
Abstract
Background/Introduction:
The COVID-19 pandemic poses enormous resource challenges to hospitals. Telemedicine is increasingly recognized as an attractive tool to alleviate resource strains. Herein we describe the rapid implementation and sequential process improvement (PI) of a centralized telehospitalist service to coordinate and optimize management of large number of COVID-19 patients in a tertiary and quaternary care hospital very close to the New York City epicenter.
Methods:
Prospective multidisciplinary PI meetings were held weekly between March 23 and May 10, 2020, and consensus service modifications were implemented for the following week. Inpatient census data, telehospitalist intervention volumes, and service utilization statistics were collected.
Results/Discussion:
Between March 23 and May 10, 2020, a total of 745 COVID-19 patients were admitted to the general medical wards. The telehospitalist service performed 1,136 audiovisual (AV) patient assessments, 379 best practice interventions, cohorted 108 patients, and conducted 170 remote family conversations. During the consecutive PI cycles, a number of adaptations in AV setup, care standardization, patient logistics, communication, and consultative functions were made to load balance the bedside hospitalist teams. As the COVID-19 hospital census increased to peak levels, the most value was added through facilitation of communication and collaboration between the bedside clinical teams, the infection prevention and control teams, and patient logistics team.
Conclusions:
A telehospitalist service can be rapidly implemented with basic telemedicine equipment. Processes/this functions can be sequentially adapted to quickly changing needs during conditions such as the COVID-19 pandemic that very quickly can place extraordinary strains on hospital resources.
Introduction
New York State has been described as the epicenter of the United States COVID-19 outbreak, with 380,892 cases and 24,442 deaths confirmed as of June 11, 2020. 1,2 Westchester Medical Center serves as a tertiary/quaternary care hospital located in Westchester County, ∼48 km north of New York City. Westchester County had 34,106 cases and 1,531 confirmed deaths as of June 11, 2020, which is the fourth highest number of cases in New York State (after New York City [which is a collective of five counties], Nassau County, and Suffolk County). 1,2
The COVID-19 pandemic has been posing the following often unprecedented challenges to hospitals
3
: a rapidly growing sick patient population with high risk of sudden clinical decompensation,
4,5
changing and evolving diagnostic testing options and turnaround times, strained infection prevention and control (IPC) resources, the need to streamline the placement and cohorting of patients, general ward and ICU bed shortages, strained patient placement/logistics resources, need to limit avoidable health care worker exposures, need to conserve personal protective equipment (PPE), the challenge to communicate with families unable to visit their loved ones in the hospital, the need to follow-up on discharged patients to check on their continued recovery, provide continuity care, and prevent readmissions to the hospital.
Telemedicine is increasingly recognized as an important tool in clinical care delivery, especially in times of resource strains such as disasters or pandemics. 6 –9 Our existing network telemedicine infrastructure (e-health center, see Fig. 1) extends access to specialty providers for in-network and out-of-network hospitals providing clinical support and expertise to better meet the needs of the Hudson Valley patient population.

WMCHealth's eHealth Clinical Operations Center coordinates a variety of telemedicine programs across the hospital network and beyond.
We implemented a centralized continuous tele-ICU support system for all adult ICU beds at our Valhalla campus in 2016. The tele-ICU helps with standardizing clinical care and supervising clinical best practices from a central location. It also serves important clinical workload balancing functions by synergistically extending the reach of bedside providers. In addition, the tele-ICU program has sequentially taken on patient logistics functions such as centralized ICU bed management and outside hospital ICU transfer coordination. 10
Posed with the challenge of a rapidly growing COVID-19 inpatient population in critical care units (Fig. 2), we adapted the existing role of the tele-ICU physician, giving them new tasks and responsibilities that centered around unloading the bedside critical care team, focusing on care standardization, and accelerating care plans 24 h a day. Given the increasing number of COVID-19 patients on the general medical wards, we also rapidly implemented a new analogous role for the general medical ward by creating a telehospitalist service. These providers helped to effectively coordinate care standardization, supervising clinical best practices, and communicating effectively with patient logistics and IPC teams. The combination of these tasks resulted in load balancing for our bedside internal medicine hospitalist teams, as a mirror image of the tele-ICU physician.
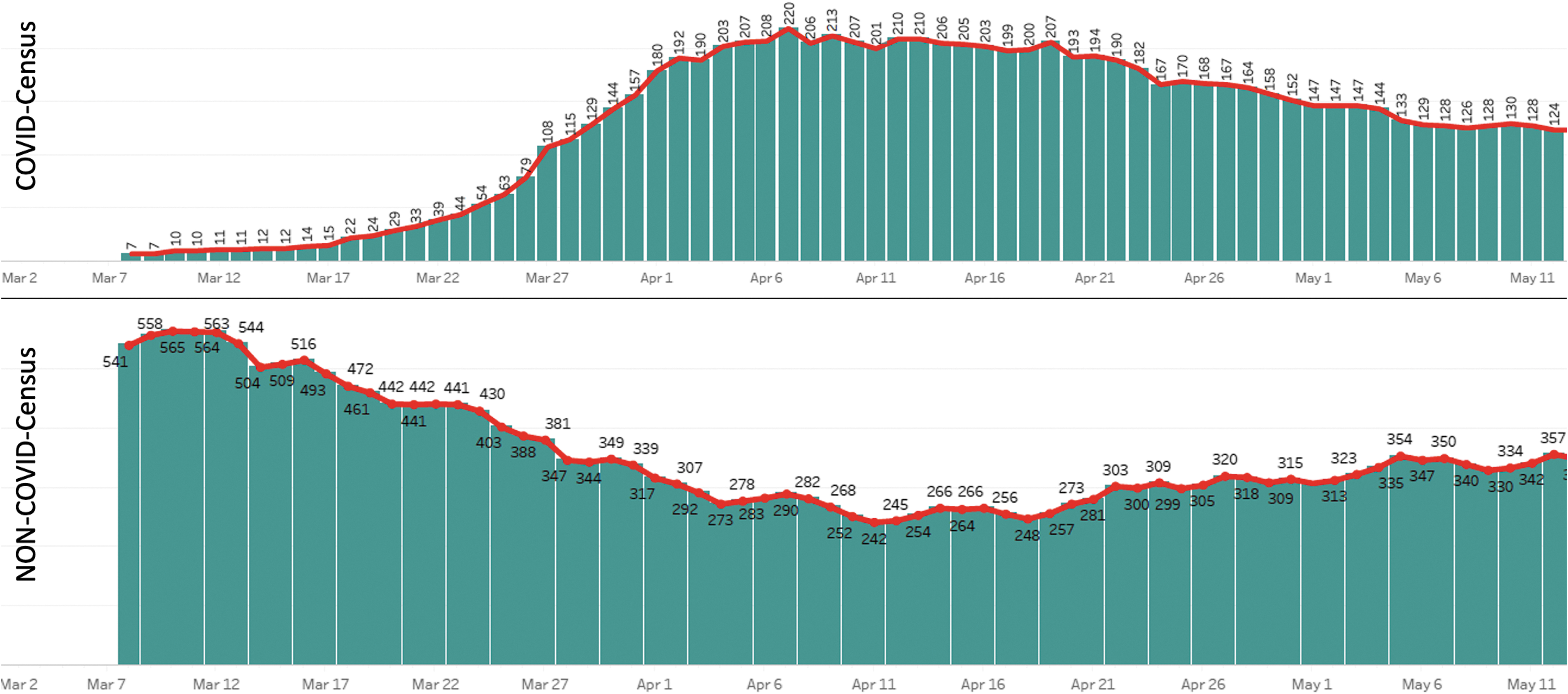
COVID-related general medical ward admissions (top) versus non-COVID–related admissions (bottom). Mid-March saw a rapid increase in daily number of inpatient admissions and a concomitant reduction of non-COVID admissions.
Herein we describe our preliminary experience of rapidly planning, implementing, and sequentially adapting and improving this novel COVID telehospitalist service to match the rapidity of influx and overall large number of COVID-19 inpatients.
Methods
We performed a descriptive study of telehospitalist service implementation combined with weekly prospective multidisciplinary process improvement (PI) cycles at Westchester Medical Center/New York Medical College. The PI meetings included data review and group discussions (patient placement/logistics team, COVID-hospitalist team leaders, telehospitalists, telemedicine leadership, information technology [IT] leadership, IPC leadership, as well as patient experience team representatives). Consensus service modifications were implemented weekly for a 7-week period from March 23 to May 10, 2020. This study was exempt from institutional review board review as it does not constitute human subjects research. Descriptive statistics on inpatient admission volumes, telehospitalist intervention volumes, and service utilization were calculated through Microsoft Excel (Microsoft, Redmond, WA).
Results
Starting in mid-March of 2020, we encountered a rapid increase of COVID-19–related general medical ward admissions (Fig. 2).
A first planning meeting to explore telemedicine strategies between e-health leadership and hospitalist medicine leadership identified the goal to create a central support system for the rapidly expanding COVID-19 general medical ward patient population, modeled after the existing tele-ICU physician function. It was jointly decided that internal medicine board-certified physicians with reduced capacity levels due to COVID-related service limitations (e.g., gastroenterologists and endocrinologists) or belonging to higher risk groups for severe COVID-19 disease (i.e., significant medical comorbidities) would be recruited for the new role of telehospitalist and would be operating 24/7 out of the existing e-health operations center, thereby enabling use of the existing administrative and IT support functions. There was consensus that with the COVID-19 case volume rapidly expanding, this new service would need to be implemented quickly and subsequently improved and adapted “on the fly” to maximize its utility. A prominent early goal was also to save PPE by performing eligible functions such as in-room equipment monitoring, patient audiovisual (AV) check-ins, and other communications through telemedicine. Early involvement of IT support was crucial to help decide which “off-the-shelf” AV technology solution could be purchased, adapted to this use case, and set up in a timely manner. To rapidly gain experience, we decided to launch a pilot phase by deploying simple mobile AV equipment (iPADs mounted on five-wheeled carts, see Fig. 3) to eight patient rooms on the designated COVID inpatient floor. Twelve-hour shifts were assigned, and providers were trained on using the AV software (VIDYO Desktop V3.6.9; VIDYO, Inc., Hackensack, NJ).
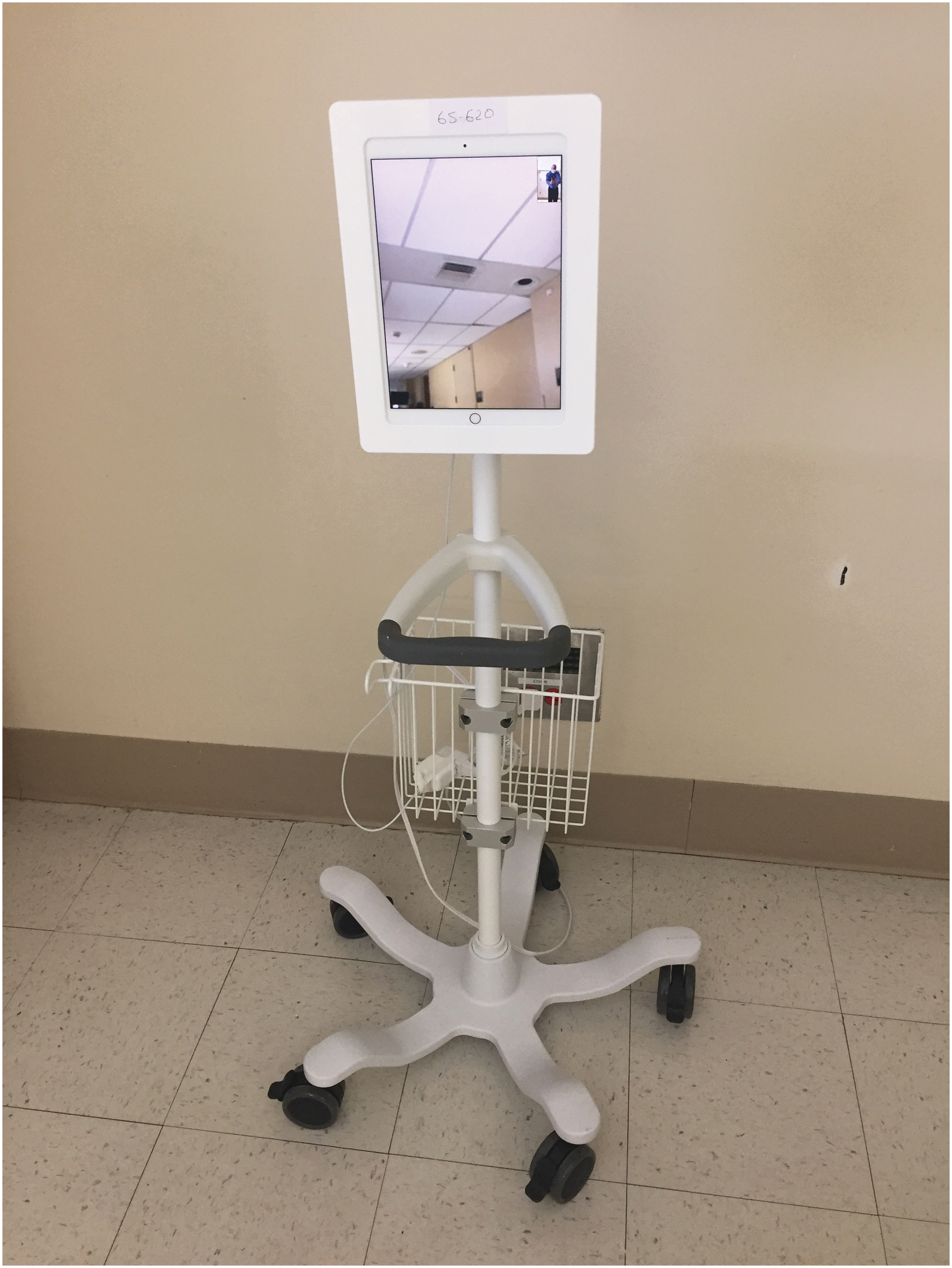
Simple mobile AV equipment setup consisting of an iPAD (Apple, Cupertino, CA) on a five-wheeled mobile stand (Amico, Richmond Hill, CA) and VidaMount VESA tablet enclosure (VidaBox, Plain View, NY). AV, audiovisual.
The first PI cycle was used to identify, discuss, and rectify any equipment issues. As more mobile AV units became available, the deployment was subsequently expanded to a total of 46 inpatient rooms. The second and third PI cycles identified that a wider circle of medical providers wanted to access AV units for patient communications and AV check-ins (i.e., medical consultants, bedside nurses, dialysis nurses, social workers, and dieticians). We, therefore, decided during the third PI cycle to switch the model from single AV units in patient rooms accessible from desktop computers at nursing stations to a paired model with one AV unit positioned outside the patient room and one AV unit positioned in the room ( Fig. 4A, B). This enabled access to the patient room AV unit from either outside the patient room through the paired AV unit (Fig. 4B, red connections) or through any hospital computer workstation equipped with the AV software (Fig. 4B, dark blue connections to nursing station or light blue connections to telemedicine operations center).

The second and third PI cycle added the functions of cohorting of confirmed COVID-positive patients and monitoring of 12 lead electrokardiograms (EKGs), magnesium levels, and corrected QT intervals (QTc) for patients treated with QT-prolonging medications such as hydroxychloroquine and azithromycin. The growing resource strain on the IPC team led to the suggestion during the second PI cycle discussion to centralize monitoring of appropriate isolation status and associated orders through the telehospitalist, which was further expanded after the third PI cycle discussion.
Given the difficult situation of patient families not being able to visit their loved ones in the hospital, the patient experience team was quickly confronted with a large volume of family calls wanting to have more information. To adapt to this change, a workflow was designed to streamline communication between the patient experience team fielding family calls and the frequently changing hospitalist bedside teams with the telehospitalist acting as an intermediary. In addition to mediating the family requests, the telehospitalist also increasingly took on the family communication function on a case-by-case basis in collaboration with the different bedside hospitalist teams. An important new function was added to the telehospitalist role after the fifth PI cycle discussion brought up a need for internal medicine consultation services for a newly created inpatient psychiatry COVID unit with a census of 6–10 patients. This was rapidly implemented with the same AV platform used for the remote COVID patient assessment function (Fig. 3).
The combined telehospitalist functions and modifications over the PI cycle discussions to date are summarized in Table 1. The utilization/volume data for some of the telehospitalist functions are summarized in Figure 5A (AV assessments) and B (interventions). The volume of AV assessments coincides with high inpatient COVID census and also with high acuity of patients on the general medical ward.

Summary of Quality Improvement Cycles and Associated Service Modifications
IPC, infection prevention and control; LMWH, low molecular weight heparins.
Discussion
We report our experience of rapidly planning, implementing, and adapting a novel telehospitalist service in the setting of the COVID-19 pandemic with basic and easily obtained technology. A telehospitalist service line can be set up and adapted to settings without an existing telemedicine infrastructure. Key stakeholders that need to be activated early on in the planning stages are IT representatives to address hardware, software, and IT support issues, hospitalist medicine leadership to arrange for staffing of the service, nursing leadership to plan for nursing education of nursing-related workflows, quality improvement representatives to plan and direct the ongoing PI of the service as well as environmental services leadership to establish a physical operations setup if not yet in place. A multidisciplinary workgroup consisting of patient logistics, hospitalist medicine, IPC, and patient experience teams is essential to build the consensus workflows that form the basis of team communication and workload sharing. The main components to set up mobile and flexible videoconferencing capabilities are basic tablets equipped with camera, speaker, and microphones (i.e., iPADs [Apple Corp, Cupertino, CA]) that are placed in robust wheeled enclosures to protect the equipment from damage and unauthorized use and also to enable medical-grade cleaning procedures between uses. The counterparts for AV conferencing can be a paired mobile unit (Fig. 4B) or any desktop computer or smartphone equipped with a Health Insurance Portability and Accountability Act of 1996 (HIPAA) secure videoconferencing application. The telehospitalist communications to the various multidisciplinary team members (as depicted in Fig. 6) can efficiently be performed either through texting or through bilateral or conference phone calls. Principally the telehospitalist can work from either a central telemedicine hub, which often will facilitate communications, or they can work from home through HIPAA compliant remote connections.
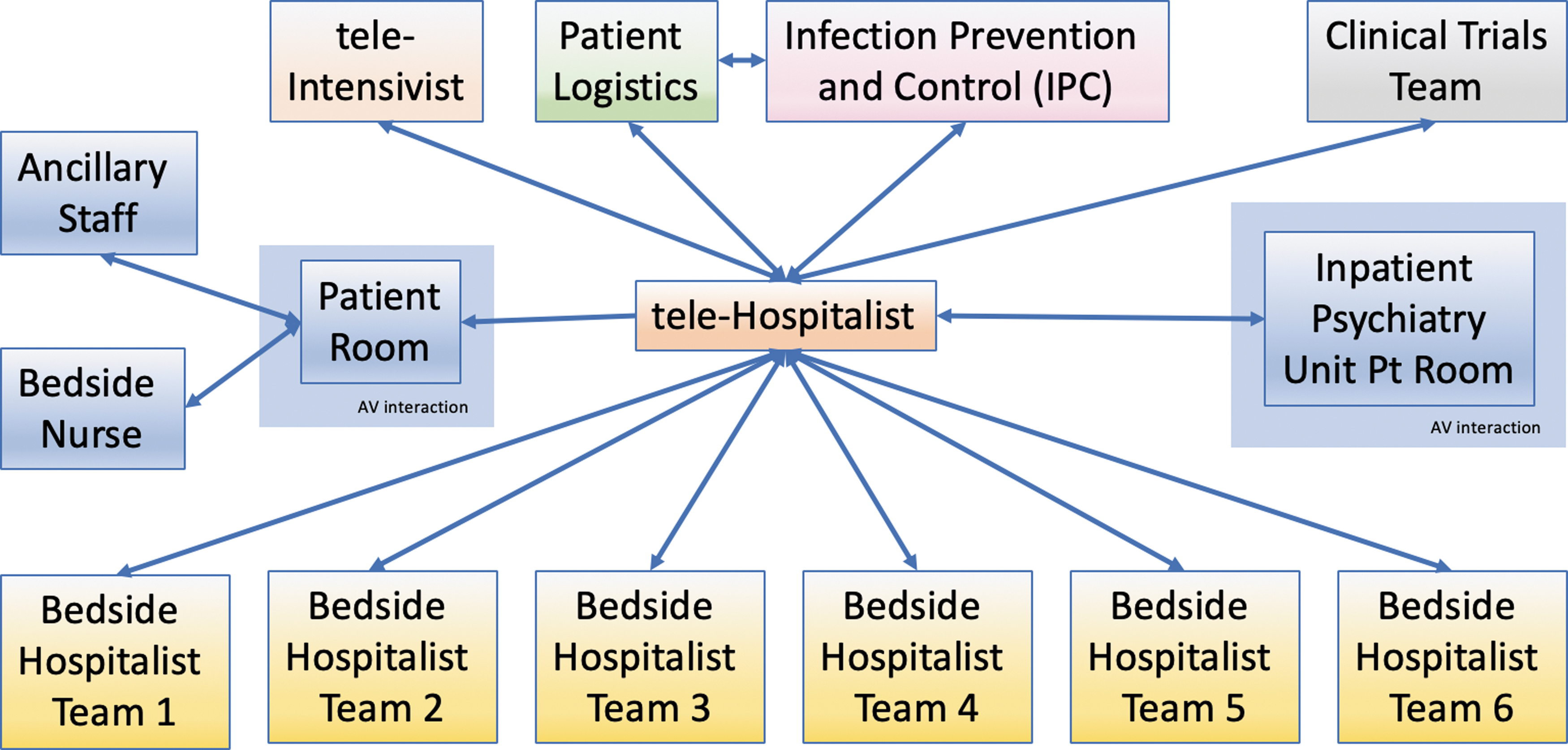
Organigram of telehospitalist functions and other team interaction pathways. The telehospitalist and teleintensivist will communicate about patients whose care levels change between ICU level and general medical ward level care. The internal medicine consultation service for inpatient psychiatry patients with COVID-19 who were cohorted in a newly sequestered psychiatry unit was targeted to reduce provider exposures and increase efficiency.
A telehospitalist service can be set up in settings without existing telemedicine infrastructure, but having an existing telemedicine infrastructure in place, including a clinical e-health center with administrative and IT support functions as well as experience in technical setups and implementing new telemedicine services may allow for a faster implementation.
Our hospital system is located in the U.S. epicenter of the pandemic. The expected early and rapid influx of large number of COVID-19 patients necessitated an accelerated planning and implementation process. A recent perspective piece in the New England Journal of Medicine pointed out that “…no telemedicine program can be created overnight,….” 11 The urgency of the growing pandemic and anticipated resource strain for us accelerated every step of planning, implementation, and iterative adaptation of this new service. Although the technical setup is comparatively straightforward, we found that it is extremely important to establish well thought-out consensus workflows that all members of the multidisciplinary team get repeatedly educated and updated on Campbell. 12
Recruitment of board-certified providers to serve in the role of telehospitalist was crucial. The best fit will undoubtedly vary from institution to institution: in this case a combination of providers with reduced clinical workload due to closure of elective services and a reallocation of providers at increased risk for complications of possible SARS-CoV-2 infections, that is, pregnant providers, providers with medical comorbidities, immunosuppressed providers, constituted the telehospitalist workforce.
One factor that was surprising was the large number of initial equipment issues related to rapid set up of AV units on different medical wards. In retrospect, the similarity between our AV unit setup and entertainment iPAD devices (Fig. 2) might have led to inappropriate use attempts or repurposing attempts by patients, including repurposing the wall charger for the iPads for personal phones, leaving the AV units unplugged losing charge. We remedied these issues with prominent warning stickers aimed to clarify that the AV units are medical equipment and not to be tampered with, and also by supplying patients with phone charger upon request. When sufficient number of AV units were available, the pairing of AV units inside and outside of the patient rooms significantly increased both stability of the system and utilization and satisfaction rates of the staff due to convenience.
It is important to decipher whether and how the new service added clinical value. In our assessment, the main drivers of value were fourfold:
First, the service added to patient safety and care standardization in times of high provider strain (clinical best practices, correct isolation, and cohorting practices).
Second, the service performed clinical workload balancing functions for the bedside teams, reducing provider exposure(s).
Third, the setup of the service with frequent improvement intervals allowed for rapid adaptation to changing conditions. For example, increasing number of COVID-19–positive psychiatric inpatients necessitated the opening of a designated COVID psychiatric inpatient floor. Given the high percentage of medical comorbidities for these patients, a telehospitalist consultation service for these psychiatric inpatients was able to be implemented in a matter of days, including workflow development and education of all involved providers.
Lastly, the service allowed for effective and standardized communication patterns between a number of different teams (Fig. 6).
We can summarize the centralized telehospitalist functions as follows:
Periodic AV monitoring of patients deemed at risk of deterioration
Serving as communication link between patient placement team, IPC, and six different COVID hospitalist teams
Supervising best clinical practices (VTE prophylaxis, EKG/QTc monitoring, and isolation status)
Maintaining a central COVID patient log as shared resource
Optimizing bed utilization by appropriate cohorting of patients in collaboration with PP and IPC
Providing telemedicine consultations to psychiatric inpatients on dedicated COVID psychiatry floor
Expediting identified hospital discharges
Facilitating family communication in collaboration with the different bedside COVID hospitalist teams and the patient experience team
Following up on COVID patients after hospital discharge to ensure continued recovery and communicate with primary care team for increased continuity of care.
Even though it was born out of the specific COVID-19 challenge, we plan to continue this centralized telehospitalist service beyond the pandemic as we are convinced that it adds value through improved clinical synergies and increased patient safety, especially if combined with ongoing periodic PI cycles, which will maintain task flexibility.
Conclusions
Centralized telehospitalist support functions can be rapidly deployed in crisis situation(s) and can be sequentially modified to best suit rapidly evolving and changing needs. Our telehospitalist service was developed to optimize clinical best practice performance, support bedside team providers, limit provider exposure, coordinate communication between teams, and extend consultation services to nonmedicine inpatient floors.
Footnotes
Authors' Contributions
All authors participated in the writing process. C.B. conceptualized and prepared the article draft. L.F., L.G., B.N., and C.S. reviewed and edited the article. All authors approved the final article.
Disclosure Statement
The authors confirm to have read BioMed Central's guidance on competing interests. All authors declare not to have any competing interests in the article.
Funding Information
No funding was received for this article.