency-level illness of COVID-19 and high specificity (89.5%) to suggest self-care and minimized the time of triage. 15
E -HEALTH SUPPORTING TEAM CARE, MEASUREMENT, AND CLINICAL DECISION SUPPORT IN PERSON-CENTERED HEALTH CARE DURING THE COVID-19 PANDEMIC
Telemedicine is a vital aid to give access to health care services to people living in remote areas during pandemics of COVID-19. 16 Khairat et al. conducted a cohort study and analyzed COVID-19–like symptoms of virtual visits of patients through phone or video calls before confirmed cases of COVID-19 to compare the results with the confirmed COVID-19 cases. In February before any confirmed cases, the authors were able to identify 57.3% of COVID-19–like cases in areas that have a high number of people and where cases are in proximity to airports. Most of the residents in this area were later diagnosed to have COVID-19. 17 Virtual primary health care allows the safe management of mild cases of COVID-19. 18 Hong et al. used internet volume data from Google Trends to measure population-level interest in telehealth and telemedicine during the time of COVID-19. The authors found that the population's interest in the United States in telehealth was high when the number of COVID-19 cases increased. Out of 6,146 U.S. hospitals, 60.8% deployed telehealth, and 13.4% had tele-ICU capability. Northeast and west survey regions showed a higher population interest in telehealth, whereas the midwest region has a high number of hospitals that adopted telehealth. 19 Telemedicine can support the management of COVID-19 and prevent its transmission between health care providers and patients. Huang et al. utilized a self-quarantine model incorporating an online and offline multidisciplinary quarantine observation. The latter was prepared using a Web Chat group to follow two patients diagnosed with COVID-19 through their phones based on their current symptoms. The online management enhanced the self-management ability of patients and improved their clinical outcome. 20
Information between patients and health workers can be easily shared using mobile phones through reliable software applications. Mobile phones are important for remote communications and effective management of the SARS-CoV-2 outbreak. 21 Zamberg et al. undergo utilization-focused evaluation of a m-health platform used by medical staff, particularly physicians of the children's hospital at the University of Geneva, Switzerland. The platform was used to distribute locally approved and the latest information about the SARS-CoV-2. The medical staff who used reliable m-health platforms through mobile app felt comfortable for the care of patients, particularly when encountering specific clinical inquiries. A majority (83.3%) of the staff who used the platform said it is easy to find information about SARS-CoV-2. Among the 332 coronavirus-related documents that were made available to the medical staff through the mobile platform, 35.6% were viewed. The medical staff preferred the platform than other sources of information. 22 Diagnosis of disease and patient treatment can be performed on time by medical experts by using videoconferences. 23 Ren et al. used a mobile telehealth system (MTS) through mobile integrated technology to share patient information, support with disease diagnosis, and assist case discussion between health care workers using videoconsultation during the COVID-19 pandemic. 24
E -HEALTH SUPPORTING CARE TRANSITION, CLINICAL DECISION SUPPORT, AND MEASUREMENT IN PERSON-CENTERED HEALTH CARE DURING THE COVID-19 PANDEMIC
e-Health can aid surveillance systems to trace contacts, follow patients, and control pandemics. Gong et al. 25 performed a pilot study of COVID-19 surveillance using new integrated medical informatics technologies of the Honghu Hybrid System to control COVID-19 in the city of Honghu in Hubei, China. The Honghu Hybrid System was created to collect and analyze COVID-19–related data from a case reporting system, diagnostic laboratories, EMRs, and social media on mobile devices. The syndromic surveillance was given through a mobile phone-based social media platform and covered >95% of the population of Honghu.
Tracking at real-time highly organized digital syndromic surveillance data was supported by a spatial analysis that helped local authorities and health workers to make evidence-based policy-related decision and evaluations on time. Therefore, Honghu Hybrid System enabled effective and efficient surveillance of COVID-19 in Honghu. 25
Similarly, Gong et al. studied multicenter internet hospital users' data. They classified them into varieties of epidemic counselees based on their online epidemic-related consultations of doctors in the general public hospitals in China during the COVID-19 outbreak. The authors were able to identify that 94% of the counselees had symptoms related to COVID-19. Of the 190 severe conditions, 137 (72%) counselees did not attend an offline visit for receiving additional management. 26
Discussion
The results of this review indicate how the internet, m-health solutions, telehealth, telemedicine, and EHRs can rapidly be used to provide support for patient-centered health care to prevent and contribute to controlling the COVID-19 pandemic. Most of the authors integrated the EHR, which is the primary domain for person-centered health care 13 and telehealth to support patient-centered care. Patients at UCSF had an appropriate and effective self-triage after cooperating with health professionals while staying at home. 15 A clinical EHR that operates with other electronic health systems was built in low resource public health emergency set up to assist data collection during the Ebola epidemic in 2015 to take preventive and control measures. 27
Primary video visits were convenient and efficient ways for patients than in-person visits. 28 A preferred virtual care visit was utilized to analyze the patients' virtual care data to identify the patients' COVID-19–like symptoms during their virtual visits. The virtual visit can be used to triage patients efficiently and predict areas that could have a high number of COVID-19 cases. 17 Patient-centered web-based solutions containing data, virtual care, and the patient app were also found to be adequate to do evidence-based practice and manage COVID-19 pandemics. 29 Although the population's interest in the United States in telehealth was high, no association was identified between the population's interest and the proportion of hospitals that adopted telehealth. This may indicate that the population's need may not be satisfied by the existing telehealth facility, as the authors suggested. 19 One way to improve this demand may be achieved by informing stakeholders that telehealth and e-health, in general, are vital instruments to dampen the rise in health care costs.
Telehealth strengthens occupational health of health care providers and minimizes the costs of epidemics by reducing the spread of infection. e-Health supports the coordination of health service providers in the treatment of patients. Adverse interactions between treatments can be avoided better than before—as well as inefficient treatments. Physicians and patients will demand better coordination and communication in their treatment approaches.
Furthermore, the populations' internet search volume data from Google Trends should be categorized as inquiries related to COVID-19 prevention, diagnosis, and treatment and followed appropriately to understand and enhance the populations' interest in telehealth.
Videoconferences are essential components of telemedicine and enable health care workers to do remote examinations of the patient's condition and share relevant information concurrently without making direct interaction, subsequently preventing the spread of SARS-Cov-2. 16,30 An MTS was used to avoid coronavirus transmission and assist case discussions among health professionals. 24
Telehealth technologies can connect a patient's medical care team and self-care routines. 19 Data obtained from patients can help health care professionals to make shared decisions and treat illness based on the patients' preferences. 31 This was exemplified by two patients who were physicians and diagnosed with COVID-19. 20 However, including more patients other than physicians in the study could have helped to gather more relevant evidence to generalize. Telemedicine can also be used in epidemics to treat patients and control outbreaks. 32
The utilization of integrated electronic patient registries with other technologies has been shown to improve quality measures. 10 Internet hospitals allowed physicians to manage patients with mild illness online. Analysis of online consultation data can help to understand the characteristics of the transmission rate of the pandemic in an area. The data also indicated that the majority of the counselees who were classified as having severe conditions did not attend a physical visit for the required management. Although the authors identify this gap, further studies are necessary to know the reason behind this. 26
Also, a smartphone-based m-health application was used to support contact tracing and improve access to surveillance data. 33 Medical professionals in children's hospital at the University of Geneva were able to get access to reliable information about SARS-CoV-2 from an m-health platform to give care for their patients comfortably. The institutional leaders in the hospital later agreed to use the platform within all medical departments in the hospital. The fact that only a few of the documents were viewed and the tendency of the staff to use other sources of information indicate that the authors should identify the gaps to consider the platform as full reference. 22
The quality of clinical care of patients is improved by technologies that advocate collection, process, and analysis of clinical data. 10 A hybrid system created by the integration of technologies can be used to collect and analyze COVID-19–related data to support surveillance and clinical decision and give necessary information to control COVID-19. 25 One study identified an online self-management application (OncoKompas) among cancer survivors that was feasible with high adoption, implementation grade, high mean satisfaction score, and a positive net promotor scale. Regardless of their findings, the researchers suggested also considering parameters such as the time it takes to use OncoKompas and measurement precision to enhance the feasibility of e-health application. 34 Contact tracing apps and social media can be used for COVID-19 prevention and surveillance. 35
Designing a new reliable system is challenging during emergencies such as epidemics than rapidly adapting already established system. 27 Therefore, the use of existing e-health technologies to rapidly detect COVID-19, protect health providers, and improve patients' clinical outcomes is appreciated. The authors deployed telehealth to control the spread of SARS-CoV-2, avoid inappropriate medical-seeking behaviors, and save medical resources. They were able to create and support personalized health systems for patients and citizens to provide person-centered health care. The patients' information security was also protected in the meantime. However, most of them failed to indicate the cost-effectiveness of the implemented e-health technologies and prove its effectiveness on patients' clinical outcomes during the coronavirus pandemic. Therefore, further researches should be done in these areas.
In general, we believe that successful digital solutions should be developed from the patient's perspective and focus on their needs and everyday activities, also outside pandemic situations. This will fundamentally change the care processes and the use of health services; the point of care will shift more and more from the physician's office and clinic to the patient.
The interaction of software, sensors, and medical technology also opens up completely new diagnostic and therapeutic options in extreme situations such as the COVID-19 pandemic.
STRENGTHS AND LIMITATIONS OF THIS REVIEW
This article has been written early in the still ongoing pandemic of COVID-19 and, therefore, presents only a snapshot of the applications of e-health to support person-centered health care at the time of COVID-19 pandemic.
We identified relevant articles through a comprehensive search of literature using well-defined inclusion criteria. However, we included only studies written in English language. Although the evidence we found is not adequate to generalize, the e-health technologies are important to support and improve the effectiveness and efficiency of the patient-centered health care during the COVID-19 pandemic.
Footnotes
Acknowledgments
We thank program facilitators for collaborating with the University of South-Eastern Norway, Norway, and the University of Gondar, Ethiopia, and their assistance to develop this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.